

Introduction
Fracture of the post-wall of the acetabulum is the most prevalent type of acetabular fracture, with incidence rates ranging from 25% to 47% in the literature.1 Due to the long-lasting beneficial functional outcome, a precise diagnosis and an effective treatment plan are paramount. Subsequently, further research by Letournel.2 Matta3 and Mayo4 demonstrated the advantages of acetabular internal fixation and open reduction, with acceptable results in 80 to 90 % of the patients. These studies emphasized the importance of achieving perfect anatomic reduction during surgery. Comminuted posterior fractures add more difficulties to fix small and small fragments.
Pelvic reconstructive plates, cortical or cancellous screws, cerclage wires, spring plates, and any combination of these may be used as fixation methods for these fractures.5–8in 1989, Mast et al. were the first to propose the use of spring plates for adjunctive fixation of comminuted posterior wall fractures.9 It is unclear from the literature which fixation method is the best or how much rigidity and stiffness are needed to keep a fracture fixed. Lag screws have been shown to be mechanically inferior when used alone; additionally, they carry the risk of joint penetration, particularly when used for small marginal fragments.10
The main objective of this study was to evaluate the clinical, functional, and radiological results of using spring plates combined with conventional 3.5 mm pelvic reconstruction plates for the treatment of posterior wall acetabular fractures.
Materials and Methods
General data
A prospective case series study of 24 patients (21 men and 3 women) with comminuted fractures of the acetabulum post wall (two or more fragments) or peripheral fragments (small periarticular fragments) was carried out in Egypt’s Al-Azhar University hospitals (Al-Hussein, Bab elshaeryya, and Damietta) from April 2020 to March 2023.
Life-threatening events were handled in accordance with the ATLS protocol, which was used for all patients’ first survey treatment. In addition, secondary survey management covered the date and kind of trauma, past medical history, clinical, neurovascular, and radiographic examinations (pelvis, spine, extremities, abdominal ultrasound, CT pelvis and acetabulum). The Judet and Letournel classification was used to classify and diagnose acetabular fractures.11
The inclusion criteria for patients were as follows: (1) were adults aged more than 18 years (male or female) (2) had fragmented fractures of the post wall of the acetabulum (two fragments or more) or peripheral fragments (3) had experienced trauma within 2 weeks (4) had primary intervention(5) were ambulatory prior to fracture(6) signed informed consent form; and (7) had clear consciousness and no severe medical comorbidities.
Exclusion criteria include: All patients who have (1) Trauma more than 2 weeks (2) Single fragment fracture of post wall (3) open fracture of acetabulum (4) Associated fracture of post column or ant column (5) Hip joint and/or surrounding soft tissue infection that is active (6) Pathologic fractures (7) Non ambulatory patient (8) Unfit for surgery (severe medical comorbidities)
Fifteen patients had associated injuries with the fractured post-wall of the acetabulum (62.5%). Two patients had fractured ribs, three patients had hemothoraxes, one patient had fractured humerus, two patients had fractured patella, two patients had fractured tibial plateau, two patients had fractured oscalsis, and three patients had sciatic nerve injury. The remaining nine patients (37.5%) had fractures localized to the post wall of the acetabulum.
Patients underwent surgery 6 days on average (range: 3–13 days) after trauma. The period before surgery was impacted by numerous factors. The most significant factor was the interval between the actual trauma and the day the patient arrived at our hospital; Due to their general health, 4 patients were first admitted to the ICU. The availability of blood units for transfusion during surgery was another problem; Two patients had blood group AB-, and one patient had blood group O-, which contributed to a significant delay in surgery.
Ethical approval
The Al-Azhar Ethics Committee at Al-Azhar University Hospitals in orthopaedic department approved this study under registration number Pat._3Med.Research.0000003, and all the study participants gave their written and verbal informed consent.
The average age of all patients was 34.5 years (18 to 45 years). Antithrombotic prophylactic therapy was started in all patients at the time of hospitalization and was stopped 12 hours before the operation. Four whole blood units were reserved for each patient.
All patients were evaluated via routine laboratory investigations, heart, chest, and anesthesia consultations were performed to assess surgical suitability and obtain consent for the procedure.
