Introduction
The menisci play a vital role in load distribution, shock absorption, joint lubrication and proprioception, and stability of the knee joint.1–3 Regularly engaging in everyday minor mobility tasks, meniscal tears are among the most frequently diagnosed orthopedic injuries, with an estimated occurrence of around 60 per 100,000 people.2–5 This increase is largely attributed to the growing engagement in different sports activities.5The sports with the highest percentages of meniscus tears were football (19%), wrestling (13%), and rugby (9%).6 Given their high prevalence among the general population, they may pose a potential economic problem as well.7,8 Arthroscopic meniscal repair and meniscectomy have traditionally and most commonly been the treatment of choice. Over the past years research work aimed at more conservative approaches for the treatment of meniscal injuries and new therapeutic strategies. In this context, various biological options have arisen to alleviate pain and enhance functional abilities; most importantly of which is platelet-rich plasma (PRP).1,9
Platelet-rich plasma (PRP) is an autologous blood product obtained through the centrifugation of whole blood, therefore increasing the concentration of platelets up to 3 to 6 times higher their baseline values.10 The natural healing role of platelets in physiological processes has sparked the development of various research fields around their use as the primary therapy for different musculoskeletal conditions, particularly cartilage pathologies.11,12
Platelets along with growth factors which are platelet-derived growth factors (PDGFs), transforming growth factor b1 (TGF-β 1), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), insulin-like growth factor 1(IGF-1), or fibroblast growth factor (FGF) play a critical role in cell proliferation, chemotaxis, cell differentiation, and angiogenesis.1,9,13 PRP is a simple, efficient, cost-effective, and safe (due to its autologous origin) solution treatment that has gained considerable interest in the management of orthopedic injuries.1,9
The use of PRP has been applied in several instances following meniscus tear surgeries. Overall, its use has been established in the literature; however, a proper comparison of the effects of PRP following meniscal repair surgeries remain an area that needs further exploration. The aim of this review is to showcase the current literature regarding the clinical and functional outcomes of patients with meniscal injuries treated with intra-articular PRP injections.
Methods
The keywords ‘meniscal tear’, 'meniscal repair, ‘degenerative tea’, ‘ramp lesion’, combined with “AND” for ‘Platelet-rich plasma (PRP) therapy’ OR ‘PRP treatment’ OR ‘PRP injections’, were searched in the database PubMed, Medline, and EMBASE. Our search initially pooled over 190 articles. Then, we focused on choosing high evidence papers as reviews, randomized clinical trials, meta-analysis, and cohort studies that were published between 2016 and 2023. Animal studies and case reports were excluded. Thus, 48 articles have been selected after a thorough evaluation of the search findings. Screening of the titles and abstracts was done to determine the articles relevant to the topic, and a more extensive reading was undertaken to fine-tune the selection, ending up with 35 articles being selected.
Results
The following paragraphs provide a detailed overview of the study results mainly depending on different scores.
Each score elements was summarized in Table 1.
Studies with follow-up of less than 1 year
In a case series of 38 patients with a mean follow-up period after PRP therapy of 75.92 ± 31.7 days, Medina-Porqueres et al. reported a significant improvement in the total KOOS score (i.e., 41.89 ± 22.89 baseline and 85.94 ± 13.5 post-treatment, p = 0.000).21 Moreover, it was also reported that no treatment-related adverse effects were reported, as also emphasized by other studies, such as pain, swelling, or any side effects because of the injection.21,22 Mitev et al. similarly showed statistically significant improvement in knee symptoms and daily activity using the Tegner Lysholm Knee Scoring Scale (TLKSS) score in 126 patients with degenerative meniscus lesions and cartilage injuries after 3 months and 6 months of follow up (i.e., TLKSS: 61.9 ± 7.4 baseline, 83.5 ± 4.6 post- 3 months, 83.4 ± 4.3 post- 6 months, p = 0.00065).23 Guenoun et al. also showed the same trend in knee symptoms and daily activity progression using the mean KOOS score in ten participants with degenerative meniscus tears without osteoarthritis according to Stoller classification after 3 months and 6 months of follow up (i.e., KOOS: 56.6 ± 15.7 baseline, 70.2 ± 16.8 post- 3 months, 72.7 ± 18.5 post- 6 months, p = 0.0007).9 Moreover, all athletes who underwent PRP injection managed to return to training or daily sports activity. In addition, patients’ MRIs after 6 months displayed a stable meniscus. Furthermore, a retrospective study on 30 patients of mean age of 13.93 years (12 - 17) with isolated meniscal tear showed a significant improvement of knee symptoms and daily activity according to Lysholm score 3 months after the PRP injection: from 3% of the patients having a “good” score to 76.7% of the patients having “excellent” and “good” outcomes after treatment13.
