
1. Introduction
Osteoarthritis, including knee osteoarthritis, is a common disease and one of the leading causes of disability in the elderly. The disease occurs in all countries, races and geographical regions. The disease is common in women and the elderly, the female/male ratio is about 2.5/1.1–6 Total knee replacement is surgery to remove damaged cartilage and replace it using artificial joints. Although the results are positive due to improvement in pain level, walking ability and knee function, some changes in knee biomechanics as well as complications of the patellofemoral joint lead to knee stiffness, instability, pain, patellar fracture and patellar tendon rupture. A common condition is patella baja.
This issue has been mentioned quite a lot in the literature. Koshino found that 65% of patients had patellar tendon shortening greater than 10% of its length, whereas Weale reported this rate to be 34%.7 Floren reported that 37% of patients had >5% patellar tendon shortening through the standard incision and 14% of patients had 10% shortening.8
Joint line changes are not uncommon, it can be seen in up to 40% of primary knee replacements, it is a result of soft tissue release, osteotomy of the distal femur, length of the artificial joints components. According to Kawamura and Bourne,9 the average joint line has changed by 3.5mm. This change according Sabbioni10 was 4mm, and Scuderi and Insall8 was 5.6mm.
We conducted this study to evaluate the degree of change in the position of the patella after surgery and the results of knee replacement surgery on the group of normal patella and patella baja.
2. Materials and Methods
2.1. Research subjects
The study was conducted on 58 patients with 62 knee joints diagnosed with knee osteoarthritis, who were assigned to have total knee replacement surgery at Saint Paul General Hospital from January 2018 to February 2020. The selection criteria included patients who are clinically evaluated and have imaging diagnostics with a diagnosis of grade III and IV knee osteoarthritis and a small degree of misalignment (varus < 30º, valgus < 20º), who have eligible for surgery. Exclusion criteria included knee replacement patients, incomplete medical records, and patients who did not agree to participate in the study.
2.2. Research methods
Patients eligible for the study were examined clinically and had knee x-rays according to a uniform procedure to diagnose knee osteoarthritis and measure patellar indices before surgery. After surgery, these patients had their knee x-rays taken in standard position, the knee was flexed 30 degrees and the x-ray direction was perpendicular to the knee, the entire knee joint was in the middle of the image, in which the lower pole of the patella was in the center of the image receptor (Figure 1a, b). We used Syngo.via software to measure patellar indices. Each dimension was measured 3 times and the average value was taken. From there, the cases of patella baja were identified before and after surgery (Figure 1c). After surgery, patients were divided into 2 groups without and with patella baja (Group 1 and group 2, respectively) to evaluate the results.

2.3. Post-operative monitoring
After surgery, patients are instructed to perform rehabilitation exercises according to a uniform procedure. Pain level was assessed according to the VAS scale. Patients were measured for joint range of motion, patella indices, KS and KFS scores.
2.4. Data analysis and processing
Means and standard deviations were taken into account when comparing differences in outcomes between different groups. We use the Chi square test, which is considered statistically significant when P < 0.05. Independent outcomes were analyzed through 95% confidence intervals. All our analyzes were performed using STATA 12.0 software
2.5. Ethics in research
Patients participating in the study were randomly selected in the community. Patient information is guaranteed to be confidential. All patients were informed and explained about the purpose of the study and the various clinical and laboratory examinations that would be performed. After being explained and advised about the research objectives, patients’ visits for examination, surgery and follow-up were all voluntary and were carried out in accordance with what had been previously advised. This study, involving human subjects and human data, was conducted in accordance with the declaration of Helsinki and was approved by the ethics committee of Hanoi Medical University, Vietnam.
3. Results
3.1. Patient characteristics
Of the total 58 patients studied, there were 53 women and 5 men. Patient ages ranged from 51 to 83 years old, average 65.86±7.61 years old. Among the patients studied, there were 14 (24.14%) obese patients, 20 (34.48%) overweight patients (Table 1).
3.2. Patella indexes
The average value of patellar height through the indicators IS (Insall-Salvati), MIS (Modified Insall-Salvati), BP (Blackburne-Peel) and CD (Caton-Deschamps) before surgery were 1.12 ± 0.23, 1.54 ± 0.42, 0.85 ± 0.21, 0.95 ± 0.29 compared to 1.19 ± 0.26, 1.51 ± 0.25, 0.73 ± 0.30, 0.79 ± 0.25 after surgery, respectively. Most indicators changed insignificantly before and after surgery (Table 2).
