Introduction
Foot drop refers to the inability to dorsiflex at the ankle, usually from a peroneal nerve palsy. The common peroneal (fibular) nerve is the most commonly injured nerve in the lower extremity and is the third most common mononeuropathy in the body.1–4 It may present with both motor and sensory symptoms, with loss of ankle and toe dorsiflexion and ankle eversion, as well as loss of first dorsal webspace and lateral leg and dorsal foot sensation, respectively.
The peroneal nerve branches off the sciatic nerve, the largest branch of the lumbosacral plexus, consisting of L4 through S4 nerve roots. The sciatic nerve traverses through the posterior thigh to the popliteal fossa, at which point it branches into the common peroneal and tibial nerves. The common peroneal nerve wraps around the neck of the fibula, after which it divides into superficial and deep branches. The superficial branch then passes between the peroneal muscles and the lateral side of the extensor digitorum longus, providing motor innervation to the peroneal longus and brevis muscles. Sensory branches provide sensory innervation to the dorsum of the foot and lateral calf. The deep peroneal branch dives deep to the extensor digitorum longus, at which point it crosses the anterior tibial artery and passes through the anterior tarsal tunnel. It serves to innervate ankle and toe-extensors and supplies sensation to the dorsal first webspace.5
At the level of the foot and ankle, the anterior tibialis (ATT) is selectively weak when compared to the flexor muscles, leading to an inherent imbalance between foot flexors and extensors. The gastrocnemius far outsizes other muscles. Given this, there are many ways for imbalance to arise leading to foot drop. These different etiologies lead to a common phenotype, but treatment is based on the cause of imbalance. To our knowledge, there is a paucity of up-to-date reviews evaluating these etiologies and their respective surgical procedures. Thus, the goals of this paper are twofold: (1) to discuss the causes of this condition and (2) discuss the orthopedic surgical treatments options.
Etiologies
Foot drop can be caused by several etiologies, from the level of the central nervous system in the brain or spinal cord, to peripheral causes from the sciatic nerve or its branches. We will discuss these etiologies looking at the time of onset: new onset (patients who were previously neuromuscularly normal) and chronic (systemic or chronic diseases).
New Onset
Most causes of foot drop requiring orthopedic intervention are peripheral and acute in nature. These can occur at any level of the sciatic or peroneal nerve’s course from trauma, internal or external compression. Traumatic injury to the nerve can present in the form of fibula fractures, knee dislocations, and direct lacerations. Woodmass et al. determined that common peroneal nerve palsy was associated with knee dislocations in 5-40% of patients.6 Although rare, iatrogenic injuries can cause peroneal nerve palsy as well; Carender et al found a 0.4% incidence of common peroneal nerve palsy following 47,585 total knee arthroplasties.7 Predominant risk factors for this injury in the setting of knee arthritis include preoperative valgus deformity and flexion contractures.3,8,9 Beyond this, surgeries such as muscle debridement or tumor excision near the peroneal nerve run the risk of injury. Proximally, traumatic injury to the sciatic nerve can also cause a foot drop. This can be from hip injury or surgery, most notably during the posterior approach to the hip.10,11
External compression can be from anything causing excessive pressure on the lower leg, including prolonged bedrest or lateral decubitus position, a poorly placed splint, sitting with legs crossed, among others.12 Internally, space-occupying lesions can compress the peroneal nerve, such as a tumor or cyst near the nerve (e.g., tumor of the fibula, lipoma, Baker’s cyst)13–17 or a tumor of the nerve or nerve sheath.
At the level of the central nervous system, weakness in dorsiflexion may occur because of intra- or extra-axial compression in the brain caused by tumor edema, tumor destruction of tissue hemorrhage, or ischemia involving parts of the central region and pyramidal tract.18 Compression or direct trauma to the nerve roots at the level of the spine can impair dorsiflexion. The intraspinal nerve roots L4 and L5 can be compressed by disc herniation, stenosis, and neurinomas.18 In these settings, foot drop rarely arises as an isolated symptom.
