

1. Introduction
Chronic lower back pain (CLBP) represents a significant global health issue, characterized by its high prevalence, debilitating effects, and considerable economic impact.1,2 In fact, CLBP is estimated to affect approximately 28% of adults in the United States annually and 90% at some point in their lives, imposing a financial burden of over $300 billion on the healthcare system.3,4 The primary cause of CLBP in adults is often attributed to Degenerative Disc Disease (DDD), with surgery being the recommended option when conservative treatments fail.5–7 Among the various surgical interventions for CLBP associated with DDD, spinal fusion has traditionally been considered the gold standard.8–10 However, this technique has been criticized for its high rates of perioperative complications, lengthy recovery times, and the potential risk of accelerating degeneration in adjacent spinal segments, potentially leading to further pain and disability. In fact, clinical success rates stand at only 51% for patients at the 5-year follow-up.11–14
For decades, total joint replacement has been recognized as an effective and proven option for treating chronic pain resulting from degenerative conditions in the hips, knees, and shoulders.13 More recently, total disc replacement (TDR) has emerged as a solution for disc degeneration, gaining popularity in numerous healthcare settings as a promising alternative to fusion for treating CLBP.15,16 TDR is proported for its potential to shorten recovery periods and reduce the likelihood of adjacent segment degeneration, which could, in turn, lessen the need for revision surgeries.11 Nevertheless, the development of effective spinal joint replacements has faced several hurdles. These challenges range from the necessity of creating biomechanically reliable and enduring prostheses to addressing the considerable anatomical changes accompanying spinal degeneration.13 While TDR has demonstrated potential in alleviating pain, reducing disability, and decreasing work absences in cases of cervical DDD, outcomes for the lumbar spine remain a subject of debate.2,3 This meta-analysis aims to compare the outcomes of lumbar disc replacement (LDR) versus interbody fusion (IBF), providing a comprehensive overview of their impact on patient care.
2. Material and Methods
2.1. Search strategy
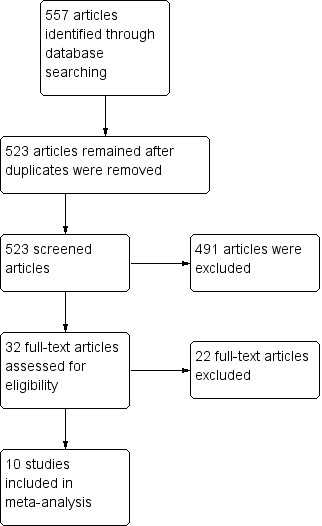
Following the PRISMA guidelines, PubMed, Cochrane, and Google Scholar (pages 1-20) were searched up until February 2024. The following keywords and Boolean terms “lumbar”, “interbody”, “IBF”, “arthroplasty”, and “replacement” were utilized to find articles comparing lumbar IBF to LDR. Supplementary articles were added by going through reference lists from articles and Internet searches. One author extracted the data and another confirmed the choice of the included articles. The process is summarized in the PRISMA flowchart (Figure 1).