In our study, before surgery, 2 knee joints (3.23%) had true patella baja. After surgery, 7 knees (11.29%) had true patella baja and 3 knees (4.84%) had pseudo-patella baja. The total number of knee joints with patella baja after surgery was 10 (19.13%) (Table 3).
3.3. Surgical outcomes
In our study, all 58 postoperative patients were instructed on rehabilitation exercises and evaluated results according to a uniform process. The proportion of patients followed for more than 6 months was 88%.
After surgery, 51 (82.26%) knee joints flexed over 90º, of which 28 knees (45.16%) reached >110º, the average knee flexion amplitude reached 103.11º±15.44º (Table 4).
Postoperative knee extension amplitude achieved good results with 60 joints (96.77%) fully extended and only 2 knees lost extension >5º (Table 5).
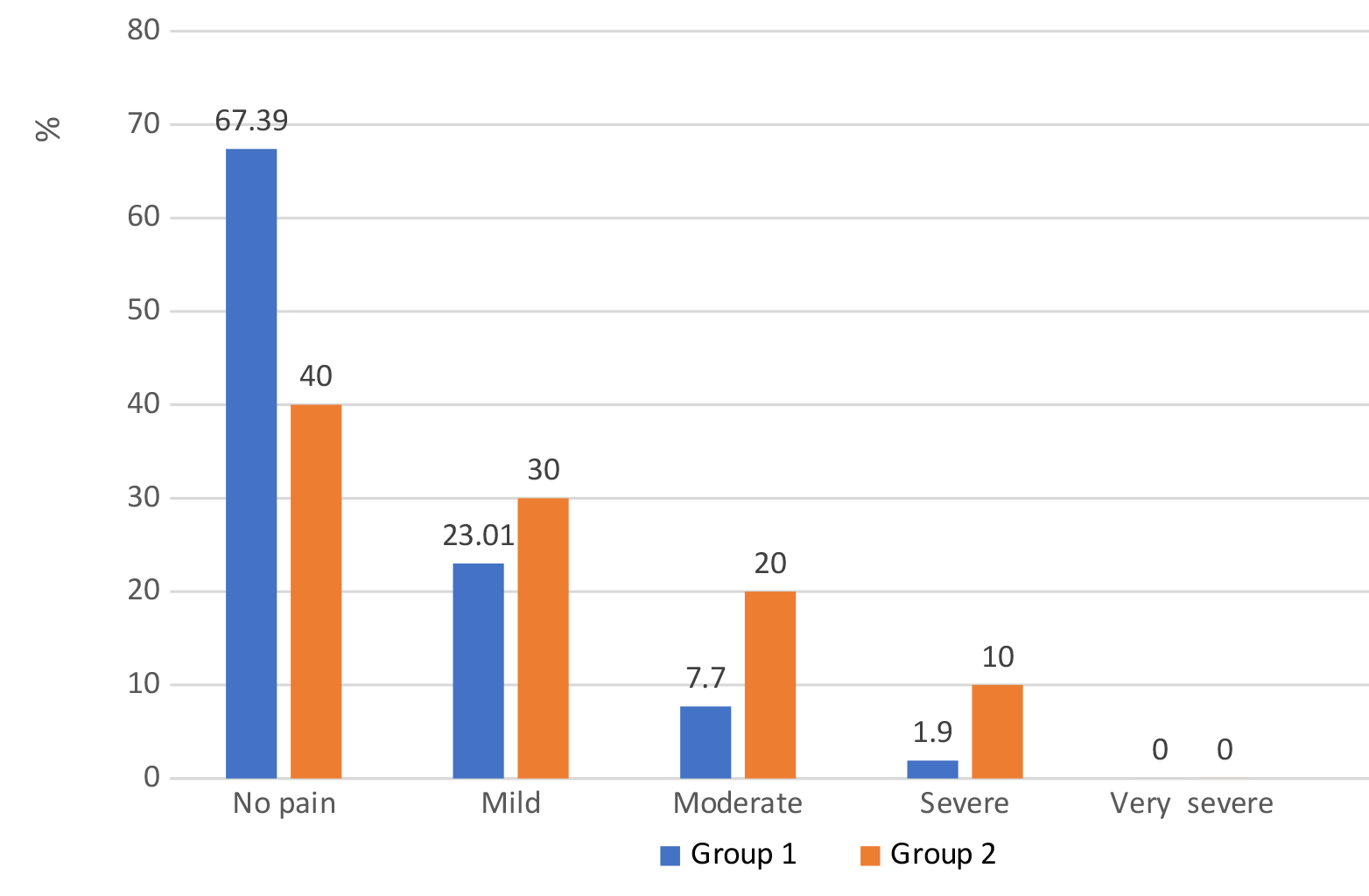
Regarding post-operative knee pain, at the time of the most recent evaluation, out of a total of 62 knee joints, no joint had very severe pain. The normal patella group had 35 (67.39%) pain-free knees, while the baja patella group had only 4 (40%) pain-free knees (Chart 1).

