


Introduction
Osteofascial compartment syndrome is a medical condition characterized by increased pressure within a closed fascial compartment, which is formed by bones, interosseous membranes, fascia, and muscles. This pressure elevation surpasses the perfusion pressure, leading to acute ischemia of the tissues within the compartment and the development of acute symptoms.1,2 It can manifest in different anatomical locations, including the lower leg,3,4 forearm,5,6 thigh,7 upper arm,8 and foot.9 Causes of osteofascial compartment syndrome can be divided into traumatic and non-traumatic factors. Traumatic causes include muscle tears or strains, blunt trauma, penetrating injuries, chemical injuries, electrical injuries, and crush injuries. Non-traumatic causes include poisoning, insect bites, and infections.5,10
Prompt diagnosis and emergent fasciotomy are crucial interventions in effectively preventing the progression of osteofascial compartment syndrome.11 Delay in diagnosis and treatment can result in irreversible complications such as nerve damage, muscle necrosis, and even amputation.12,13 Classic approaches for fasciotomy in cases of tibial osteofascial compartment syndrome include the double-incision method, which involves a lateral approach and a posteromedial approach,14 as well as the single-incision method.15 In recent years, a new approach called the Mesh notch technique has also emerged as an alternative option. This technique involves creating a mesh-like notch in the fascia to relieve the pressure within the compartment and restore tissue perfusion.16 The choice of surgical approach depends on the specific case and the surgeon’s expertise.
The paper presents a rare case of bilateral tibial posterior compartment syndrome, a rare condition that was caused by prolonged squatting after alcohol intoxication. The medical team utilized an innovative posterior approach to manage the patient and achieved good results.
Case presentation
A 24-year-old female presented to our hospital with bilateral lower limb swelling and pain. The patient reported a history of getting drunk and squatting in a car for 10 hours prior to the onset of symptoms. No specific treatment was administered on the day of the incident. However, the swelling and pain in her lower limbs progressively worsened over time, prompting her to seek medical attention. The duration from the onset of mild symptoms to hospital presentation was approximately 24 hours.Upon admission, the patient underwent vascular angiography as the initial diagnostic procedure to rule out deep vein thrombosis (DVT).
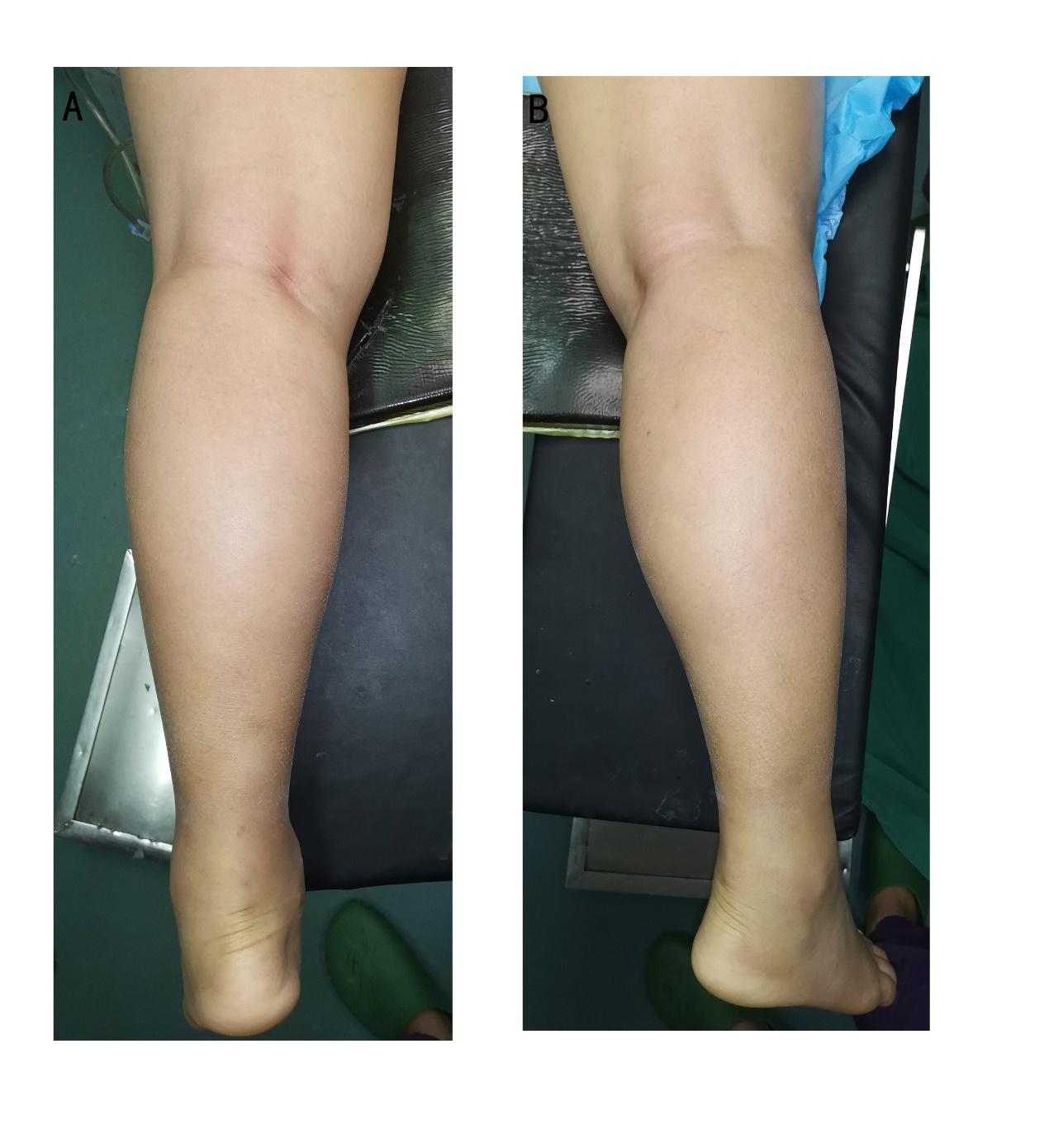
