

INTRODUCTION
Proximal humeral fractures account for 4-5% of all fractures.1 Osteosynthesis in grade IV-VI of Neer classification complex fractures; elder patients with more than 40% of articular surface defacement and coexisting osteoporosis often result in limited shoulder activity and high risk of avascular necrosis which leads to impaired shoulder function.2 In the context of traffic accidents still being a serious problem in Southeast Asia. Based on the report of the ASEAN Regional Road Safety Strategy in 2016, the biggest risk faced by most ASEAN countries is traffic accidents.3 In the context of traffic accidents in Vietnam still being high, the rate of people using two-wheeled vehicles is up to 95%, facing the increasing challenge of returning to daily activities after injury, in major hospitals we have initially applied shoulder hemiarthroplasty to treat the complex proximal humeral fracture and this surgery has become routine at Viet Duc Friendship Hospital for many years. We conducted this study to describe the clinical and radiographic characteristics of complex proximal humerus fractures and evaluate the results of shoulder hemiarthroplasty for this type of fracture at Viet Duc University Hospital, provide information on the specific features of patients undergoing shoulder joint replacement in Vietnam and contribute additional insights into this surgical approach for the global medical literature.
MATERIALS AND METHODS
MATERIALS
78 patients with complex proximal humeral fractures underwent shoulder hemiarthroplasty at Viet Duc University Hospital from 1/2017 to 12/2021.
Inclusion criteria
Patients diagnosed with fractures of the proximal humerus are classified as Neer types IV, V, VI; damage to humeral head cartilage surface > 40% of the joint surface (on computed tomography with 3D reconstruction) in patients aged 60 or older. Patients falling into Neer type VI, with comminuted fractures (3 or 4 fragments) in those under 60 years old, or patients with osteoporosis. The patient participated in post-operative rehabilitation from the first day and followed Wilcox’s 4-stage protocol.4
Exclusion criteria
Cases of proximal humerus fractures that failed with other treatment methods. Patients with shoulder joint degeneration, brachial plexus paralysis, and pathological fractures due to bone cysts or tumors.
METHODS
A retrospective, cross-sectional descriptive study.
Data collection: The protocol involves a review of the patient’s medical records, as well as a minimum of 3 months of postoperative follow-up care. Patients will be reevaluated at 3,6,9, and 12 months post-surgery, and then annually.
Data was analyzed by SPSS 20.0 software.
The general result was evaluated by Constant score.
RESULTS
General features
Traffic and daily-life accidents accounted for 53.8% and 43.6%, respectively; other causes were less common. In the group of patients younger than 60, the main cause of injury is traffic accidents (88%). In the group of patients older than 60 years old, the main cause of injury is daily life accidents (60.38%). In the group of traffic causes, it is mainly found in men, accounting for 54.76%. In the group due to daily life accidents, it was mainly found in women, 64.71%.
Diagnostic features
Clinical features
The right upper limbs are involved slightly more than the left with 52.6%. 45 patients were treated on the dominant hand, accounting for 57.7%. The patient’s dominant arm is more vulnerable to bone fractures. Sharp pain (100%), limited shoulder mobility (100%), subcutaneous hematoma (70.51%), upper limb deformity (57.69%), and abnormal movements (51.28%). Patients usually did not witness any associated injuries (93.59%). 5 cases had associated fractures.
The most common fracture was grade VI with 48 cases (accounted for 61.54%). 94 Group IV and V fractures had a lower rate with 23.08% and 15.38%, respectively. 95 There were 65 cases of three-part fracture (83.4%) which consisted of 18 cases of the 96 greater tuberosity and surgical neck fracture without head dislocation, which accounted for 23.1%; 12 cases of the lesser tuberosity and surgical neck fracture without head dislocation accounted for 15.4%. There were 35 cases of greater tuberosity fracture with surgical neck dislocation, accounting for 44.9%. Thirteen patients had four-part fractures, in which both tuberosities and the surgical neck were involved with or without head dislocation, accounting for 16.6%. In 38 cases (80.75%), the head was dislocated anteriorly while posterior dislocation was rare.
Short–term results
There were no complications.
100% primary wound healing rate.
Postoperative X-ray showed a normal axis in 94% of total cases.
Long-term results
Mean Constant score of the unaffected arm was 84.67 ± 7.85 while for the injured arm was 67.45 ± 13.20.
Postoperative pain: 74.4% of patients had no pain, 17.9% had mild pain, 7.7% had moderate pain and no patient suffered from severe pain.
Postoperative active shoulder mobility: the average flexion was 115.68 ± 20.36°; abduction was 99.81 ± 20.65° and external rotation was 37.14 ± 10.12°. The position of the hand placed in a posture of internal rotation forward flexion referenced by the buttocks, the sacrum, L3, T12, T7-8 accounted for 8.97%; 26.92%; 47.43%; 8.97%, and 7.71%, respectively.
No complications were recorded.
Return to work: 75.64% of patients were able to return to pre-injured life while 17.95% needed partial assistance and 6.41% needed daily life assistance. However, there is no patient required for special medical care.