Regarding knee function scores, all 62 knee joints before surgery had KS and KFS scores below 60. After surgery, the average KS score of the whole group reached 83.69±9.98 compared to 33.44±11.38 before surgery. Similarly, the KFS score after surgery was 81.01±8.84 compared to 37.05±8.08 before surgery (Table 6).
At the time of latest follow-up in group 1, according to KS and KFS scores, 94.23% and 96.15% of patients achieved excellent and good results, respectively. In group 2, this rate only reached 80% according to KS score and 70% according to KFS score, respectively.
According to the KS and KFS scores, in group 1, 5.77% and 3.85% of patients achieved moderate results, respectively. While this rate in group 2 were 20% and 30%, respectively.
4. Discussion
The objective in this study was to evaluate the results of 2 groups with patella baja and normal patella after knee replacement surgery. The study patient group ranged in age from 51 to 83 years old, with an average age of 65.86±7.61 years old. Similar to author Doan Viet Quan,11 the most common age group is from 60 to 79 years old, accounting for 72.4%. According to Bin Xu,12 this is the age group most often prescribed knee replacement. In our study, 58.62% of patients were overweight and obese, while only 3.45% of patients were underweight (Table 1), this result is similar to the studies of other authors, such as Author Bin Xu,12 Henrik Behrend.13 According to research by Nicholls et at, for every 5kg increase in weight, the risk of knee osteoarthritis will increase by 35% and overweight women are up to 4 times more likely to develop early knee osteoarthritis than other women of the same age.14
In this study, the IS index after surgery increased slightly compared to before surgery, although this change was not significant. This may be because during surgery we removed the degenerated bone spurs of the patella, so the length of the patella was shorter than before surgery. Our results are similar to those of authors Bin Xu12 and Dejour.15
In our study, the MIS index before and after surgery did not change significantly. This result is different from author Bin Xu.12 According to this author, the MIS index before and after surgery has a statistically significant difference (p<0.0001), MIS before surgery is 1.61 ± 0.22, after surgery was 1.51 ± 0.21. This difference may be due to the fact that we did not perform patellar replacement, whereas these authors tended to replace the patella, leading to changes in the length of the patellofemoral articular surface, and thus MIS index changes (Table 2).
BP and CD indexes often change during total knee replacement surgery.16 Bin Xu,12 when studying 256 knee joints, found that both BP and CD indexes changed significantly compared to before surgery (p<0.0001), while our BP and CD indexes there was no difference (Table 2). During the surgery, we calculated that the thickness of the removed bone was equal to the thickness of the instrument, so the height of the tibial plateau was almost constant. We balance the tibial component to the middle of the tibial plateau, measure and test carefully before installing the artificial joint to restore the knee joint’s anatomy as much as possible. In addition, we did not perform patellar replacement, so almost all BP and CD indices did not change significantly compared to before surgery. In author Bin Xu’s study, the author performed patella replacement. They also cut the tibia bone more than the tibial instrument thickness, leading to a difference in the postoperative BP and CD index compared to before surgery, and the results are different from ours.
In our study, the rate of true patella baja before surgery was 3.23% (2 joints), and after surgery increased to 11.29%, this difference is statistically significant (p<0.01). Both knees that were determined to have true patella baja before surgery had limited range of motion, including 1 case with rheumatoid arthritis for > 20 years and 1 case with severe knee osteoarthritis and deformity. These two knee joints, after knee replacement surgery, still had patella baja even though we released the soft tissue during surgery. In the remaining patients, through post-operative follow-up, 5 more knee joints were found to have true patella baja (Table 3). In Bin Xu’s study,12 the rate of true patella baja before surgery was 9.4%, and after surgery it was 10.2%. Compared to them, our rate of true patella baja before surgery was lower, but after surgery this rate was higher.