Chronic
Systemic neurologic conditions can also result in foot drop. Disorders such as Amyotrophic Lateral Sclerosis, Guillain-Barré syndrome, and Charcot–Marie-Tooth can cause neuropathy and foot drop. Patients with vasculitis of small arteries may also present with foot drop in late disease. Lastly, leprosy can induce nerve injury, ultimately leading to autonomic, motor, and sensory neuropathy, commonly causing foot drop. At the level of the central nervous system, it can occur as a symptom of cerebral palsy or other disorders affecting brain development.
Treatment
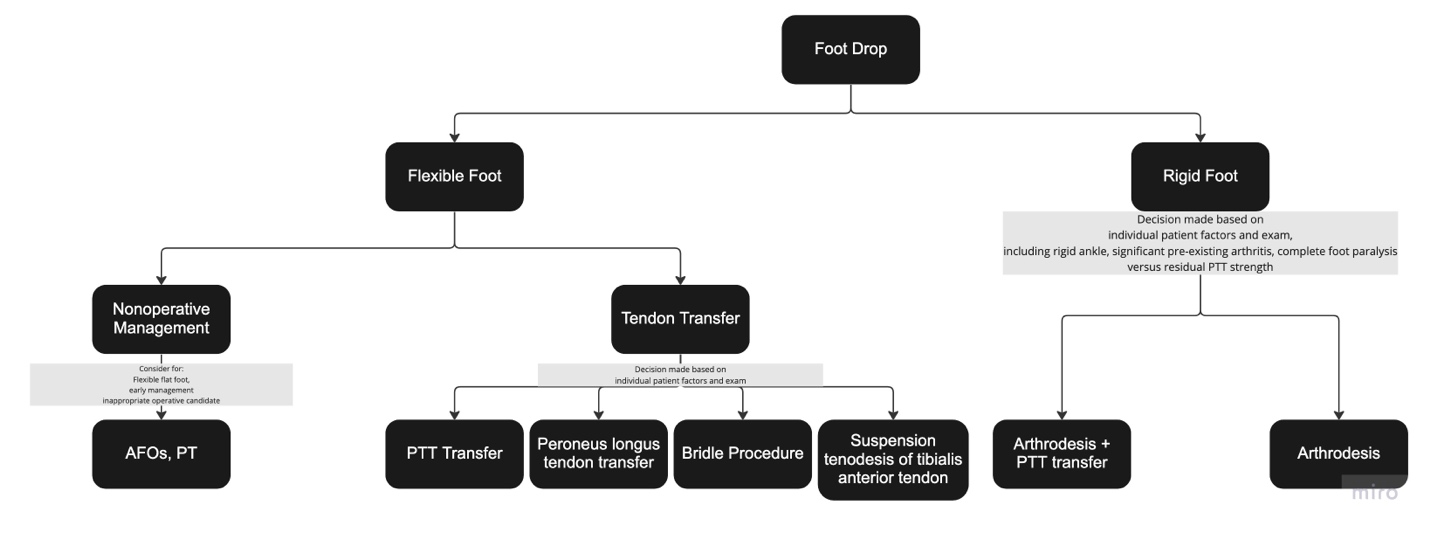
Treatment for foot drop should begin with an initial assessment to identify the deformity as flexible or rigid. A flexible foot drop indicates that the ankle may be passively brought to neutral dorsiflexion, whereas rigid indicates the deformity is fixed and the foot cannot be passively brought to neutral. Foot drop usually begins as a flexible deformity caused by an imbalance of plantar and dorsiflexion by those etiologies described above. It can progress to contractures and eventually, in chronic disorders, the patient can no longer actively or passively dorsiflex the foot to neutral. Additionally, in those patients with systemic diseases, there may be other symptoms present that make it even harder to function and select treatment options. In this section, we will evaluate treatment options for foot drop based on if the foot is flexible or nonflexible.