The patient presented with significant bilateral lower limb swelling. On examination, the skin tension of the bilateral tibial posterior was noted to be high, while the skin tension of the lateral and anterior aspects was normal (Figure 1). The patient experienced pressure pain in the bilateral tibial posterior region. Additionally, numbness was observed in the bilateral plantar skin. The pulsation of the bilateral dorsalis pedis artery was weakened, and the posterior tibial artery at the ankle joint was not palpable. Furthermore, active dorsiflexion of the bilateral ankle joint was significantly limited, but plantar flexion was still possible. Passive dorsiflexion elicited positive traction pain.

The patient’s laboratory results at admission revealed several abnormalities. The white blood cell count (WBC) was elevated at 17.7 x 10^9/L, with a neutrophil percentage of 81%. Liver function tests showed elevated levels of alanine aminotransferase (ALT) at 614 U/L and aspartate aminotransferase (AST) at 1096 U/L. Muscle damage markers were significantly elevated, with creatine kinase (CK) levels at 95270 U/L and creatine kinase-MB (CK-MB) levels at 3660 U/L. Lactate dehydrogenase (LDH) levels were also elevated at 2239 U/L, along with hydroxybutyrate dehydrogenase (HBDH) levels at 1050 U/L. The chloride level was slightly elevated at 114.5mmol/L. Additionally, the C-reactive protein (CRP) level was significantly elevated at 141.5 mg/L. These laboratory findings indicate possible liver dysfunction, muscle damage, and systemic inflammation.
Lower extremity vascular angiography indicated no deep vein thrombosis in both lower limbs.
Based on the medical history, clinical symptoms, laboratory and imaging findings,the patient suffered frombilateral posterior tibial compartment syndrome, rhabdomyolysis syndrome, and alcoholic hepatitis.
Surgical Management
Considering the young age of the patient and the high disability rate associated with compartment syndrome, incomplete decompression could have a significant impact on the patient’s lifelong outcomes. Therefore, Dr. Li, the author of this study, innovatively employed the posterior approach for surgical treatment.The patient underwent a total of three surgical interventions. Before each operation, she signed the corresponding surgical consent forms, affirming her comprehensive understanding of the procedures, potential risks, and anticipated results. Furthermore, she consented for her treatment process and associated data to be utilized for academic publications and educational objectives, thereby contributing to the medical community’s knowledge and research advancement in similar cases.