Articles were included if they consisted of comparative studies, comparing IBF to LDR. Articles were excluded if they were non-comparative, or based on national databases (in order to avoid an overlap of patients).17–20
2.2. Data extraction
Eligibility of the included studies were determined by two reviewers independently. Extracted data consisted of surgery related outcomes (operative room (OR) time, estimated blood loss (EBL), and length of stay (LOS)), adverse events (complications, and reoperations), and patient reported outcome measures (PROMs) (Oswestry disability index (ODI), back pain, and leg pain). If present, differences between the investigators were resolved by a third independent reviewer.
2.3. Risk of bias assessment
The ROBINS-I tool was used to assess the risk of bias in the included non-randomized studies by two authors independently.21 Studies were excluded if they had a critical risk of bias. The Cochrane risk-of-bias tool was used in a similar manner to assess the risk of bias for randomized studies.
2.4. Statistical analysis
Review Manager 5.4 (The Cochrane Collaboration, 2020) was implemented for the statistical analysis. Mean differences (MD) and standardized mean differences (SMD) with 95% CI were used for continuous data while odds ratio (OR) was utilized for dichotomous data. Heterogeneity was evaluated by Q tests and I2 statistics. In considerable heterogeneity indicated by p ≤ 0.05 or I2> 50%, random-effects model was used. On the other hand, the fixed-effect model was chosen if p > 0.05 or I2 < 50%. A statistically significant result is shown by p=0.05.
3. Results
3.1. Characteristics of the included studies
Ten studies met the inclusion criteria with 6 being randomized controlled trials (4 different trials and 2 reporting different outcomes of similar included trials22–25) 3 retrospectives and 1 prospective, and were included in the meta-analysis.13,22–30 These studies included 1720 patients with 1034 being in the LDR group and 686 being in the IBF group. The main characteristics of the included studies are summarized in Table 1.
3.2. Surgery related outcomes
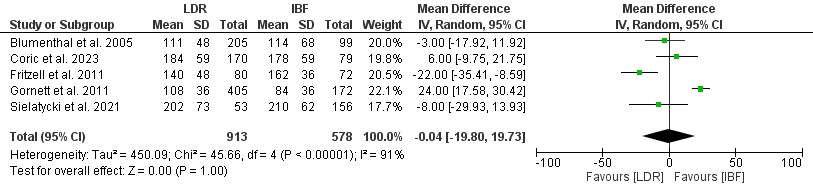
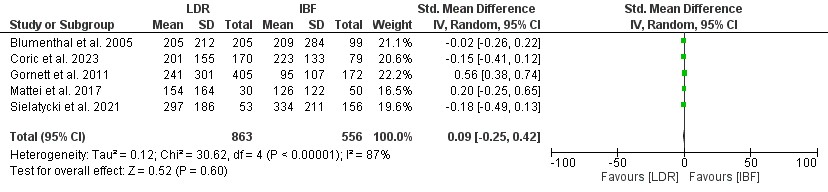
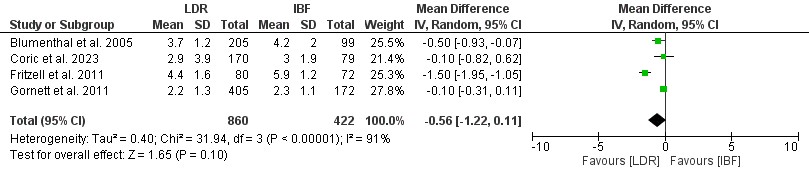
Five studies including 1491 patients reported data about OR time (913 in the LDR group and 578 in the IBF group), five studies including 1419 patients reported data about EBL (863 in the LDR group and 556 in the IBF group) and four studies including 1282 patients reported data about LOS (860 in the LDR group and 422 in the IBF group). No statistically significant difference was seen in OR time (Mean Difference=-0.04; 95% CI: -19.80–19.73, p=1.00, Figure 2A), EBL (Standardized Mean Difference=0.09; 95% CI: -0.25– 0.42, p=0.60, Figure 2B), or LOS (Mean Difference=-0.56; 95% CI: -1.22– 0.11, p=0.10, Figure 2C).



3.3 Adverse Events
3.3.1. Complications
Six studies including 1545 patients reported data about complications (947 in the LDR group and 598 in the IBF group). No statistically significant difference was seen in the rate of complications (Odds Ratio=1.02; 95% CI: 0.73– 1.43, p=0.90, Figure 3A).

3.3.2. Reoperations
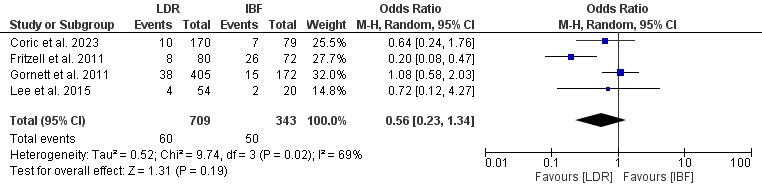
Four studies including 1052 patients reported data about the rate of reoperations (709 in the LDR group and 343 in the IBF group). No statistically significant difference was seen in the rate of reoperations (Odds Ratio=0.56; 95% CI: 0.23– 1.34, p=0.19, Figure 3B).

3.4. PROMs
3.4.1. ODI
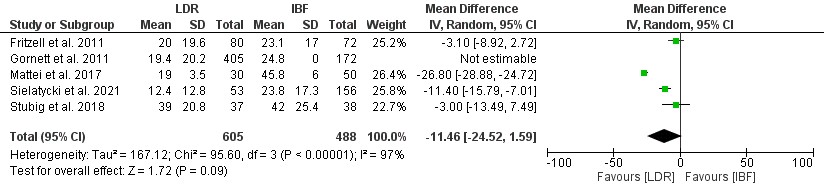
Five studies including 1093 patients reported data about ODI (605 in the LDR group and 488 in the IBF group). No statistically significant difference was seen in ODI (Mean Difference=–11.46; 95% CI: -24.52– 1.59, p=0.09, Figure 4A).