Chirichella et al. mentioned a study conducted by Blanke et al. of ten athletes diagnosed with grade II intrasubstance meniscus lesions via MRI who underwent percutaneous intra-meniscal injections of PRP and were followed up after 6 months.24,25 The average pain NRS- score significantly improved from 6.9 to 4.5 after treatment (p = 0 .027). Moreover, 60% of patients reported an increase in sports activity compared to that before PRP injection. In addition, 90% of patients first experienced short episodes of heavy pain at the injection site which was supported by Guenoun et al. as well.9
Studies with follow-up of more than 1 year
At longer follow-up periods, no significant differences were found between the PRP group and non-PRP group on Lysholm score, Ikeuchi grade, and Visual Analog Scale (VAS) for pain at the last follow-up, as reported by numerous studies.4,26–28 Most patients were evaluated at baseline (the day before surgery) and then 12 and 24 months after the last injection.
Other domains were also investigated in several of the included studies including the risk of meniscal repair failure (vertical, horizontal, radial, and root). Zaffagnini et al. reported this in a systematic review and meta-analysis of 5 studies with a total of 286 patients of an average age of 33.2, where they highlighted the difference between the PRP augmentation group and the control group at 35.7 months mean follow-up period: 9.9% (4.5%-19.1%) versus 25.7% (12.7%-38.7%) (OR= 0.31; 95% CI, 0.14-0.69; P < .0005); I2 < 50.29 Trams et al. added a double bind, placebo-controlled RCT of 72 patients with a mean follow-up of 92 weeks (54 - 157 weeks) to the latter’s meta-analysis which yielded similar results.2,30 In addition, he investigated the effect of PRP injection on the symptoms and daily knee activity function using the IKDC scores which yielded no statistically significant difference between the PRP group and control group. This is also supported by Migliorini et al. who assessed on top of IKDC, the VAS, and Lysholm scores.31 The rate of revision and rate of failure was not statistically significant although including one additional study by Trams et al.30,32 A retrospective matched case-control study of 324 patients who underwent ACL reconstruction with meniscus repair (PRP vs control age: 91.6 ± 11.2 vs 92.4 ± 10.6) showed no significant difference in IKDC scores nor in the timing of return to activity nor postoperative complications among the intraoperative PRP injection group and the control group after 2 years33 In addition, Bailey et al. reported a higher rate of postoperative knee motion loss compared with the control group (13.6% vs 4.6%; P < .001).
Discussion
Vascularization of the menisci
The vascularization of the menisci is critical for optimal function, stability, and biomechanical activity. Adequate blood supply is essential to maintain an optimal supply of nutrition, immune cells, and oxygen to the menisci, in exchange for accumulated waste products. As a result, diminished or inadequate supply can have a direct impact on the integrity and strength of the menisci, resulting in a variety of difficulties such as inappropriate stability, weight balancing, or smooth articulation during movement. These concerns can subsequently result in increased discomfort, poor gait, and limited daily activity in patients, especially those with underlying knee conditions such as osteoarthritis.