Among the 5 patients with true patella baja after surgery, 2 patients did not do rehabilitation exercises after surgery and 2 patients did rehabilitation exercises but did not follow the program instructed by the doctor. The remaining patient did very well in rehabilitation according to the curriculum, very well complied with the exercises as instructed by the doctor and made a follow-up appointment on time. After 6 months, no abnormalities were detected on the radiograph. After 2 years of re-examination, the patient had mild pain and relatively good range of motion, but on the knee x-ray, there was an image of patella baja. Through our research in the medical literature, it is possible that in this case, we removed too thoroughly the Hoffa fat behind the patella, causing the patellar tendon to become undernourished, leading to shortening over time. Or it is also possible that the patient has limited knee flexion and extension movements due to the surgical technique, and in the long term the patellar tendon also shortens, causing patella baja. Author Floren17 reported that 37% of patients had shortening of the patellar tendon >5% through the standard incision and 14% of patients had shortening of 10%. Author Koshino18 reported in his study that 65% of patients had patellar tendon shortening >10%, whereas Weale7 reported this rate to be 34%.
Pseudopatella baja (PPB) is known to cause changes in the relationship of the patella and femoral trochlea after surgery. The most common cause of PPB is an elevated joint line. In this study, before surgery we did not have any patients with PPB, however, after surgery we discovered 03 knee joints with PPB, accounting for 4.84% (Table 3). In these 3 cases, there is one case of a patient with a very small anatomical size of the knee. Although we used the smallest tibial plateau component size, it is still slightly larger than the patient’s actual tibial plateau, causing the joint space line of the tibial plateau to be higher than before surgery, leading to PPB. The remaining two cases may be due to the fact that during surgery, the distal femoral cut was too thick, leading to thinning of the tibial cut. Therefore, the tibial cutting part is less than the thickness of the tibial plateau component, leading to a decrease in the distance from the lower pole of the patellar articular surface to the line passing through the tibial plateau articular surface, causing PPB. In all 3 of these cases, we performed the classic incision, which went into the quadriceps tendon, causing damage to the flexion system of the knee joint. Maybe this is also a contributing factor to PPB in this study. However, our results are still lower than Bin Xu’s study.12 According to this author, before surgery, the PPB rate was 0.8%, and after surgery this rate increased to 9%, twice as high as the results of our study. But in general, patients with patella baja, our results and Bin Xu’s are similar, that is, patella baja after surgery accounts for about 15%.
The IS and MIS indices are used to evaluate patellar tendon length, and both of these indices use the tibial tuberosity as an anatomical landmark. BP and CD are used to measure joint line height and both use the tibial plateau plane as an anatomical landmark. IS and MIS can be used to detect true patella baja, but they cannot be used to evaluate PPB because they cannot evaluate joint line changes. BP and CD are important indicators to detect PPB because they combine the consideration of patellar tendon length and joint line height. The combination of these indicators will help to more comprehensively evaluate patella status and provide a basis for detecting true patella baja and pseudopatella baja.
In her 2006 study, Thornton-Bott19 performed a multicenter study of 266 patients with normal patella, recording the degree of soft tissue release and the size of the spacer. As a result, in the group of patients with minimal soft tissue release, only 21% of patients were found to have PPB after surgery, while in the group of patients with extensive soft tissue release, this rate was 47%. In the group of patients using <12mm spacers, the rate of patients developing PPB was 25%, while in the group of patients using >12mm spacers, this rate was up to 46%. The authors concluded that the incidence of PPB increases with the degree of soft tissue release, pad thickness, and that total knee arthroplasty with excessive soft tissue release increases the risk of PPB, possibly up to 100%. Giulia Bugelli20 also believes that minimal bone cutting and using spacers with the smallest thickness (8mm) will help surgeons avoid patella baja complications.
Of the 62 knee joints that underwent total knee replacement surgery, 51 joints had a maximum knee flexion >90° (accounting for 82.26%), of which 28 knee joints had a maximum knee flexion >110°, accounting for 45.16%. The maximum knee flexion reached 150°. The patient with the lowest knee flexion range of motion, reaching 70 degrees, was the patient with patella baja before and after surgery, even though the patient had received active rehabilitation exercises (Table 4).