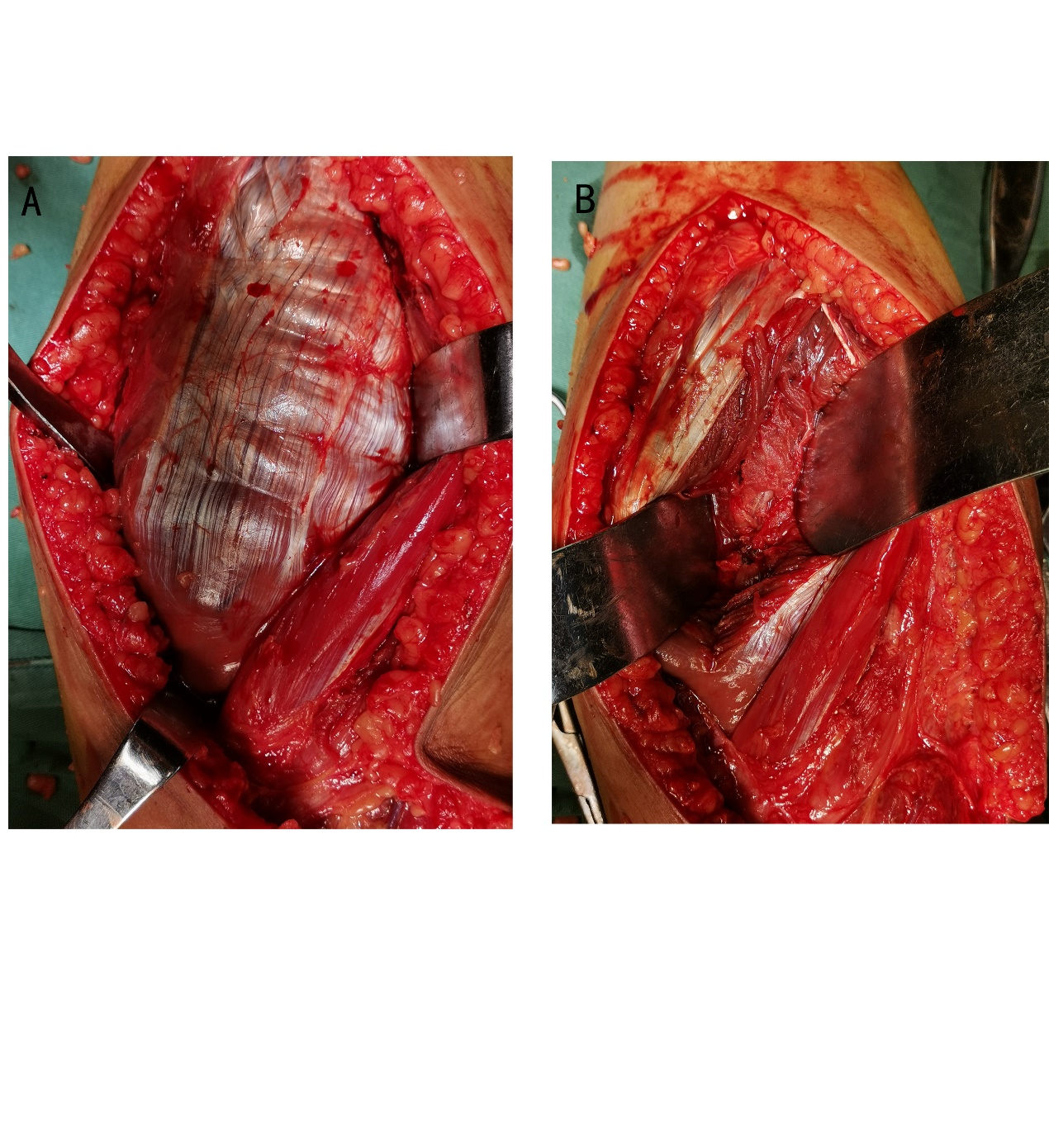
One stage (emergency surgery):The urine appears to be brown in color following catheterization. The patient is positioned in a prone position, and a posterior approach incision is made in an S-shaped pattern from 3 cm above the transverse crease of the popliteal fossa to the lower 1/4 of the distal leg, approximately 21 cm in length. The layers of skin, subcutaneous tissue, and deep fascia are carefully separated. Subsequently, the gap between the gastrocnemius and soleus muscles is opened, revealing that the color of the soleus muscle resembles fish meat. Additionally, there is a weakened muscle contraction force, significantly reduced muscle tension, and increased muscle fragility.The soleus muscle was longitudinally incised, and a translucent exudation was observed (Figure 2).Continuing with the procedure, the fascia compartment was further incised to expose the posterior tibial muscle, long flexor digitorum brevis, long flexor pollicis brevis, and popliteus muscle. The color of the posterior tibial muscle and popliteus muscle was similar to that of the soleus muscle.The procedure involved exploring the posterior tibial nerve, posterior tibial artery, and vein. The root of the anterior tibial artery could be felt pulsating, while the pulsation of the posterior tibial artery was weaker. Additionally, the color of the lower tibial nerve was darker than that of the proximal tibial nerve. The posterior tibial muscle was temporarily preserved and covered with vacuum sealing drainage (VSD), and the decision for removal would be based on the recovery of the muscle.