DISCUSSION General Features
The female-to-male ratio is 1.17. Our results are lower compared to other studies: R. Castricini et al. (2000–2008): 13/15; Ph. Valenti et al. (2011–2015): 3/16; Antti P. Launonen et al. (2006-2010): 3/17; Passaretti D et al. (2016-2018): 3.4/18. The mean age was 64.26 (from 33–90). Our results are lower compared to other studies: G.
Kontakis et al. (2008): 67.7 years,5 CM. Court–Brown et al. (2001): 66 years,6 Iglesias-Rodríguez (2016–2018): 70.4 ± 12.2 years.7 From these findings, we found that the rate of humeral head fractures in men and women varies according to geographical region and living habits. Despite the gender ratio differences among authors, the commonality is that the fracture rate on the proximal humerus is higher in females than males, and the age group most susceptible to proximal humerus fractures is 60 years and older. This difference is related to postmenopausal conditions in females, including hormonal changes, metabolic disorders, physical activity history, and healthcare conditions. In a study by Van Staa TP et al., the lifetime risk of fractures for a 50-year-old woman was 53.2%, while in men, it was 20.7%. In normal individuals, bone is constantly undergoing a balance between bone formation (performed by osteoblasts) and bone resorption (caused by osteoclasts). However, in postmenopausal women, bone loss occurs at a faster rate than bone formation. On average, each year, there is approximately a 2% loss of cortical bone mass and a 9% loss of trabecular bone mass. The mechanism behind this phenomenon is linked to the decrease in estrogen levels after menopause. This reduction stimulates osteoclast activity through intermediaries such as Interleukin-1 and TNF, leading to an increased rate of bone resorption, resulting in a gradual decrease in bone density, making it more susceptible to fractures.
Characteristics of Injury Causes
Traffic and daily-life accidents accounted for 53.8% and 43.6%, respectively; other causes were less common. In the group of patients younger than 60, the main cause of injury is traffic accidents (88%). In the group of patients older than 60 years old, the main cause of injury is daily life accidents (60.38%). In the group of traffic causes, it is mainly found in men, accounting for 54.76%. In the group due to daily life accidents, it was mainly found in women, 64.71%. Antti Launonen et al. (2015) highlighted common causes of proximal humerus fractures, with falls while standing being the most frequent (89%), followed by traffic accidents (4%), falls from stairs (2%), and excessive physical activity (1%). The authors observed an age-related mechanism, with high-energy trauma like traffic accidents more prevalent in younger individuals, and low-energy trauma more common in older adults.8 Passaretti D et al. noted gender-based differences in injury causes. High-energy trauma (e.g., sports injuries and traffic accidents) is more frequent in males aged 18-60 (30.1%), while low-energy trauma (e.g., falls while walking, running, or at home) is more common in the over-65 age group. Similar patterns were observed in females.9 Sandra IglesiasRodríguez et al. found that the majority of high-energy traumas (73.9%) occurred in patients under 60 age, while only 20.7% of low-energy traumas were recorded in this age group.7 The results of the study show that young men often suffer complex proximal humeral fractures due to traffic accidents. The mechanism of injury is caused by strong, direct impact force, leading to serious injury. Therefore, in the study, there were patients even as young as 33 years old who were prescribed partial shoulder replacement surgery. While this injury, with daily life accidents, is common in older people, the rate in women is higher than in men. This is completely consistent with the socio-economic and transportation characteristics of Vietnam, a country with a developing economy, a young population, and a common means of transportation using motorbikes.
Diagnostic Characteristics
All patients exhibited signs of sharp pain and restricted shoulder joint movement. Hematoma and subcutaneous bleeding were observed in 70.51% of cases, limb deformity in 57.69%, and abnormal movements in 51.28%.
Characteristics of fracture groups according to Neer classification on X-ray
The most common fracture was grade VI with 48 cases (accounted for 61.54%). Group IV and V fractures had a lower rate with 23.08% and 15.38%, respectively. There were 65 cases of three-part fracture (83.4%) which consisted of 18 cases of the greater tuberosity and surgical neck fracture without head dislocation, which accounted for 23.1%; 12 cases of the lesser tuberosity and surgical neck fracture without head dislocation accounted for 15.4%. There were 35 cases of greater tuberosity fracture with surgical neck dislocation, accounting for 44.9%. Thirteen patients had four-part fractures, in which both tuberosities and the surgical neck were involved with or without head dislocation, accounting for 16.6%. In 38 cases (80.75%), the head was dislocated anteriorly while posterior dislocation was rare. Court-Brown et al. (on 1027 cases): Neer type IV, V, and VI fractures were reported as 21.24%, 9.86%, and 57.97%, respectively; three-part fractures constituted 55.53%, including 15.24% greater tuberosity fractures, 13.57% lesser tuberosity fractures, and 26.72% displaced fractures; four-part fractures constituted 44.47%, including 15.03% greater tuberosity fractures and 29.44% displaced fractures; three-part fractures with posterior displacement accounted for 0.1%, and four-part fractures with posterior displacement accounted for 0.1%.6 Kazuya et al. (on 509 cases): Neer type IV, V, IV-V, and VI fractures were reported as 55.32%, 2.84%, 17.73%, and 24.11%, respectively; threepart fractures constituted 60.76%, including 49.37% with greater tuberosity fractures and non-displaced neck, 3.80% with lesser tuberosity fractures and non-displaced neck, and 7.59% with displaced fractures; four-part fractures constituted 39.24%, including 31.65% non-displaced fractures and 7.59% displaced fractures14. Launonen et al. (on 174 cases): Three-part fractures constituted 73.6%, and four-part fractures constituted 26.4%.8 Zyto et al. three-part fractures constituted 62.96%, and four-part fractures constituted 37.04%.10 These findings highlight that three-part fractures are more common than four-part fractures, and posterior dislocation fractures are rare. Our study has a higher rate of group VI fractures than other authors in the world. The reason may be because the majority of accident mechanisms in our study group are due to traffic accidents, patients mainly travel by motorbikes, and high speeds cause high-energy injuries with the mechanism of falling with arms forward.