Patella baja reduces the length of the moment arm and the lag of extension, reducing the range of motion of the knee joint. When studying the range of motion of knee joints with patella baja, Chonko2 suggested that when the length of the patellar tendon is shortened by >10%, there will be an inverse correlation between the shortening of the patellar tendon and the knee range of motion, and between patellar tendon position and knee joint function.
The change in joint line after TKA surgery will change the kinematics of the knee joint.21 When the joint line is high, it is easy to cause patella baja, which is more likely to cause pain in the front of the knee, reduced range of motion, reduced knee function and negative impact of the patella on the tibia or spacer.2,21,22 Rand believes that the higher the joint line is, the lower the patella moves compared to before surgery.23
In our study, 60 knee joints (96.77%) had full knee extension, only 2 knee joints (3.23%) lost >5 degrees of extension (Table 5). Our results are similar to the research results of domestic authors such as Doan Viet Quan11 and Vo Sy Quyen Nang.24 Kazemi,25 when studying patella baja, divided his 60 patients into 3 groups, group A did not have patella baja, group B had pseudopatella baja and group C had true patella baja. The author concluded that the range of motion of group A was significantly higher than that of groups B and C and the level of pain in group A was less than the other two groups. However, the KSS scores in all 3 groups did not have a statistically significant difference. In other studies, it has been shown that patella baja can affect the mechanical axis of the femur and patella, hindering range of motion, wearing out the polyethylene spacer, and causing postoperative pain.2,17,21
We divided the study group of patients into 2 groups, group 1 included 52 knee joints without patella depression, group 2 included 10 knee joints with patella baja. In group 1, 67.39% of patients had no pain during the examination, only 7.7% of patients had moderat pain and 1.9% of patients had severe pain, there were no patients with very severe pain. Meanwhile, in group 2, only 40% of patients had no pain, but 20% of patients had moderate pain and 10% of patients had severe pain (Chart 1). The difference between the number of patients in each pain level of each group is statistically significant (p<0.05). This means that when patients have patella baja, they will have more pain than patients who do not.
The average KS score in our study was 83.69 ± 9.98, which was significantly improved compared to before surgery. Many authors also noted a significant improvement in KS score. Doan Viet Quan11 recorded an average postoperative KS score of 86 ± 7.61, while Ahmad Hafiz26 reported an average postoperative KS score of 90.94 ± 5.6. Giulia Bugelli20 reported that the postoperative KS score of knees without patella baja was 86.7 points, and that of the patella baja group was 84.2 points.
In our study, the KS score of group 1 was 85.06±10.4, while the KS score of group 2 was 76.67±8.67, the difference is statistically significant (Table 6). In group 1, patients had less pain, better flexion and extension, and patients could walk longer distances, so the average KS score was higher. Our results are similar to Alfredo et al.27 When studying 354 knee joints, the authors found that the KSS score of the group without patella baja was higher than the group with patella baja, although pain scores and range of motion did not have a significant difference. Rachid Rassir28 also had similar results. However, Giulia Bugelli,20 when studying 203 knee joints, showed that KSS scores between the two groups with and without patella baja condition were no different.
Our post-operative KFS score was 81.01 ± 8.84, also improved compared to before surgery, similar to the KS score. A high KFS score shows that the patient’s knee function has improved significantly and the ability to walk is much better after surgery. This conclusion is similar to other authors when using the KSS scale to compare TKA results. Doan Viet Quan’s study11 had a postoperative KFS of 82±7.76, while Guclu29 also showed positive results with an average postoperative KFS of 87.1.
Giulia Bugelli20 also showed that the postoperative KFS score of the group without patella baja was 87.8 points, and the group with patella baja was 85.1 points. In our study, in group 1, the average KFS score was 83.78 ± 8.9, while the average KFS score of group 2 was 74.36 ± 6.15. Although the KFS scores in both groups improved compared to before surgery, the improvement in group 1 was better (Table 6).
5. Conclusion
After total knee replacement for 58 patients with 62 operated knees, patella indices did not change significantly after surgery compared to before surgery. The pain level, range of motion and knee function of the group without patella baja improved better than the group with patella baja after surgery. However, more detailed studies with longer follow-up periods are needed.