1.1. Introduction/Anatomy
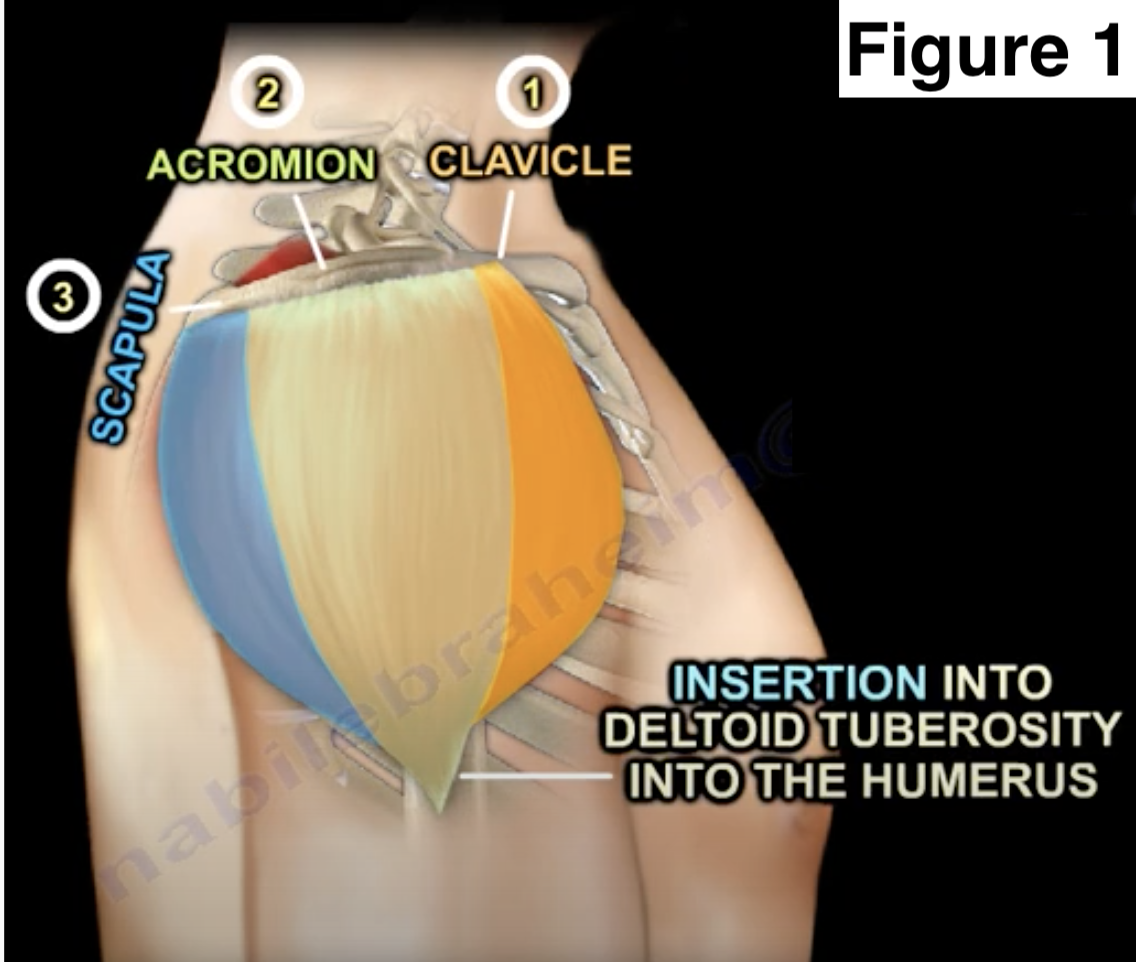
The deltoid muscle forms the rounded appearance of the shoulder. This external curvature of the shoulder is formed by the deltoid extending anterior to posterior as it encapsulates the glenohumeral joint. The bulk of the muscle sits between the acromion and the deltoid tuberosity of the humerus. The muscle is divided into three parts based on origin (Figure 1).