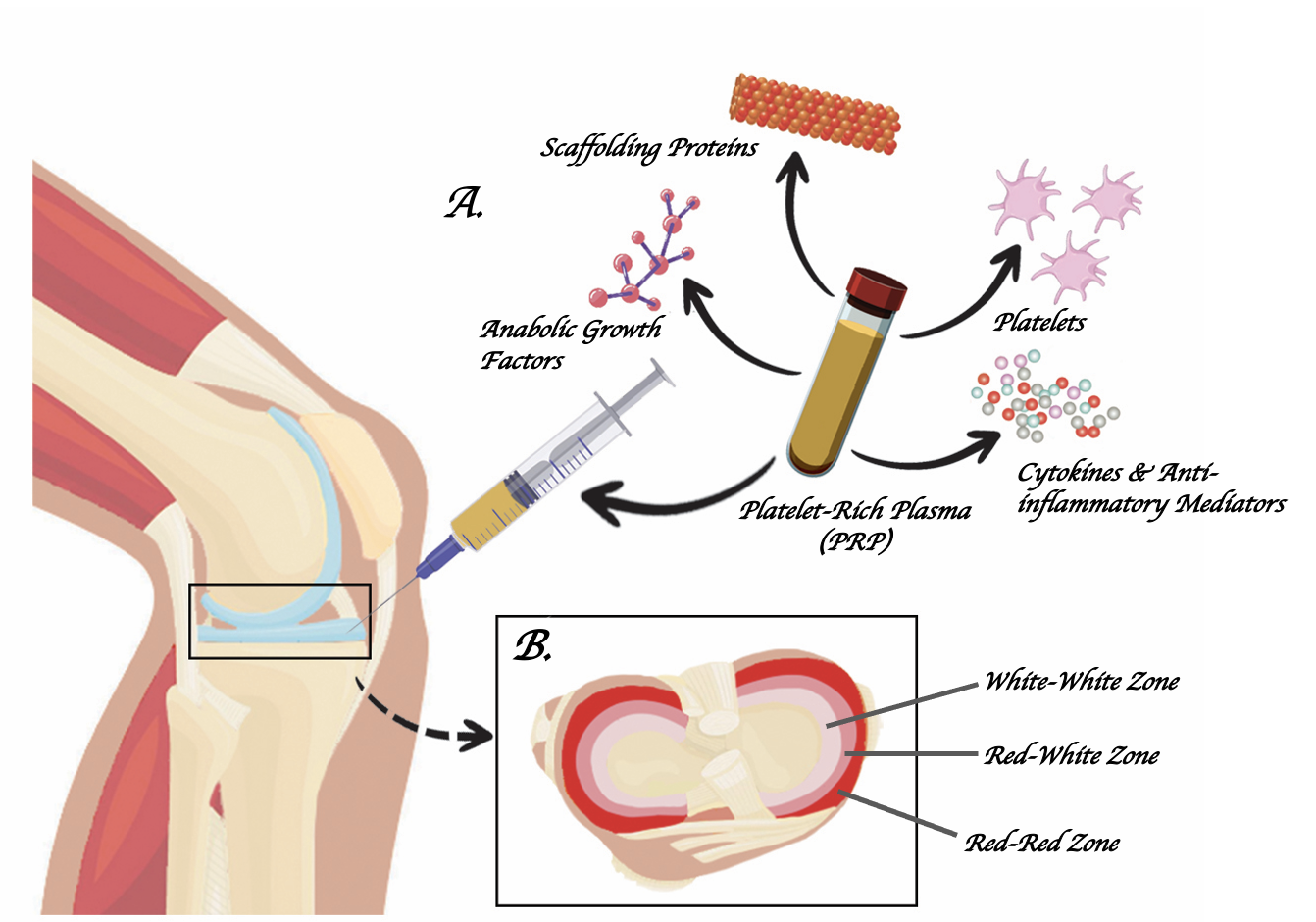
During development, the vascular supply of the menisci varies with different developmental stages. In the prenatal period, the entire meniscus is vascularized and becomes more and more localized as the knee matures.34 By adulthood, the periphery of the meniscus becomes the region that is concentrated with blood supply, while the inner areas become completely avascular. This led to visible segregation between the different zones of the meniscus, with the peripheral vascularized zones being the “red-red”, the inner avascular region as the “white-white” zone, and the area in between as the “red-white” zone.35 Given the importance of blood supply on healing, injuries to the more peripheral regions of the meniscus, or the red-red zone, tend to heal significantly better than those to the inner meniscus. Current guidelines in treatment recommend preserving and maintaining the structural integrity of the meniscus whenever possible; however, given the limited vascular supply to the inner meniscus, and hence healing abilities, injuries there usually require resection of the damaged tissue.36,37
Platelet-rich plasma action
PRP therapy aims to aid meniscal healing in 3 ways: through its anabolic growth, anti-inflammatory, and scaffolding effects.11 As such, PRP constituents include growth factors for anabolism, inflammatory mediators, and fibrinogen.11 Megakaryocytes produce platelets as anucleate cells. Growth factors (GF), coagulation factors, adhesion molecules, cytokines, chemokines, and integrins are all stored in platelets (Figure 1). After activation, platelets in PRP can release a variety of growth factors, including transforming growth factor (TGF), platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), basic fibroblast growth factors, vascular endothelial growth factor (VEGF), epidermal growth factors, and many others.38 Platelets in PRP also contain inflammatory mediators and modulators. Platelets can produce a variety of anti-inflammatory cytokines, including IL-1 receptor antagonist (IL-1ra), soluble tumor necrosis factor (TNF-R) I and II, IL-4, IL-10, IL-13, and interferon.11 Unlike serum, plasma contains fibrinogen and other clotting factors that, when activated, form a temporary fibrin scaffold that allows attachment, adhesion, migration, and proliferation of cells.39 Studies have shown some chondroprotective and proliferative effects of PRP, as per Spreafico et al. and others, whose experiments also revealed increased activity of Sox9 and aggrecan when stimulated by PRP.40 These in-vitro observed changes have been shown to be related to improved chondrocyte re-differentiation.

