

Introduction
Acromioclavicular (AC) joint injury is a common entity. It accounts for about 50% of shoulder girdle injuries from sports.1 It also constitutes 9–12 % of all shoulder injuries following fall on an outstretched hand.2,3 The approach to treat this injury has been evolving from the days of Hippocrates4,5 and Galen.5 The classification system that is most commonly used is that proposed by Rockwood. It classifies this injury into six types.6 Type I, represents ligamentous sprain, type II is AC joint subluxation, type III is superior dislocation less than 100%, type IV is posterior dislocation, type V is high (more than 100%) superior dislocation and type VI is inferior dislocation.6 There is a general consensus to treat Rockwood type I and II injuries conservatively and Rockwood type IV, V and VI injuries surgically. However, the most suitable treatment for Rockwood type III injuries remains debatable.7,8 Management options for AC joint injury range from bandages and slings to multiple surgical procedures including fixation with pins, tension band wiring, coracoclavicular screw, the modified Weaver-Dunn operation, tight loop and clavicular hook plate. Each of these methods show advantages and disadvantages, however, none has proved most superior as yet.9 In addition, distal clavicle fracture comprises 15% to 25% of all fractures of the clavicle and its treatment depends on the classification of the fracture.10 Three types have been described by Neer according to the relationship of the fracture to the coracoclavicular ligaments and acromioclavicular joint.11 Type I fractures occur between the acromioclavicular joint and the coracoclavicular ligaments while type III fractures extend into the acromioclavicular joint. These 2 types are stable with minimal displacement and are usually managed nonoperatively. Neer type II fractures occur proximal to the coracoclavicular ligaments and are usually markedly displaced due to coracoclavicular ligaments rupture, resulting in a high incidence of nonunion ranging from 21% to 44% with nonsurgical management.11–13 If a surgery is indicated, devices such as K-wires, tension band wires and plates can be used.14 Hook plate is a hardware option that is suitable for both AC joint dislocation and distal clavicle fracture. It is simple to use and it shows mechanical properties comparable to those of the original AC joint.15,16 Therefore, it is advantageous to encourage joint and bone healing while starting mobilization early in the postoperative period.17 However, despite these advantages, the hook plate is associated with several problems. The pressure induced by the hook under the acromion induces osteolysis (erosion).18,19 Also, because it permits the normal biomechanics of the AC joint to be maintained, the hook moves freely as the clavicle rotates and elevates resulting in subacromial impingement, rotator cuff injury, arthritis of the AC joint, and ossification of the coracoclavicular ligament.20 Therefore, the manufacturers of the hook plate recommend removal of the plate after 3 to 4 months to avoid these complications. So, despite that the hook plate has become a valid option for AC joint dislocation and distal clavicle fractures during the last years, many surgeons do not prefer to use it. The reasons include unfamiliarity with the technique, lack of certainty about the patient’s functional and cosmetic outcome, the association of the plate with complications and the need for early removal. The aim of the study is to evaluate the clinical and radiological outcomes and the complications of hook plate fixation in AC joint dislocation and distal clavicle fracture as well as to compare these outcomes and complications between these two categories.
Materials and methods
This was a prospective observational study. The study protocol was approved by the Ethics Committee of our hospital. We followed the patients of AC joint dislocation and distal clavicle fracture treated with a hook plate from November, 2017 to February, 2023. The inclusion criteria for AC joint dislocation included acute (within 2 weeks) Rockwood types III and V and a minimum 12 months follow up period after removal of the plate. For patients with distal clavicle fracture, the inclusion criteria included Neer type II and a minimum of 12 months follow up after removal of the plate. The exclusion criteria included other types of AC joint dislocation and distal clavicle fracture, chronic injury, bilateral and multiple injuries and history of previous stiffness, arthritis, rotator cuff lesion, injury, or any operative intervention around the shoulder girdle.
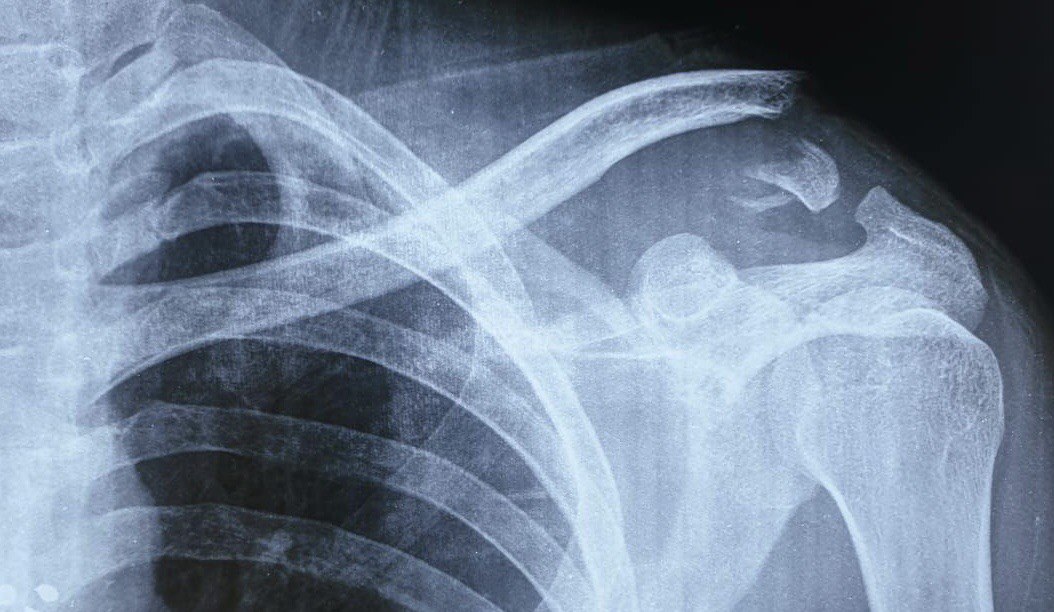
Radiographic evaluation was undertaken preoperatively and during follow up as standard shoulder anteroposterior and lateral scapular Y views for both the index and the normal sides (fig. 1 and 2). Standing stress view was taken in the context of evaluation of the AC joint dislocation.