Flexible Foot Drop
In flexible foot drop, there is a role for nonoperative management in the form of stretching and AFOs. The main goal of these treatments is to stabilize gait, prevent contractures, and prevent falls. The mainstays of this treatment are ankle-foot orthoses (AFOs) and physical therapy (PT).19,20 Van der Wilk and colleagues conducted a systematic review evaluating management of floppy paresis of ankle muscles using AFOs. The three paresis groups (dorsiflexor, plantarflexor, and paresis of both) were distinguished in 24 studies evaluating 394 participants.21 They found that patients with a dorsiflexor paresis benefited more from circular or elastic AFOs with respect to their gait patterns, walking efficiency (decreased effort), and walking speeds. Similar outcomes were found when using a dorsal AFO in patients with a plantarflexor paresis, both with and without a dorsiflexor paresis. The authors noted that adverse effects of dorsal AFOs were decreased ankle ROM and increased physical discomfort.21,22
The goals of surgery in flexible foot drop are to improve gait and eliminate the need of a brace. The most common approach to accomplish these goals is through a tendon transfer. There are multiple types of tendon transfers that can be considered based on the pre-operative patient assessment of potential donor muscles for each procedure. Transferring the posterior tibialis tendon (PTT) is most often the procedure of choice, as it restores dorsiflexion when inserted on the dorsum of the foot and reduces unopposed inversion from the tendon itself.23–26 Woodmass et al. reinforced that the most predictable means of re-establishing antigravity dorsiflexion in a persistent common peroneal nerve palsy (CPN) is with salvage procedures such as posterior tibial tendon transfer (PTTT).6 R.K. Shah and Xu et al explored two routes of transfer for the PTT procedure: the interosseous (IO) route for the correction of foot drop in leprosy and the circumtibial (CT) route in a cadaveric limb analysis. Shah summarizes the long-term results of interosseous PTT with elongation of the Achilles tendon in a prospective study of 69 patients (120 feet) with leprosy neuritis.27,28 Following the surgical procedure with split attachment to the tibialis anterior and to the peroneus brevis or tertius tendons, the leg was placed in a plaster cast for three weeks with the foot dorsiflexed to relieve tension on the tendon sutures. After another three weeks, the cast was split for intensive rehabilitation and coordination exercises (alternate dorsiflexion and relaxation but not plantar flexion) and relearning of “swing-phase walking” with crutches. This was followed by partial weight-bearing in parallel bars or with crutches. Active plantar flexion was allowed six weeks after operation, and the patient was given a sandbag (0.5–1 kg) to use for exercises to build muscle strength. Patients gradually increased weight-bearing until the ninth or tenth week after operation when they could walk without crutches and could practice walking up and down stairs, after which they were considered ready for discharge from intensive physiotherapy. Shah found that tibialis posterior transfer done by the IO route produced active dorsiflexion in 80% of patients, with the restoration of near-normal gait in 94% of patients.27 The author recommended that whenever possible, an IO route should be used, and failure to lengthen the Achilles tendon can lead to a poorer result. Furthermore, they observed that the IO route is preferred with split attachment to the tibialis anterior and to the peroneus brevis or tertius tendons. At final follow-up the IO route produced better active dorsiflexion, although less active plantar flexion, than the CT route. When discussing the CT transfer method of PTT, Shah stated that this route should be reserved for patients with a calcified and unyielding interosseous membrane, generally seen in the elderly with recurrent inflammation and infection in the foot. If CT transfer is performed, the tendon bifurcation must be at least 3 cm above the ankle so that the line of pull is as close to the vertical as possible, as the CT route has been shown to have an unacceptably high rate of recurrent inversion and persistent weakness.27