The anterior portion originates from the lateral one third of the clavicle, the acromial portion originates from the acromion of the scapula, and the posterior part originates from the spine of the scapula. Each of the three parts of the deltoid also perform a different function. The anterior deltoid flexes and medially rotates the arm, the lateral part abducts the arm, and the posterior part extends and laterally rotates the arm. All the sets of muscles fibers converge and travel distally to form a short tendon that insert at the deltoid tuberosity on the lateral aspect of the humerus.
The axillary nerve provides motor innervation to the deltoid and cutaneous sensory innervation over the shoulder.
The axillary nerve arises from the posterior cord of the brachial plexus and is one of the two terminal branches of the posterior cord, along with the radial nerve. The axillary nerve travels around the upper arm transversely from posterior to anterior approximately 7cm distal to the acromion. Axillary nerve injury may present as weakness of shoulder abduction, loss of sensation over the lateral aspect of the shoulder, and atrophy of the deltoid muscle. Deltoid atrophy can be visualized as a flattened curvature of the shoulder. The axillary nerve may be injured by shoulder fracture or dislocation as discussed in the following section.
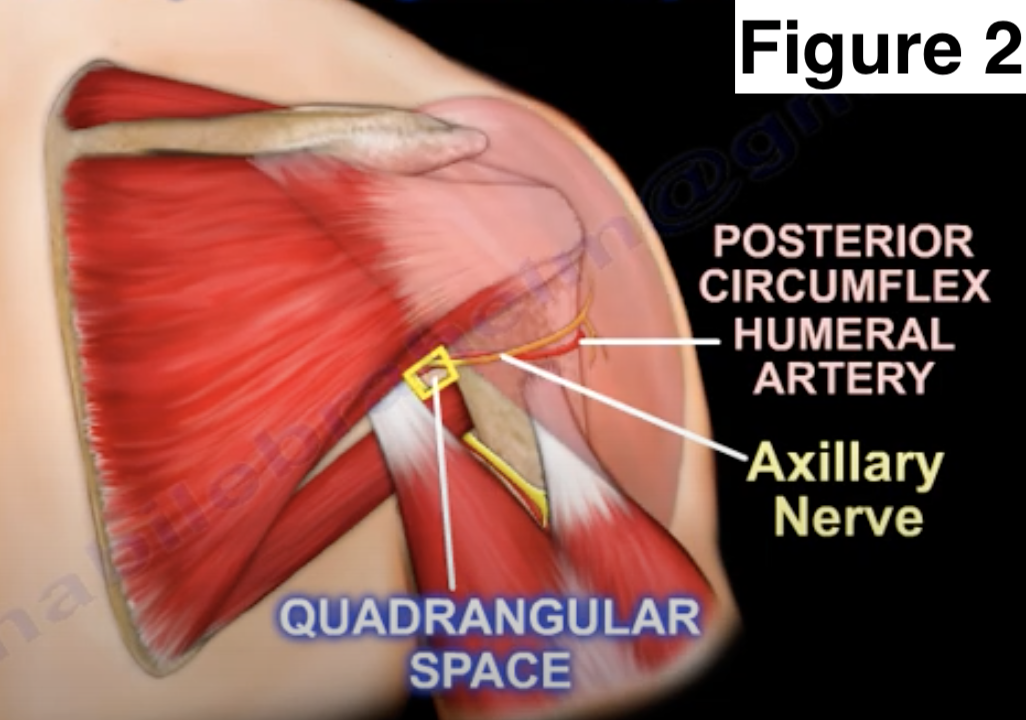
The deltoid muscle is supplied by branches of the axillary artery and the posterior humeral circumflex artery. The axillary artery provides the thoracoacromial artery; the deltoid branch of this artery supplies the anterior deltoid muscle. The posterior aspect of the deltoid receives arterial supply from the posterior circumflex humeral artery. Vessels of the deltoid muscle are anatomically associated with the quadrangular space (Figure 2).

