Introduction
Treating degenerative joint disease through Total Knee Arthroplasty (TKA) is a successful procedure, but it does come with a significant risk of blood loss that may require transfusion. In the past, around one-third of patients who underwent total joint arthroplasty (TJA) needed 1 to 3 units of blood after the operation.1,2 During total knee arthroplasty (TKA), a tourniquet is commonly used in the surgical technique to minimize intraoperative bleeding. However, this may lead to significant postoperative blood loss.3 After surgery, there is typically a drainage of 500 to 1000 cc, and there may also be an additional hidden blood loss of up to 700 cc. As a result, the total blood loss is determined by comparing pre and postoperative hematocrit values ranging from 1500 to 1900 cc.4 Various factors can affect bleeding following TKA. These include pre-existing conditions in patients (such as cardiovascular, respiratory, hepatic, and coagulation disorders), medication usage (such as NSAIDs, salicylates, LMWH, and antiagregants), the type of anesthesia used (spinal versus general), postoperative blood pressure management (keeping systolic under 150 mmHg), surgical technique (use of cement, incision technique, tourniquet time, hemostasis, and tissue damage).5 A multicenter study was conducted in Europe to assess the use of allogeneic blood transfusion in 3996 patients who underwent unilateral hip and knee replacement surgery. The results showed that 46% of patients required transfusions, which correlated with low preoperative hemoglobin levels. It was discovered that the infection rate among patients who received autologous transfusions was significantly lower, at only 1%.6 This may be linked to immunosuppression that can occur with allogeneic transfusion.7 Research has found a correlation between acute postoperative anemia and transfusion with higher morbidity and mortality rates. These risks include angina, myocardial infarction, heart failure, and delayed progress in rehabilitation.8 Tranexamic acid (TXA) was an antifibrinolytic medicine discovered in the 1960s. It has since become crucial to postoperative blood management in orthopedic surgery. TXA is a synthetic derivative of lysine, an amino acid, and it works by attaching to plasminogen, stopping fibrin from breaking down. Numerous studies have confirmed TXA’s blood-saving properties since its first use in TJA by Benoin et al. As a result, TXA has become a more prevalent treatment option for TJA.9 Numerous studies have compared the effectiveness of TXA through intravenous, oral, and topical use in recent decades. However, distinct benefits have yet to be found for any specific route of administration.10 In a meta-analysis study, the effectiveness of topical intra-articular administration of TXA was compared to that of a placebo in TKA. The study revealed that both treatments had comparable results in reducing blood loss, hemoglobin reduction, and the need for blood transfusion. Moreover, adverse reactions were not observed in either group.11 In addition, Lin et al. conducted a study that showed that combining topical and intravenous TXA could reduce overall blood loss and the need for transfusions without increasing the risk of Deep venous thrombosis (DVT), compared to intravenous TXA alone.12
Materials and methods
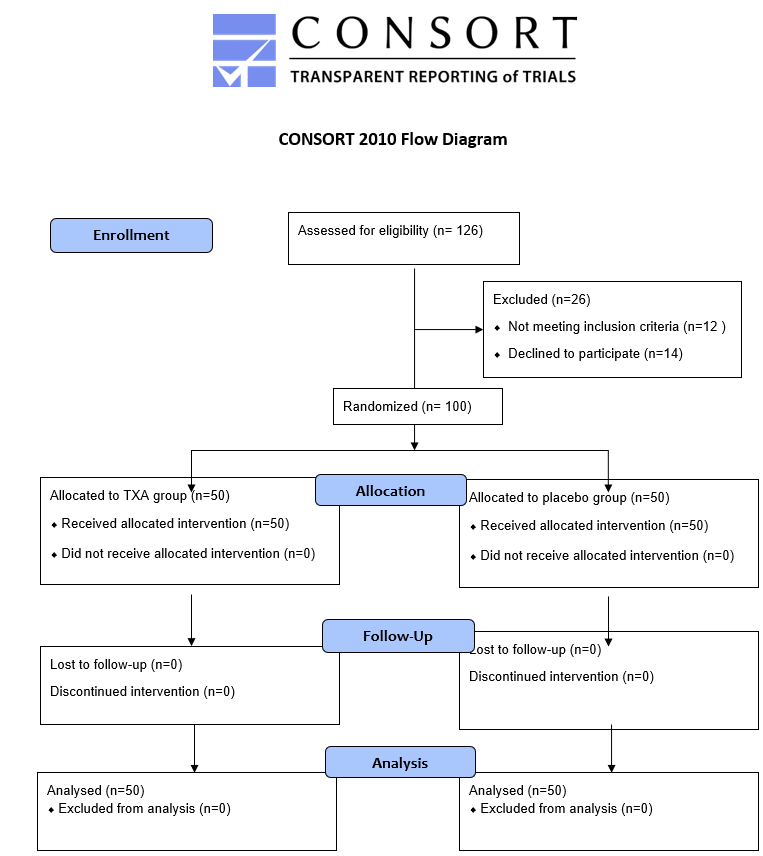