3.4.2. Pain
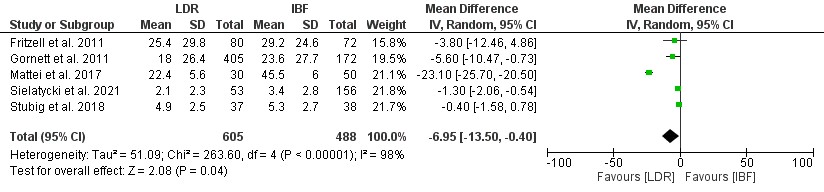
Five studies including 1093 patients reported data about back pain (605 in the LDR group and 488 in the IBF group), and three studies including 861 patients reported data about leg pain (495 in the LDR group and 366 in the IBF group). Patients in the LDR group had a lower mean back pain (Mean Difference=-6.95; 95% CI: -13.50– -0.40, p=0.04, Figure 4B), but no difference in leg pain (Mean Difference=-0.28; 95% CI: -1.94–1.27, p=0.74, Figure 4C) when compared to the IBF group.


4. Discussion
This meta-analysis examining 6 studies with 1720 patients revealed no difference in EBL, LOS, OR time, ODI, leg pain, complications, and reoperations between TDR and lumbar spinal fusion. However, lower back pain scores were shown in the LDR group.
When examining OR time, EBL, or LOS, no statistically significant difference was found between TDR and IBF. In fact, the absence of difference in OR time is in line with the statistical similarity for EBL31 and align with the findings of a previous meta-analysis by Mu et al. comparing LDR to anterior lumbar interbody fusion.32 Nevertheless, in their meta-analysis, they reported a reduced LOS in the LDR group.32 However, not only did they have only 3 studies in their LOS analysis, but two of the three studies reported data about overlapping patients making their results not valid.23,33
The absence of statistically significant difference in overall complications and reoperations between LDR and IBF aligned with the findings of Mu et al.32 However, Annette et al. favored LDR as it showed a reduced rate of complications.34 Nevertheless, our analysis included 6 studies compared to only 2 studies in both of their analysis making our results more valid. Similarly for the reoperation analysis, Mu et al. included only two studies while our analysis included 4.32
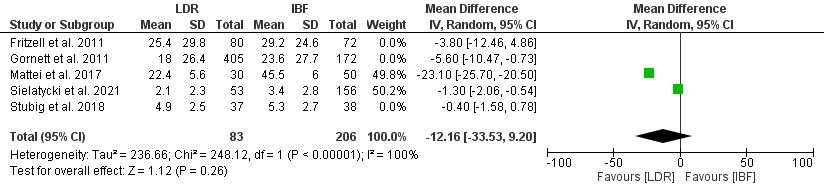
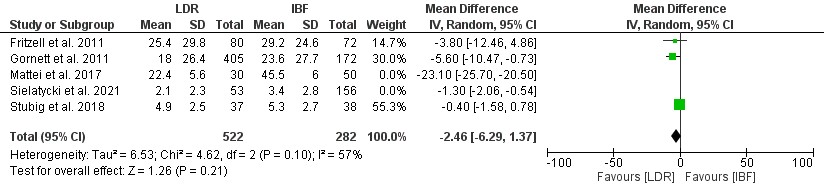
Despite the absence of statistically significant difference in leg pain and ODI, LDR was shown to reduce back pain. This reduction of pain (6.95, Figure 4B) exceeded the minimal clinically important difference being around 3.5 on a scale of 0-10.35 However, one must note that when taken separately, back pain at 1 year follow-up (Figure 5A) and 2-year follow-up (Figure 5B) did not differ significantly between LDR and IBF. Both Annette et al. and Mu et al. reported lower back pain and ODI in LDR.32,34 However, Annette et al. only included 2 studies in their analysis while Mu et al. included three studies, but with different follow-up timepoints (2 studies had 2-year follow-up and one study had 1-year follow-up).32,34


Strengths and limitations
The main limitation of this study are the absence of post-operative sagittal radiographic parameters and cost analysis. Furthermore, a sub-analysis based on the type of interbody fusion was not possible due to the low number of studies assessing a similar IBF approach. Nevertheless, this study included an extensive literature review leading to an inclusion of a substantial number of studies.
5. Conclusion
The findings of this meta-analysis revealed no significant differences in OR time, EBL, LOS, rates of complications, reoperations, and leg pain between the LDR and IBF procedures. However, LDR was associated with a significant reduction in mean back pain, which exceeded the minimal clinically important difference, suggesting a potential advantage in terms of pain management. Nevertheless, this reduction in back pain was not significant when stratified by follow-up timepoints and may be due to an absence of deformity and disc degeneration at other levels. Consequently, this study supports the use of both LDR and IBF as effective treatments for CLBP.
Corresponding Author
Alan H. Daniels, MD
1 Kettle Point Ave
East Providence, RI 02914
Email: alandanielsmd@gmail.com
Disclosures and Funding
BGD reports the following: receives consulting fees from Clariance, SpineArt, and SpineVision. AHD discloses the following, receives royalties from Spineart and Stryker, consulting fees from Medtornic, research support from Alphatec, Medtronic, and Orthofix, and Fellowship support from Medtronic.
The rest of the authors do not report any conflicts.
Source of Funding
None.