Operative details
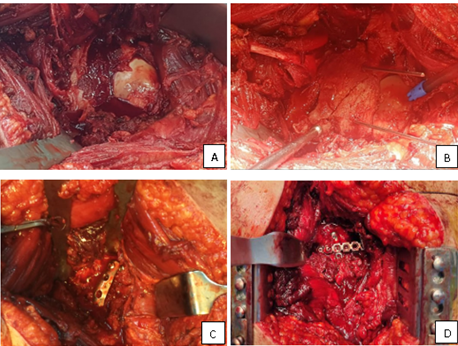
The induction of anesthesia was accompanied by the administration of prophylactic antibiotics (2 g of third-generation cephalosporin) to all patients who underwent spinal or epidural anesthesia. All patients underwent the same surgical procedure. They were set up in a lateral position. With the afflicted hip on the upper side and the thigh and leg free draped to be easy to move and manipulate during surgery to aid reduction, all fractures were revealed and stabilized using the K-L technique, which is the accepted gold standard in the treatment of posterior wall fractures. The gluteus maximus muscle was divided along the vascular plane after an incision was made in the skin, subcutaneous tissue, and fascia lata. After identification of the short external rotators, they were tagged, their ends were cut, and the sciatic nerve was protected. The fracture fragments were examined, any soft tissue pieces between the fragments were removed, and any associated capsular soft tissues were preserved [Figure 1A]. The osteochondral free fragments of the hip joint were removed, and the degree of marginal impaction was determined via the application of light traction. After that, portions of the posterior wall and their connected capsular ligaments were reduced and kept in place using a sharp ball spike. Kirshner wires were occasionally used after the final reduction was complete [Figure 1B]. A 3 or 4hole one-third tubular plate was modified by cutting a small central portion of the terminal hole of the plate. This process leaves 2 adjacent end prongs. Both prongs are bent at an angle of 60 to 90 degrees toward the undersurface of the plate. The hooks were designed to press on the bone fragments but not into the labrum. A 2-mm Kirschner wire (K-wire) was used to hold the comminuted wall fragments in a reduced position. The K-wire was positioned behind the bony rim of the acetabular wall fragment, which was directed away from the intra-articular marginal rim surface to avoid penetration of the joint space. The spring plates were placed at 90 degrees to the articular fragments creating a buttress effect. The medial hole of the spring plate was fixed to the retroacetabular bone with a 3.5-mm cortical screw. Compression of the malleable straight spring plate led to better contouring of the retroacetabular surface, increasing compression of the joint fragments. Spring plates were not precontoured to anatomically fit the residual intact bone. A pelvic reconstruction (straight or curved) compression plate, usually from 8 to 10 holes in length, is placed over the spring plates to increase the stability of the spring plate effect and prevent postoperative loss of fixation. The spring hook plates were extended medially beyond the longer buttress plate. All patients underwent open reduction and internal fixation with a precontoured one-third tubular plate (spring plate) [Figure 1C], which was secured with one or two 3.5 mm cortical screws and reinforced with a 3.5 mm reconstruction plate [Figure 1D]. Following fixation, a stability test and moderate traction at the hip joint were used to confirm intra-articular reduction. With the use of suction drainage tubes, the incisions were stitched and closed in layers.

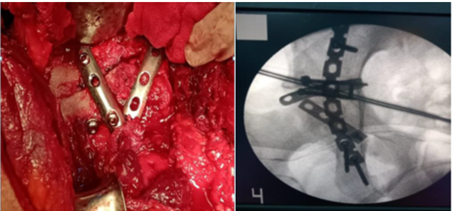
Eighteen patients were fixed with one spring plate, six patients were fixed with two spring plates, and all of them were reinforced with a 3.5mm reconstruction plate [Figure 2].

Postoperative
Forty-eight hours after surgery, the wound was sterileressed, and the surgical drain was removed, followed by removal of the epidural catheter. Between the 12 and 15 postoperative days, the sutures were removed.
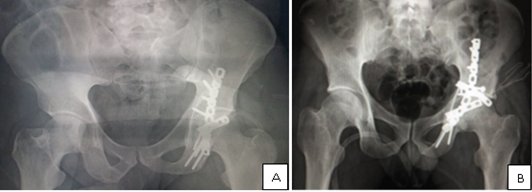
Immediate postoperative radiographs were used to judge the precision of the reduction [Figure 3]. Follow-up radiographs were taken regularly in the outpatient clinic to detect any reduction changes. The displacement of 0 to1 mm was considered anatomical, the displacement of 2 to 3 mm was considered good, and displacement >3 mm was considered unsatisfactory [Figure 4].