This study, which is a prospective, randomized, triple-blinded (patient, surgical team, data collection team) controlled trial, was performed in Damascus, Syria. It was also registered in clinicaltrial.gov under the number NCT05919615. One hundred participants were enrolled between July 2021 and September 2022 and followed up with every patient for six months. Written informed consent was obtained from all participants. All the methods were conducted according to the CONSORT statement.13 The study included patients undergoing unilateral primary TKA for primary osteoarthritis knees; exclusion criteria are shown in Table 1. Participants were randomly assigned to one of two groups following simple randomization procedures (computerized random numbers). They were allocated to the TXA group and placebo group in a ratio of 1:1. Fifty patients were included in the placebo group, and 50 were included in the TXA group. The allocation was put into concealed envelopes independent of the surgeon and the author, and the randomization was performed by a research fellow who was not involved in patient care. Participants who went unilateral primary TKA and did not use TXA, just IV normal saline (0.9% sodium chloride), formed the control group. In contrast, the intervention group comprised participants who went primary unilateral TKA and used two-dose intravenous tranexamic acid that was applied as follows: 10mg/kg of Tranexamic Acid in 100 Milliliters (ml) normal saline (0.9% sodium chloride), the first dose 15 minutes before the tourniquet deflation and the second dose at 180 minutes after the first dosage.

Surgical technique and postoperative management
One senior surgeon performed the operations. All patients were given 1g of cefazolin 20 minutes before the incision, then 1g thrice daily for 48 hours after surgery. The surgeries were performed under ischemia with a full inflating of the tourniquet to a pressure 125 mmHg higher than the patient’s systolic blood pressure after limb exsanguination and releasing it after closure and compression bandage application. The procedures were done under spinal anesthesia, and a medial para-patellar approach was used. The prostheses used in all patients were cruciate scarifying cemented DePuy Synthes PFC Sigma without patellar resurfacing. All patients received drains, which were removed 48 hours post-surgery. During hospitalization, subcutaneous low-molecular-weight heparin (Enoxaparin 2000 IU) was administered 8 hours postoperatively and once daily (4000IU). An (Apixaban 2.5 mg orally) was administered twice daily, which continued for 21 days after discharge.
Outcome measures
The primary outcome measure was 72h total blood loss. Total blood loss (TBL) in the perioperative period was calculated using the Gross formula,14 estimated by hitting the patients’ blood volume by the difference between pre-and post-operative hematocrit values divided by the initial hematocrit value. Intra-operative blood loss is the amount of lost blood intraoperatively and was measured by the time of incision closure by calculating the increased weight of the utilized wet mops and the volume of the suction bottle after erasing the amount of the used lavage. Post-operative blood loss is the amount of lost blood postoperatively that was calculated as the output of the drain bottle once two days after surgery. Hidden blood loss is the amount of lost blood in the tissues not measured intraoperatively or postoperatively and was calculated once 72h after surgery using the difference between total and intra and post-operative blood loss. The secondary Outcome Measure was transfusion rates throughout the patient’s hospital stay, an expected average of 3 days (8g/dl was our threshold for blood transfusion or clinical symptoms of inadequate oxygen supply, i.e., dyspnea, tachypnea, reduced.