Complications
Most studies in the literature reported no local adverse events after PRP injection such as knee pain, erythema, or locking.1,4,21,22 However, it is worth mentioning that some studies reported pain at the site of injection and knee pain which could have been induced by an overload of volume due to lack of absorption by the damaged meniscus.9,25 Other sources attributed the pain to leukocytes in PRP. This might explain the lack of pain after PRP injection in most studies, especially the ones using leukocyte poor PRP. Leukocyte filters should be considered in the preparation of PRP to prevent such adverse events.
The debate over the use of PRP injections in meniscal repair arthroscopy is still ongoing due to major heterogeneity in the PRP preparation, laterality, type, and location of injury.41 Different dosages and constituents of PRP whether it is rich or poor in leucocytes affect the healing process. Moreover, it is known that the meniscus anatomy is divided into three zones which have different degrees of vascularization (red-red vascularized zone vs. white-white avascular zone vs red-white transition zone). Therefore, the location of the meniscal tear might also affect the healing of the meniscal tear. Other factors such as the laterality of meniscus (medial vs lateral) or type of meniscal tear (bucket-handle, longitudinal, horizontal, complex, undersurface, and radial) could contribute to the process of healing Field.42–44 Hence, standardization of PRP preparation and minimization of heterogeneity are crucial to drawing credible conclusions. Regarding meniscal repair with concomitant ACL reconstruction, no evidence supports the administration of PRP as it leads to no significant difference.30
Failure rate
PRP has become popular in sports medicine due to its ability to improve the healing capacity of wounded tissues. It is believed to increase efficiency and clinical results when paired with arthroscopic surgery. Most studies reported a decreased failure rate in arthroscopic isolated meniscal repair augmented with PRP injections.29,30,44,45 Administration of growth factors holds the potential to initiate a cascade of events leading to the activation of meniscal chondrocytes and the promotion of regenerative processes. Platelet-derived formulations exhibit a rich reservoir of bioactive agents and cytokines, including interleukin 1 (IL-1), transforming growth factor beta (TGF-β), platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), insulin-like growth factor 1 (IGF-1), hepatocyte growth factor (HGF), and basic fibroblast growth factor (β-FGF).46,47 These bioactive constituents play a pivotal role in angiogenesis, chemotaxis, the assembly of extracellular matrices, and cellular proliferation. Thus, PRP injections are hypothesized to expedite the reparative trajectory and enhance the regenerative potential across all zones of the meniscus.48 The therapeutic utility of PRP in the context of cartilage regeneration has garnered significant recognition, attributed to its capacity to mitigate catabolism while concurrently amplifying the anabolic milieu within the hyaline cartilage environment.31
Differences in Rehabilitation protocols
Rehabilitation therapy aids in the reduction of swelling, and pain, and in restoring knee function.