Second stage (1 week after the first stage): During the surgery, there was a significant amount of thick secretions present in the tissue space. Additionally, compared to the previous surgery, there was a noticeable improvement in the color of the soleus muscle (Figure 3). Upon exploration of the posterior tibial nerve, some improvement in color was observed, and the pulse of the posterior tibial artery returned. After thoroughly cleaning the wound, it was sutured using limited sutures, and the remaining wound was covered with VSD.

Third stage (2 week after the first stage): After thoroughly cleaning the wound, it is completely sutured(Figure 4).

Clinical outcome
12 hours after the first surgery, the levels of ALT were 425 mg/L were completely normal.Four years of follow-up showed mild limitations in squatting function, normal ankle joint flexion and extension, and unrestricted walking ability in the patient (Figure 5).

Discussion
Timely and effective fasciotomy decompression can prevent the occurrence of complications in compartment syndrome.17 Relevant studies have shown a high incidence of poor outcomes in compartment syndrome, ranging from 33% to 43%.18,19 Most current researches indicate that compartment syndrome should be treated with complete decompression,20,21 however, there is limited research on the optimal level of decompression for the best patient recovery, and there is no objective standard.22 Currently, the commonly used methods for decompression of lower leg compartment syndrome are double incision14 and single incision.15 Whether these methods can achieve complete decompression or if they are the optimal approach remains to be further validated. In our article, we used a posterior approach for the first time to treat compartment syndrome. The approach not only opens the posterior compartments of the tibia, but also allows for visualization of the posterior blood vessels and nerves, enabling direct observation of the decompression effect. Additionally, the transverse popliteal ligament is incised to achieve more complete decompression. After thorough debridement, the white blood cell count decreased from 17.7*109/L to 8.6*109/L on the following day.
Previous literature has reported that the main objective of surgery for compartment syndrome is decompression.23 However, there is no relevant research on whether clearing the surrounding infiltrates has an impact on clinical outcomes. In this case, after thoroughly decompressing the fascial compartments and cleaning the surrounding infiltrates during the initial surgery, normal muscle color was observed within 7 days postoperatively. During the final follow-up, it was found that the patient had achieved satisfactory functional outcomes in both lower limbs.
CRP plays an important role in predicting the prognosis of compartment syndrome.24 Relevant studies have shown that when Creatine kinase levels reach 10,000 U/L, it can lead to clear poor outcomes.18 In our case, the Creatine kinase level reached 95,270 U/L. However, after our surgical treatment, no serious postoperative complications were observed.
There are multiple causes that can lead to compartment syndrome, but this case report describes a unique scenario where compartment syndrome was caused by squatting in a car for 10 hours after alcohol consumption. This particular case also involves compartment syndrome in the posterior compartments of both lower legs, which has not been reported before.
The case presented in this article on the posterior approach fasciotomy decompression for the treatment of bilateral tibial compartment syndrome provides a viable treatment option for surgeons. However, further research and clinical practice are still needed to further validate its efficacy and safety.
Authors’ contributions
WL – designed the study, acquisition of data, drafted manuscript, literature search, and analyses; QLZ – designed the study, literature search, and analyses. YL – study conception and design, collected the data; YC – study conception and design, collected the data, preparation of figures; LB –literature search and analyses; QKZ – analysis, and interpretation of data, critical revision and supervision; final approval, submission of the manuscript.All authors read and approved the final manuscript.
Conflict of Interest Statement
All the authors declared that they had no conflict of interest in this case report.
Funds
This work was supported by program funded Fuyang Municipal Health Commission of China (No. FY2019-064 and No.FY2021-051).
Authorship declaration
All authors agree with the publication of the manuscript.