Consciousness, etc.). All adverse events, such as infection, VTE, etc., occurred six months postoperatively and were recorded. They were assessed if it happened within month intervals until six months after surgery. All the patients received an examination for clinical symptoms of DVT every day during hospitalization. Both lower limbs were examined using a diagnostic Doppler ultrasound three days postoperative and in the first visit or earlier if a patient exhibited any clinical symptom (e.g., limb swelling or calf pain).
Sample size
A pre-hoc power analysis was done for the primary outcome measure of 72h total blood loss (TBL). Using a medium effect size of 0.5, power of 0.8, and alpha error of 0.05, we determined that 82 participants were required to be enrolled in the study. Eighteen participants were needed to compensate for a 20% expected dropout rate, and 100 were enrolled in the study, divided randomly into two groups.
Statistical analysis
The categorical variables were analyzed using the Chi-square test or Fisher’s exact test, and the Student t-test was used for continuous variables, with P <0.05 considered significant. All data were analyzed using the Statistical Package for the Social Sciences (SPSS), version 28 (IBM).
Results
Patients: The diagnosis in all patients was primary osteoarthritis. One hundred patients completed the study (50 patients in each group), and we did not lose any patients during the follow-up period, and all patients committed to follow-up visits. The youngest patient was 56 years old, the oldest was 76, and the average age was 65.87.
The characteristics of the studied sample did not show any statistically significant differences in age, gender, and body mass index (BMI), as presented in Table 2.
Outcome measures: There was no statistically significant difference in terms of intraoperative blood loss as the average value of bleeding was (75.00) and (84.03), respectively, in the TXA and control groups, and the p-value was (0.072), as shown in Table 2.
On the other hand, there was a statistically significant difference between the two groups regarding hidden blood loss, total blood loss, and post-operative blood loss values. The average values are shown in Table 2.
We needed an allogeneic blood transfusion for eleven patients in the TXA group and 13 patients in the control group. There was no statistically significant difference between the two groups, and the p-value was (0.640), as shown in Table 2.
As for the complications, we had five cases of superficial wound infection, six cases of deep venous thrombosis in the TXA group, eight cases of superficial wound infection, and five cases of deep venous thrombosis in the control group. No cases of deep sepsis or pulmonary embolus occurred in either group. There was no statistically significant difference between the two groups regarding complications, and the p-value was (0.219), as shown in Table 2.
Discussion
Total knee arthroplasty (TKA) is a complex surgery that often relieves pain and improves patient function. However, there are still complications related to the surgery, especially regarding excessive intra- and postoperative blood loss.15 Different methods have been established to decrease intra- and postoperative blood loss and, thus, reduce the risk of allogeneic blood transfusion in the patient after surgery.5 A tourniquet is generally accepted to reduce intraoperative blood loss during TKA.16 TXA has become widely used in knee arthroplasty to reduce perioperative blood loss and transfusions. Several publications worked to determine the dosage, number of doses, timing, and route of administration, which secures the best way to reduce blood loss.9
Through our study, we found that giving TXA in two doses reduced postoperative blood loss and total blood loss. The average total blood loss in the TXA group was 950.60 ml, and in the control group, 1068.46 ml, and there was a statistically significant difference between the two groups’ p-value=0.001. These results are consistent with numerous studies in this field, such as Brian Hallstrom et al. and Eric Tille et al.17,18 However, this difference didn’t seem to carry a critical clinical importance as this difference did not lead to increased blood transfusion rates.
We noticed no statistically significant difference between the two groups regarding blood loss during surgery. These results are inconsistent with those reached by Mohamed A. Lotfy et al. and B. Hari Krishnan et al.,19,20 who found that giving TXA reduces the amount of blood lost during surgery. This can be explained by the fact that we used the tourniquet in all patients, and the tourniquet was not released until after the wound was closed and the compression bandages were applied.