Jian Xu and colleagues acknowledged the merits of the widely used IO route of PTT transfer providing increased dorsiflexion strength and decreasing the probability of varus recurrence from residual inversion force in literature. However, they found that when compared to the IO method of transfer, the CT route is safe, convenient, and possibly contains a longer moment arm that increases mechanical advantage and thus power than other route.28 Both authors Shah and Xu concur that the CT approach can be used for patients with calcified and unyielding IO membranes and those who experience recurrent foot inflammation, infection, which can alter anatomy and create adhesions in the IO membrane, increasing risk of neurovascular injuries.27,28 Xu et al. felt the CT route was technically easier and had less risk of complication than the IO route. They performed CT PTTT in 25 lower-leg cadavers to determine the optimal height level for tendon transfer (5 to 11 cm of the height proximal to the distal tip of the medial malleolus), finding that a height at 10 cm above the distal tip of the medial malleolus could be optimal for subcutaneous PTT transfer.28
Agarwal and colleagues conducted circumtibial PTT transfers on twenty patients who all had foot drop for more than one year.29 The most common cause of foot drop in this cohort was Hansen’s disease in eleven patients, followed by post-traumatic peroneal nerve damage in seven patients, and post-injection sciatic neuropathy in two. At surgery, three or four incisions were made- one for harvesting the PTT usually over the navicular tuberosity, one posterior to the medial malleolus to mobilize the PTT, one over the IO membrane anterior ankle for passage, and a fourth over the dorsal foot with specific location depending on transfer target. The tendon was detached at the insertion site, and the bulbous end was trimmed. The second incision was made 10 cm above the medial malleolus and the PTT tendon was identified and pulled out. The tendon was split into two slips up to where it crossed the tibia proximally. A third incision was made on the dorsum of the foot or at the dorsal ankle level to identify and isolate the TA and EDL. Two separate subcutaneous tunnels were made for each slip of PTT with the help of a tendon tunneler. One slip of PTT was attached to the TA and the other slip to the EDL tendon and peroneus tertius via pulvertaft weave repair. The tension was adjusted to balance the foot in a neutral position, favoring dorsiflexion and eversion. After a mean follow-up of two years, 19/20 patients could walk with heel-toe gait without any orthotic support. These patients achieved a mean active dorsiflexion of 7.5 degrees, mean active plantarflexion of 36.25 degrees, and total range of ankle movement of 43.75 degrees.29
Cho et al also evaluated outcomes following this procedure, following 17 patients at least three years status-post PTT transfer for foot drop, evaluating level of function compared to matched controls.30 While the functional scores of the patients who had undergone transfer were statistically significantly lower than controls, their mean AOFAS, FAOS, and FAAM scores within the group demonstrated significant improvement postoperatively. All patients saw improvement in their strength. There was no evidence of flat foot deformity radiographically and only one patient required an AFO.30
Molund et al evaluated outcomes for this procedure for common peroneal paresis following knee dislocation.31 They evaluated range of motion (ROM), dorsiflexion strength, and patient-reported outcomes. Fifteen patients underwent PTT transfer and experienced symptom improvement in these three domains at 1 year. Additionally, 12 patients reported high AOFAS scores and increased dorsiflexion strength compared to preoperatively (though still significantly less than the unaffected contralateral side).31
Finally, Yeap et al followed 12 patients status post PTT transfer with the longest-term follow up to date reported in the literature at an average of 90 months.32 They found that 11 of 12 patients maintained at least 4 out of 5 strength in ankle dorsiflexion, with 83% of patients rating their outcome as good or excellent.32
Another tendon transfer option besides PTT is peroneus longus transfer. This is indicated in cases of isolated deep peroneal nerve involvement which generally spares peroneal tendon function. The procedure is performed by first identifying the peroneal tendons laterally, avoiding the sural nerve. The peroneus longus (PL) is elevated and secured with suture then transected as distally as possible in the cuboid tunnel. The PL is then pulled from a proximal incision over the lateral compartment of the distal third of the leg. A bone tunnel is created in the intermediate cuneiform and the tendon is then transferred subcutaneously distally into the bone tunnel, with the proximal stump of the tendon fixed using screws, anchors, or staples.