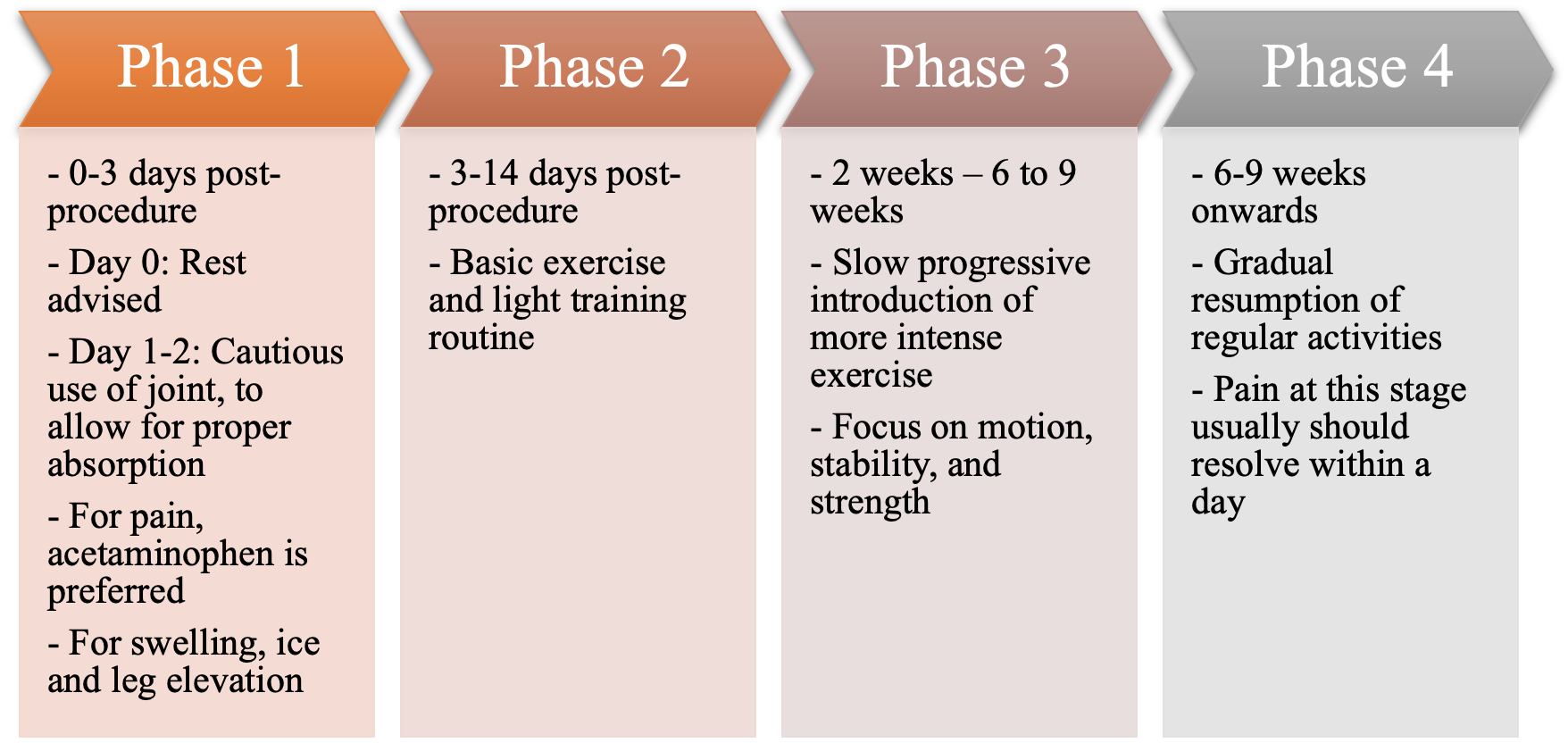
Chicago stem cell therapy and regenerative medicine reports that rehabilitation protocols after PRP injection consist of 4 phases and are over 9 weeks following the procedure49 (Figure 2).

PRP Recovery Stages following PRP injection
The patient can leave the clinic right away, but resuming a routine isn’t immediate. Phase 1 spans 0-3 days after the procedure on the procedure day, complete rest is advised. For the subsequent two days, the treated area ought to be used sparingly to enable proper platelet absorption in the joint. Immobilization aids like slings or walking boots might be necessary to minimize movement while safeguarding the treated joint. Patients should avoid using NSAIDs for at least 2 weeks after the injection, yet they can take acetaminophen for any pain that arises. As for the management of any swelling, it is advised to apply ice and elevate the leg. Phase 2 of rehabilitation consists of days 3-14 after the procedure.