The method of calculating blood loss by calculating the total blood lost during and after surgery is inaccurate because it neglects the calculation of the so-called hidden blood loss, which represents the amount of blood lost in the tissues during and after surgery.3 Therefore, we used the gross formula method to estimate blood loss, which allows us to calculate hidden blood loss. The formula estimates blood loss by hitting the patients’ blood volume by the difference between pre-and post-operative hematocrit values divided by the initial hematocrit value. Thus, we can calculate the hidden blood loss by decreasing the values of blood loss during and after surgery from the value of total blood loss.21
We needed an allogeneic blood transfusion in 13 patients in the control group and 11 in the TXA group, with a p-value of 0.640. Hence, the difference between the two groups was not statistically significant. There was no need for more than two units of blood transfusion in any patient, and allergic reactions occurred in eight patients the supervising internal physician managed. These results suggest that the role of TXA in primary unilateral TKA is overrated. We are not against using TXA in TKA, as it might compensate for inexperienced surgeons as they tend to take more time performing the surgery, and as the expertise grows, usually good surgical habits also develop, such as gentle soft tissue handling and adequate hemostasis. Also, extended surgical dissection and prolonged surgical time are needed in complex and revision cases, so the effect of TXA might be more prominent. as it would reduce the need for allogeneic blood transfusion and thus reduce complications, such as infections and allergic reactions that may have a catastrophic effect, such as death.22,23 Although the literature supports different findings in 2018, David Sadigursky et al. conducted a systematic review and meta-analysis of randomized clinical trials (RCT). They found that intravenous, intra-articular, or combination administration of TXA reduces the need for blood transfusion without increasing the incidence of associated complications.24 In 2017, Marek Lacko conducted an RCT and showed that Intra-articular TXA was equally effective as the IV regimen in reducing the number of blood transfusions.25 These findings might not apply to all cases, especially when done by a well-trained surgeon, since the reported rates range from 3 percent to 18 percent,26 and even higher rates in many other studies,27,28 which displays the variance in transfusion standards between different institutions. Still, we believe surgical skills adequacy also plays a role in this variance. Of course, each case’s complexity implies extended surgical dissection and prolonged operative time, which also affects the blood loss and, thus, the transfusion rates.
Our study did not notice a significant difference between the two groups regarding surgery-related complications. We witnessed five cases of superficial wound infection in the TXA group and eight cases in the control group. They were treated well with antibiotics and topical care. In addition, six cases of deep venous thrombosis (DVT) occurred in the TXA group and five cases in the control group. They were discovered in the first visit by periodic Doppler ultrasound scanning without complaining of clinical symptoms, and these cases were treated without consequences.
Autologous blood infusion is also a viable option to decrease the need for allogenic transfusions. However, it is not available in all centers and can’t be done to all patients, and it has many downsides with no less dangerous complications.29
Our study has several limitations as we excluded high-risk patients, and all surgeries were done in a relatively short time; thus, we cannot generalize our study to high-risk patients, bilateral knee arthroplasty, and junior surgeons. We did not assess the functional outcomes; the follow-up period was short. Still, we may explain this because our study aimed to investigate the effect of giving TXA on the rate of blood loss and the potential complications from its administration. However, the strength of our study is based on our methods; we strived to isolate any external factor that would affect the results; only one highly experienced surgeon did all the surgeries, strict inclusion criteria, and a unified protocol for assessing blood loss and the need for transfusion.
Conclusion
Our study suggests that the role of tranexamic acid in primary unilateral total knee arthroplasty might be overrated. The difference in blood loss doesn’t seem to carry a clinical Importance in simple cases reformed by an experienced surgeon.
Acknowledgments
Not applicable.
Authors’ contributions
Hakam Alasaad: conceptualization, investigation, data curation, writing, editing, and reviewing.
Jaber Ibrahim: conceptualization, investigation, data curation, writing, editing, and reviewing.
All authors read and approved the final manuscript.
Funding
This research is funded by Damascus University - funder No. 501100020595.
Availability of data and materials
All data and material are available for review if requested by the reviewers/ editors.
Ethics approval and consent to participate
Taken for the study by Damascus University’s institutional review board (MD-130623-7-H4)
Consent for publication
Informed consent was received from all patients.
Competing interests
The authors declare that they do not have any competing interests.
The author details
Department of Orthopedics - Faculty of Medicine – Damascus University – Syria