As the peroneus longus lies adjacent to anterior muscles, it is more easily mobilized and transferred, a technical advantage of the procedure. Regarding outcome, Cohen et al performed postoperative assessment of 19 cases of foot drop caused by leprosy.33 They found average dorsiflexion of 10 degrees and plantarflexion of 32 degrees. Fifteen patients were satisfied with the procedure based on being able to walk without an AFO. Two patients were satisfied but still required a brace. Two patients were unsatisfied and maintained only weak dorsiflexion postoperatively, thought to be secondary to undetected preoperative weakness of the peroneal tendon.33
Finally, among the soft tissue procedures for foot drop, the Bridle procedure utilizes the tibialis posterior, peroneus longus and tibialis anterior tendons in a “tri-tendon” anastomosis. This is done by first transferring the PTT through the IO, then the peroneus longus, followed by a tri-tendon anastomosis of these two tendons with the tibialis anterior, all anchored in bone. The Bridle procedure specifically attempts to address coronal plane positioning to maintain the ankle in more neutral without varus or valgus, which may have been overlooked in other tendon transfers. Flynn et al described the outcomes of eight patients 61 months status post a Bridle procedure (7 of the initial 15 were lost to follow up). They found that all eight patients were able to dorsiflex past neutral and none required a brace postoperatively.34 Johnson et al compared 19 patients to 10 matched controls at two years postoperatively following this procedure.35 They found reduced functional outcomes and comparable ankle DF and PF compared to controls; however, all Bridle patients reported excellent to good outcomes and, perhaps most importantly, reported they would repeat the operation. None of the patients required an AFO.35
The suspension tenodesis of the TA tendon to the distal tibia is another surgical procedure that has been described to correct footdrop deformity. Roukis and colleagues proposed that this procedure was simpler and more secure than transferring the distal attachment of another tendon to a new location in the foot or using tendon weaving techniques.36 Additionally, compared to ankle fusion, the authors claim suspension tenodesis is a less invasive, joint sparing procedure that allows for increased shock absorption during gait. Roukis treated foot drop deformity using this method to tenodese the TA tendon to the distal tibia using paired screws and spike washers in six limbs, four of which had a neuromuscular etiology of foot drop and two with posttraumatic etiology. Preoperatively, each of the six limbs demonstrated the following: (1) complete loss of function of the anterior muscle compartment with the presence of a steppage gait pattern with pronounced foot slap; (2) a supple pes planovalgus foot posture; and (3) the inability to either benefit from or tolerate in-shoe orthoses and lower-limb bracing.36 Each limb underwent a 3-cm incision approximately 10-cm proximal to the medial malleolus and directly medial to the TA tendon. After retracting the subcutaneous tissues, the TA tendon sheath was identified and incised linearly, exposing the underlying tendon, which was then retracted from the site and transected at the proximal extent of the incision near the musculotendinous junction. The periosteum overlying the medial crest of the distal tibia was incised and reflected, after which the exposed cortical bone was roughened using a rotary bur to aid in tenodesis. The TA tendon was then pulled proximally until the foot was in the desired position of neutral ankle dorsiflexion, slight hindfoot valgus, and parallel alignment of the plantar forefoot to the weightbearing surface. The TA tendon was then secured to the underlying tibia using two solid cancellous screws and two small spider washers. Post-operatively, the patients wore a short-leg weightbearing cast maintaining ankle dorsiflexion for three weeks followed by a removable short-leg walking brace for an additional three weeks. During the latter period, the patient received physical therapy for gait retraining and strengthening of the remaining lower leg musculature. This technique corrects the foot slap component of foot drop deformity but does not allow for TA tendon excursion to provide active dorsiflexion of the foot. Nevertheless, some active dorsiflexion was achieved when the peroneus tertius muscle was functioning in conjunction with the enhanced mechanical advantage created postoperatively. Compared with an ankle fusion, this technique is much less invasive, preserves some ankle motion, and allows for a certain amount of shock absorption during the gait cycle. The authors did note that an ankle fusion can be performed if needed to achieve full stability and definitive correction of the symptomatic foot drop.36
Rigid Foot Drop