Diagnostic features
All patients had sharp pain and significant limitation of shoulder joint motion. Subcutaneous hemorrhage and hematoma were observed in 70.51%, limb deformity in
57.69%, and abnormal movement in 51.28% of cases. In the current study, we studied
18 cases of group IV fractures (23.08%), 12 cases of group V fractures (15.38%), and 48 cases of group VI fractures (61.54%). There is a resemblance between our results and those of a previous report by Court-Brown.8
Results
Shoulder joint function
According to our research, the mean Constant score of our patients was 67.45 ± 13.20, higher than the results reported by Ph Valenti (2017),11 and Castricini (2011).12
All patients received routine rehabilitation immediately after surgery and performed 220 instructed exercises continuously upon discharge, which significantly improved 221 shoulder function.
Shoulder range of movement
There was no significant difference between our results and those of many authors worldwide. Additionally, patients achieved a moderate level of upper extremity range of motion. During postoperative function tests, patients position their hand at head level in all elbow positions along the anteroposterior axis after surgery and touch the contralateral shoulder in both the front and back of the head successfully. Based on these results, we concluded that if patients were under the same improvable postoperative conditions and rehabilitation procedures compliance, the postoperative outcomes might be more pretended with better shoulder function after hemiarthroplasty.
Postoperative pain
In this study, most cases (74.4%) had no complaints about postoperative pain. Some patients had mild pain (17.9%), while only 7.7% reported moderate pain. None of the patients developed severe pain that required regular pain-relief therapy. Our results are also consistent with previous research conducted by Kontakis (2008),7 demonstrating the effectiveness of hemiarthroplasty in reducing pain associated with proximal humeral fractures.
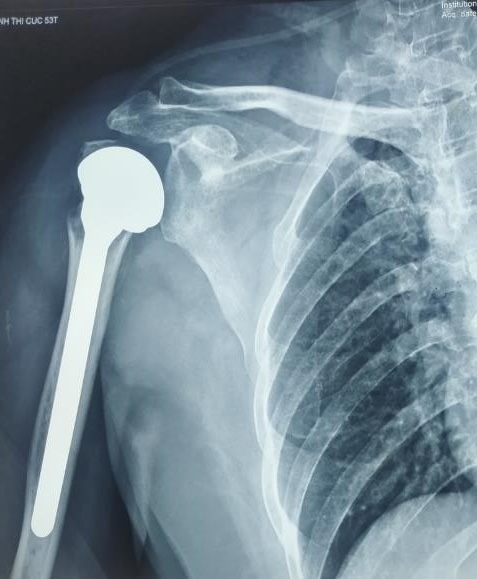
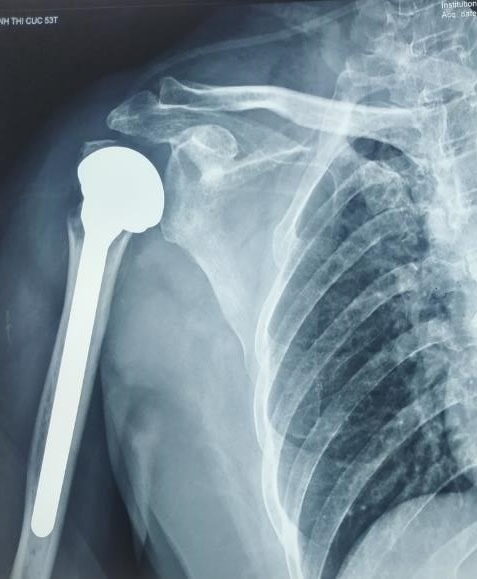
Image Illustration of Clinical Cases in the Study


CONCLUSION
In Vietnam, the most common cause of trauma is traffic accidents, often occurring in young males with complex proximal humeral fractures. Shoulder hemiarthroplasty is the treatment method for complex proximal humeral fractures: Neer type IV, V, VI fractures; damages to head humerus fractures > 40% of the articular surface in patients aged ≥ 60, osteoporosis ensuring good results and maintaining shoulder joint function.