The posterior circumflex humeral artery and the axillary nerve pass through the quadrangular space to supply the deltoid muscle.
1.1.1. Deficiency of the Deltoid Muscle
The deltoid muscle function can be compromised by axillary nerve injury, rupture of the deltoid muscle itself, or by iatrogenic damage to the muscle. Compromise of the deltoid muscle manifests as weakness in shoulder abduction. While the supraspinatus assists in initiation of abduction up to 15 degrees, the deltoid is responsible for shoulder abduction. If the patient is able to passively abudct the arm to 90 degrees, abduction beyond 90 degrees may be possible as this range is performed by scapular motion exerted by the trapezius and serrates anterior muscles. As there is overlap in muscles assisting with shoulder abduction, deltoid dysfunction can be tested by having the patient rest their hands on the iliac crest and perform shoulder abduction in the coronal plane. This should be performed with internal rotation of the shoulder and keeping the elbow flexed and forearm pronated. As the deltoid works in conjunction with muscles of the rotator cuff to perform abduction of the shoulder, rotator cuff pathology should be parsed from deltoid dysfunction. Conversely, the deltoid muscle compensates for deficiency of neighboring muscles in patients with rotator cuff pathology.1,2
The axillary nerve is commonly injured by shoulder fracture or dislocation. Shoulder dislocation can result in brachial plexus injury in 5%-60% of patients depending on mechanism of injury and patient demographics. Of these brachial plexus injuries, the axillary nerve is most commonly injured.3 Suspect an axillary nerve injury if the patient has loss of shoulder adduction and deltoid tone as well as decreased or absence of lateral shoulder sensation. If a patient experiences loss of abduction after shoulder dislocation, one must also rule out an acute rotator cuff tear. It is important to check the sensation over the shoulder area as this will differentiate a rotator cuff tear from an axillary nerve neuropraxia. Loss of sensation to the skin over the lateral shoulder is the best test to rule out axillary nerve palsy. Injury to the axillary nerve varies from mild neuropraxia due to neurotmesis (complete disruption) of the nerve. Axillary nerve injuries are treated conservatively with an arm sling for comfort and physical therapy. The patient’s progress can be assessed with EMG and nerve studies three months after injury, where biphasic waveforms will indicate nerve recovery. If the nerve fails to recover, fibrillation potentials and p waves will be present on EMG. Failure to abduct the shoulder after 4-6 months despite physical therapy suggests intact rotator cuff muscles have failed to compensate for the lack of deltoid function.4