In rigid foot drop, the ankle cannot be dorsiflexed to neutral. For these patients, the surgical goal is to get the foot straight; these patients will require a postop brace. In these situations, generally it is not just the bone that is fused, but the soft tissue also contracts and the Given this, soft tissue procedures are not sufficient, and ankle fusion is considered. Indications for fusion include rigid ankle, significant pre-existing arthritis, or complete paralysis of the foot with no viable tendon for tendon transfer.37 The Lambrinudi hindfoot realignment with triple arthrodesis has shown favorable outcomes in this patient population. The procedure involves removing a wedge of bone from the plantar-distal talar surface, which is then wedged into a notch created in the navicular. The subtalar joint is then put in a relatively calcaneus or dorsiflexed position and biplanar closing wedge osteotomies are performed to dorsiflex and possibly abduct the foot as needed to correct the equinocavovarus deformity. The procedure is completed with a calcaneocuboid joint fusion. Tang et al followed the outcomes of ten patients at 5.8 year follow up status post Lambrinudi arthrodesis procedures. They found an average of 47 degrees of correction and painless range of motion at time of follow up, with 86 degrees as the maximum arc of motion.38 In terms of radiological imaging, flattening of the talus was present in seven patients. Preoperatively, 100% of patients had less than 10 degrees of ankle ROM. At follow-up, the group’s active range of motion varied from 5 to 50 degrees. Five patients showed an improvement in exercise tolerance postoperatively and all patients who previously had difficulty in using ordinary footwear no longer had this issue. All five patients who reported pain prior to the procedure had complete resolution postoperatively. No patient reported a diminished ability to perform daily activities. Functional outcome measures ranged from good (five of ten patients) to fair (five of ten patients).39
So et al was able to locate ten patients who had undergone an Lambrinudi arthrodesis for the following reasons: eight with poliomyelitis, one patient with a diagnosis of Kugelberg Welander spinal muscular atrophy, and one with recurrent clubfoot deformity associated with spina bifida. The average follow-up was 36.6 years.40 Outcome parameters included the presence of pain, instability, limitation in activity, abnormal gait, need for special shoes, residual deformity, symptomatic callosities, and successful fusion of all joints. Seven of ten patients maintained a fair to good outcome at the close to 37-year follow-up. Radiological studies showed excellent union rate of subtalar, calcaneo-cuboid, and talo-navicular joints, with none of the patients demonstrating pseudoarthrosis or nonunion. The correction in the tibiometatarsal (TM) angle representing coronal alignment approached an average of 69 degrees in four patients (the control group average TM angle being approximately 110 to postop TM angle in the study group being 131.8 degrees). However, the authors cautioned against overreliance on measuring the TM angle as an indicator of surgical success since it did not necessarily correlate with clinical outcomes. The outcomes suggest that although the range of motion is less than that of a transfer, fusion is a viable salvage procedure that resulted in improvement in ROM and pain in those patients. So et al concluded that Lambrinudi is a reliable surgical choice, especially for polio patients with fixed equinus deformities in improving outcome and deformity correction.40
In patients with some residual strength in PTT, Elsner et al described a combined procedure – a Lambrinudi arthrodesis with PTT to the lateral cuneiform.39 This procedure uses the fusion to address the rigid bony component of foot drop, but also uses PTT for more dynamic ankle stability and dorsiflexion. In 39 month follow up of 19 patients who had previously failed conservative treatment and eventually underwent the above procedure, the AOFAS Hindfoot Score improved from 38.9 preoperatively to 73.2, and SF-36 scores improved from 38.3 to 70.5, with all patients able to wear normal shoes. While active plantarflexion in a seated position decreased from preoperatively 52 degrees to 22 degrees, active dorsiflexion increased from 0 to 10 degrees. In a standing position, all patients were able to lift their forefoot off the ground. Pain levels improved from a preoperative AOFAS score of 20 to a postoperative score of 40 and VAS decreased from 3.4 to 1.8 . Elsner et al showed that the combined procedure of Lambrinudi arthrodesis with an additional PTT transfer provided a stable correction of the adult foot drop in patients with a significant flail or rigid deformity of the transverse tarsal joint.39
Conclusion
Foot drop due to peroneal nerve palsy is a complex problem arising from various etiologies. As a result, all patients are not the same and there is no universal solution when operative options are considered. This article presents and evaluates the common surgical procedures used to address foot drop. By highlighting these options and their outcomes, this can hopefully assist surgeons in determining the ideal treatment plan for each patient.

Author’s Contributions
Kyle L McCormick MD: Literature search, manuscript writing, manuscript editing, submission
Dev Patel BA: Manuscript editing
Bonnie Y Chien MD: Mentorship, manuscript editing
Justin K Greisberg MD: Mentorship, manuscript editing
Ettore Vulcano MD: Mentorship, manuscript editing
Conflict of Interest
The authors declare that they have no conflict of interest.