During this phase, exercise routines are kept basic, such as alight activities like yoga and weight-bearing exercises. Activities stressing the treated joint; however, should still be avoided. During phase 3, from 14 days to 6-9 weeks after the procedure, the patient can gradually reintroduce lifting, stretching, cardio, and similar exercises. Their physician may guide them through therapeutic exercises to regain motion, strength, and balance. Finally, in Phase 4, approximately 6-8 weeks post-procedure, the patient might resume their regular activities. Some lingering soreness in the treated joint could occur, but this should typically subside within a day.
On the other hand, according to Massachusetts General Hospital guidelines for Rehabilitation Protocol for Arthroscopic Total Meniscal Repair, there are 6 phases of rehabilitation that a patient should follow for more than 26 weeks (6 months) post procedure.50,51 The protocol for Arthroscopic Partial Meniscectomy is of 4 phases and over 9 to 12 weeks.51
This shows that the rehabilitation protocol for PRP is less in duration, and this might be considered in the patient’s preference if the two options can be done.
Return to Sports
Returning to sports after platelet-rich plasma injection is earlier than that of arthroscopy according to rehabilitation protocols.49 PRP might be promising for athletes with meniscal tears. A randomized clinical trial was done on acute muscle tears and PRP injection. It proved to decrease the time to return to sports among the group who did PRP injection with physiotherapy compared to the control group that underwent rehabilitation alone. The average duration for returning to play was 21.1 ± 3.1 days for the PRP group and 25 ± 2.8 days for the control group (P = 0.001).49,52 This point might be of high importance to athletes.
Conclusion
In conclusion, platelet-rich plasma (PRP) may be regarded as a viable therapeutic option when conventional treatments fail, or even as an adjunct to traditional treatment. The published literature on the usefulness of PRP in treating meniscus tears addresses the role of this injection in providing faster healing and short-term recovery. Other factors that come into play when deciding on the use of PRP, particularly in the case of athletic patients, are personal preferences, the desire to adhere to the rehabilitation plan, and the cost of treatment. In terms of the sole use of PRP instead of traditional treatment, further high-quality studies ought to be conducted to assess this; most current studies show no significant difference, with some showing some inferiority against PRP, and others favoring PRP as the superior approach to managing meniscal injuries. Furthermore, more emphasis should also be placed on the long-term outcomes of patients who have undergone PRP injections, to provide a more holistic understanding of the expectations of this treatment.
List of the abbreviations
-
PRP: Platelet-Rich Plasma
-
MRI: Magnetic Resonance Imaging
-
ACL: Anterior Cruciate Ligament
-
NRS: Numerical Rating Scale
-
KOOS: Knee Injury and Osteoarthritis Outcome Score
-
TLKSS: Tegner Lysholm Knee Scoring Scale
-
VAS: Visual Analog Scale
-
SF-36: RAND-36 (Short Form 36)
-
IKDC: International Knee Documentation Committee
-
IL: Interleukin
-
TGF-β: Transforming Growth Factor Beta
-
PDGF: Platelet-Derived Growth Factor
-
IGF: Insulin-like Growth Factor
-
VEGF: Vascular Endothelial Growth Factor
-
EGF: Epidermal Growth Factor
-
β-FGF: Basic Fibroblast Growth Factor
-
NSAIDs: Non-steroidal anti-inflammatory Drugs
Authors’ Contributions
Both authors AEZ and JY equally contributed to the project. They participated in the concept of the study, doing the whole literature review, data extraction, and writing the different sections of the manuscript. AEZ worked on Figures 1 and 2, as well as table 1. MH participated in data extraction, writing the manuscript, its rigorous revision several times, and coordinated the flow of the work. EK helped in the brainstorming and literature review. MN is the corresponding author. He made substantial contributions to the concept of the study and followed up the work to ensure that it was original and complied with the research ethics and guidelines of this journal. MN also contributed to the development of the manuscript. All authors are accountable for all the contributions and integrity of the work. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Ethical review was not required because the study is a review of literature.
Consent for Publication
Not applicable
Availability of data and material
Not applicable
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Corresponding author
Mohamad Nassereddine, MD,
Division of Orthopedic Surgery, American University of Beirut Medical Center, Beirut, Lebanon
Email: mn103@aub.edu.lb