Damage of the deltoid musculature itself can also result in dysfunction. The muscle may rupture as a result of sports or occupational trauma. Complete rupture is rare and only seen in the setting of extensive rotator cuff pathology. More commonly, deltoid rupture is secondary to iatrogenic injury. Detachment of the deltoid to any of its three origins at the clavicle, acromion, or scapula, can occur during open shoulder surgery with underlying os acromiale. Patients with os acromiale have failure of fusion in the secondary ossification centers of the acromion. While this may present with pain, most patients are asymptomatic. Symptomatic patients can be treated with arthroscopic subacromial decompression and acromioplasty, or a two stage fusion to first fuse the deformity and then perform acromioplasty. These methods are preferred over open surgical treatment as open procedures have a higher risk of deltoid detachment at its acromial origin.5,6
1.1.2. Clinical Considerations
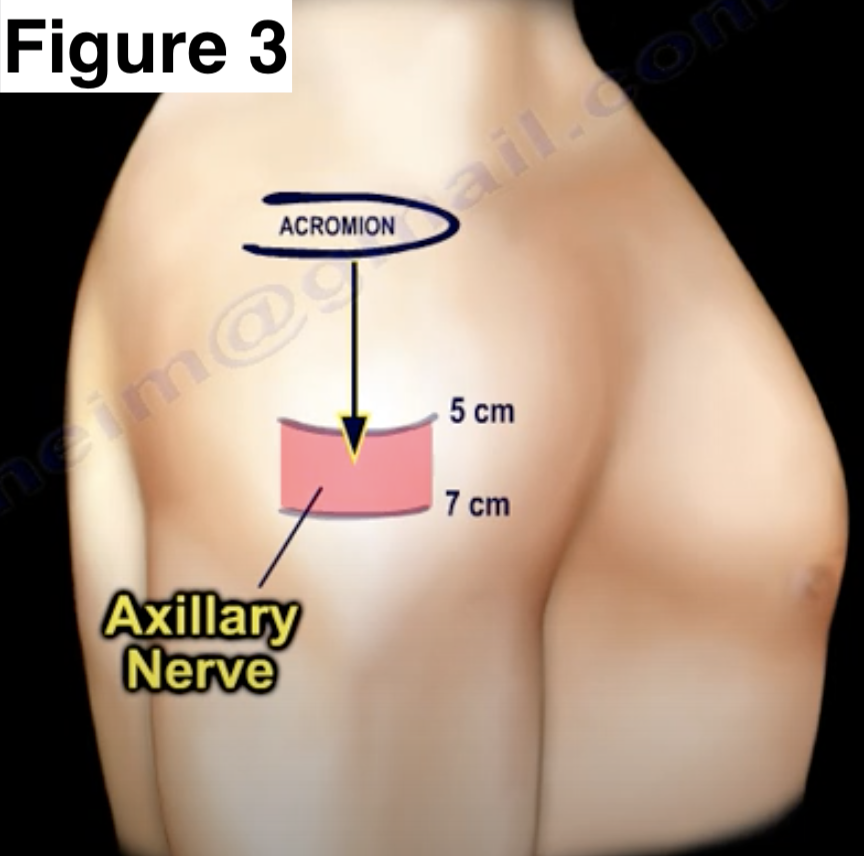
The integrity of the deltoid muscle must be maintained during lateral approach to the shoulder. A lateral deltoid splitting approach may be used for rotator cuff repairs or to access the proximal humerus and is performed by extending an incision distally from the tip of the acromion. If fixation of the proximal humerus is needed, an additional anterolateral incision over the humeral shaft may also be used. In either case, the incision must not be extended more than 5-7cm distal to the acromion as this may damage the axillary nerve as its travels transversely at this level from posterior to the anterior arm (Figure 3).

If this region of the axillary nerve is avoided, the lateral deltoid splitting approach is otherwise a reliable and less invasive alternative to open procedures.7
The deltoid muscle must also be considered when performing intramuscular injections. The injection should be placed in the lateral portion of the deltoid approximately 3-5cm distal to the acromion. Injections more proximal to this level can enter the shoulder capsule or joint while injection more distal risks axillary nerve injury. Upper arm injury related to vaccine administration can involve damage to the deltoid and axillary nerve as well as the radial nerve or subacromial bursa. Proper training of vaccine administration and abducting the arm to 60 degrees by instructing the patient to place their hand on the iliac crest also promotes safe injection.8
1.1.3. Conclusion
Careful evaluation and knowledge of the deltoid muscle and deficiency of the deltoid muscle is necessary in order to properly identify and treat it. Treatment options include intramuscular injections or surgical intervention in order to alleviate pain and restore functionality in patients.
Corresponding author
Anderson Lee, Anderson.lee@rockets.utoledo.edu
Acknowledgements
None
Conflict of Interest
The authors have no conflicts of interest to declare.
Funding
The authors received no funding for this article.
Author Contributions
Phillip J. Stokey: Conceptualization, methodology, investigation, writing-original draft, writing-reviewing & editing, resources, data curation, project administration, supervision
Sargampreet Kaur: Methodology, writing-original draft, data curation, writing-reviewing & editing
Anderson Lee: writing-reviewing & editing
Kyle Behrens: resources, writing-original draft, writing-reviewing & editing, supervision
Nabil Ebraheim: Conceptualization, writing-reviewing & editing, project administration