All patients were regularly followed every 3 to 4 weeks until the fracture healed, every 3 months until 1 year, and then every 6 months. Active-assisted and pain-free passive range of motion exercise was suggested after surgery.
Patients were advised to use crutches on the injured extremity. After six weeks, partial weight bearing was permitted; after ten to twelve weeks, full weight bearing with one crutch, or cane was allowed. After the fracture had healed completely, unprotected weight bearing was advised.
The modified Merle D’Aubinge and Postel [MAP] score12 was used to evaluate functional outcome, a clinical score of 18 judged excellent, a score of 15-17 Good, a score of 13-14 fair, and poor with a score <13.
The final radiological results were assessed using Matta’s criteria.3 A normal hip joint has an excellent score, while a good score indicates minor changes with minimal sclerosis and joint narrowing, a fair score denotes significant changes with considerable sclerosis and joint narrowing [50%], and a poor score denotes advanced changes.
The clinical assessment of hip function was performed via the modified Harris Hip Score [mHHS].13 Its ranges are as follows: 70 bad, 70–79 fair, 80–89 acceptable, and >90 excellent. Complications that developed during the follow-up period were recorded.
Statistical analysis
SPSS (version 25, Armonk, NY, USA) was used to analyze the data. For quantitative variables, data are presented as mean and range, while qualitative data are presented as percentage and frequency.
Results
At a mean follow-up of 14 months (range 6-24), 24 patients (21 men and 3 women) with a mean age of 34.5 years (range 20-48) were included. The most frequent cause of injury was motor vehicle collision (13 patients), followed by 9 patients being struck by a car, the last two patients experienced falls from height [Table1]. Fracture reduction was anatomical in 12 patients, good in 10 patients, and poor in 2 patients [Table 2].
The average operating time was 107.5 minutes, with a range of 90 to 140 minutes. The range of blood loss during surgery was 300-800 cc. Blood was transfused into 16 patients; 14 patients received one unit and the other two patients received two units.
Regarding complications reported in our study, three patients had neurological injury (neuropraxia of the sciatic nerve) postoperatively (12.5%) and improved after four months. Furthermore, patients who had a sciatic nerve injury directly after trauma improved after three months. Regarding postoperative infection, one patient had an early deep wound infection at 2 weeks, which improved after surgical debridement and medication, and another patient had a superficial wound infection that improved with medication without debridement [Table 3].
Nine months after surgery, two patients who experienced AVN of the femoral head were treated with total hip replacement (THR). During follow-up, three patients (12.5%) experienced mild post-traumatic osteoarthritis (OA), which had an impact on clinical outcome by causing joint stiffness and pain.
Regarding clinical outcomes and physical function [Figure 5], the mean MAP was 10.2 (range 5–12), and the mean mHHS was 86 (range 64–96). Finally, at the most recent radiographic check-up, no delayed union, malunion, or screw penetration was found. Neither implant loosening nor heterotopic ossification was detected [Table 3].

Discussion
The complex anatomy of the pelvis makes operative fixation of acetabular fractures challenging. Accurate anatomical reduction enhances the prognosis of these injuries.14–17 Most posterior wall fractures involve comminution and marginal impaction, making secure fixation of small periarticular fragments using screws and plates challenging and increasing the possibility of joint penetration or subsequent surgical comminution.18 Traditional buttress compression plating, lag screws, and spring plates, are all recommended as fixation methods for posterior wall fractures.19 Lag screws, alone in comminuted small fragments, are not the ideal fixation method.20
Currently, several surgical fixation techniques have been developed for comminuted fractures of the acetabular posterior wall using locked compressive Pilon plates, T plates, and cervical spine plates. Although these methods have a better contact surface with comminuted fragments and plates than the original one-third tubular plate, they still have issues with longitudinal plate contouring and less peripheral screw fixation than spring plates. Contouring custom plates decreases the final compression of the spring plate, as it reduces the loading of the plate.21,22
The standard treatment for post-wall fracture is buttress compression via the use of an ilio-ischial reconstruction plate.23,24 However, high shear stresses, which are more prevalent in cases of superior fragments, are not adequately resisted by it.25 Additionally, this approach lacks the adaptability to successfully compress and retain the multi-fragmented wall in place in cases of comminuted fractures.21,26 This longitudinal plating technique requires contouring along the complex-shaped retro-acetabular surface. Furthermore, because this plate runs along the pillar of the posterior column, it is extremely challenging to properly buttress the fragment with the plate alone in case the fracture extends to the acetabulum’s superior dome.25
To ensure the fixation of small fragments and prevent intra-articular screw penetration, which is required for fixing such fragments close to the articular surface, the use of a spring plate was advised.8,24 However, these plates (usually one-third tubular) are mostly utilized as an adjuvant for the ilioischial plate20,26 and are thought to be too weak to be used individually, especially for larger fragments.24
However, few mechanical studies have compared different posterior wall fracture fixation strategies. One of these studies that involved cadaveric specimens demonstrated that lag screws through a plate were substantially stiffer and stronger than lag screws alone (those that failed at a higher load). Similarly, adding spring plates to the reconstruction plate made it stronger and stiffer.27
In terms of biomechanics, the spring plate serves as a dynamic buttress for peripheral bone fragments. The prongs of the plate, which are made by cutting the end hole of the one-third tubular plate, act as a point of fixation to hold the small pieces of bone. Minor pre-contouring of the plate enables a dynamic buttressing effect as the plate adapts to the bony architecture.28
In this study, 79 % of patients had excellent to good results at the final check-up. Comparing these clinical results with those of other series using the same approach, the finding is quite favorable. Our study’s average mHHS was 86 (range 64–96), which is comparable to that of Gaurav A et al.29 In addition, De Mauro D et al.30 reported an average mHHS of 84.9 (range 59–94) and 92.22 (range 80.8–99.6). Furthermore, the mean MAP in our study was 10.2 (range 5–12), whereas it was 10.2 (range 5–12) according to De Mauro D et al.
Our study did not report a high complication rate; only two patients developed avascular necrosis and were treated with total hip replacement. Other three patients. 12.5%. had mild arthritis, and these results are very favorable compared to those of De Mauro D. et al. who reported a patient with femoral head necrosis that required THR treatment 12 months after surgery. Additionally, seven patients (15.2%) had posttraumatic osteoarthritis (OA) that was detected during radiological follow-up and had an impact on their clinical prognosis through pain and stiffness in their joints.
Strengths and limitations
The strengths of the study include the fact that the established assessment techniques used the — mHHS and MAP — were consistent with those employed by other authors at institutions perform reconstruction of comminuted posterior wall fractures. As a result, we can quickly compare our findings with those of others. The study’s limitations, however, include the small sample size (due to the infrequent occurrence of comminuted posterior wall fractures) and the lack of original spring plates. In every instance, the spring plate was shaped with a potential bias toward the surgeon’s manipulation of the implants.
Conclusion
Comminuted posterior wall acetabular fractures can be stabilized with the help of spring plates. It could be used in conjunction with the primary reconstruction plate as a viable alternative for stable and anatomical reduction. High patient satisfaction and good functional results make this approach effective.
Conflicts of interest
The authors declare that they have no relevant financial or non-financial interests to report.
Financial support and sponsorship
No funding was used in this study.
Availability of data and material
The datasets used and analyzed during this investigation are accessible upon request from the corresponding author.
Acknowledgment
No
Authors’ contributions
-
Mohamed A. A. Ibrahim: Study design, participation in writing the manuscript and follow up of patients, grammar and language editing, corresponding author.
-
Mostafa. M. Elgahel: Participation in writing the manuscript (surgical technique) and follow up of patients.
-
Shady. A. Gouda: study design, participation in writing the manuscript, statistical analysis and follow up of patients.
-
Mohamed Rohayem: participation in writing the manuscript, statistical analysis and follow up of patients.
-
Mahmoud M. Hassaan: Participation in revising the manuscript and revising statistical analysis.
-
Zenat A. Khired : Participation in revising the manuscript and revising statistical analysis.
-
Maamon Aljonaid: final revision of the manuscript and statistical analysis.
Declarations
-
Ethical approval: This article does not contain any studies of animals.
-
Informed consent was obtained from all individual participants included in the study according to the rules of the hospital research ethical committee.
-
The study obtained approval from the Institutional Review Board (IRB) under registration number Pat._3Med.Research.0000003, ensuring ethical compliance and participant protection.
-
All procedures performed in our study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Competing interests
There are no conflicts of interest in the manuscript, including financial, consultant, institutional and other relationships that might lead to bias or a conflict of interest. Authors had no disclosing of any financial ties to the subject of this research.