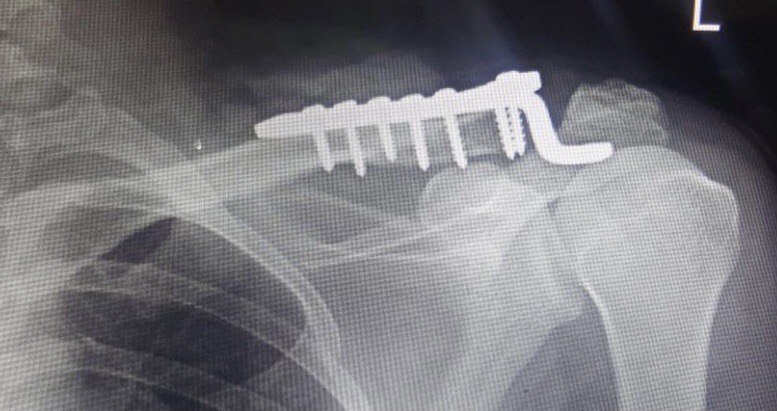
All surgeries were performed in both groups in the beach-chair position under general anaesthesia. A transverse incision was created over the lateral clavicle and the AC joint and dissection was undertaken to expose these structures. In patients with AC joint dislocation, the torn acrmioclavicular and coracoclavicular ligaments were assessed and the AC joint was manually reduced and a hook plate was inserted under the acromion and fixed to the clavicle by screws. The torn coracoclavicular ligament was repaired without augmentation. In patients with distal clavicle fracture, the fracture was exposed, reduced directly and a hook plate was used in a similar fashion and fixed by screws. The hook plates used were 3.5mm LCP titanium plates manufactured by Synthes with 4 to 6 holes and a hook depth of 15 and 18mm (fig. 3 and 4).
._a_postoperative_x-ray_after_open_reduction_and_fixation_.jpeg)
._a_postoperative_x-ray_after_open_reduction_and_fixation_.jpeg)
Postoperatively, all patients were subjected to a rehabilitation program. This included a gradual postoperative range of motion and an arm sling for 4 weeks. Two weeks after the operation, the patients were allowed to move their shoulders to handle daily tasks. After 8-12 weeks, the patients were allowed to move freely. Strength-related activities were permitted 3 months postoperatively. Hook plate removal was scheduled after 4 to 6 months in group I. In group II, the hook plate was scheduled to be removed after confirming bone healing. All clinical data were collected in our database and retrospectively reviewed.
The clinical and radiologic outcomes were evaluated at time of plate removal and then at regular intervals of 3, 6 and 12 months from metal removal time. The Constant-Murley score was utilized for clinical evaluation at these episodes and was assessed by a researcher who was not involved in the patient management. The Constant- Murley scoring system includes individual and clinical functional parameters. These parameters include pain, activity level, arm positioning, strength of abduction, and range of motion.21,22 The radiologic evaluation included standard bilateral anteroposterior and lateral scapular Y views. The subacromial erosion was evaluated on X-ray as described in previous studies18,23 where significant erosion was defined as more than 2 mm. Radiologic assessment of AC joint dislocation and reduction was undertaken preoperatively and regularly during the postoperative follow up by measuring the coracoclavicualr distance (CCD) and comparing it to the contralateral side (in percent) on standing anteroposterior radiograph. The CCD was measured between the upper border of the coracoid process and the lower cortex of the clavicle. Significant displacement after metal removal was defined as an increase in CCD more than 5 mm.
Statistical analysis was undertaken using SPSS Statistics. The null hypotheses were rejected when p-values were <0.05. The Constant-Murley scores were compared between group I and II using an independent t-test while the difference in the incidence of radiographic subacromion erosion between them was analysed using the Chi- square test.
Results
The preoperative data are clarified in table 1. A total of 96 patients (81 men and 15 women) were included in the study. The number of patients with AC joint dislocation (group I) was 64 (57 men and 7 women) while that of patients with distal clavicle fracture (group II) was 32 (24 men and 8 women). The mean age was 36 years (range, 18 to 58 years) in group I and 41 years (range, 19 to 68 years) in group II. Within group II, there were 27 and 37 patients of Rockwood type III and V respectively. There was no significant baseline difference between both groups-in terms of age. In both groups, the dominant side was slightly more involved than the non-dominant side but there was no statistical difference between the two sides. In both groups, males were more significantly affected. In group I, the commonest mechanism of injury was fall on the shoulder or on an outstretched hand due to slipping on level grounds or falling from a height during work (52%). Sport injury was not common (12%) while motor vehicle accidents (MVA) were involved in 27%. In group II, the commonest mechanism was MVA (44%) followed by falling during work (33%) while sport injuries were involved in 9%. There was a statistical difference between the two groups regarding the mechanism of injury.
All operations were undertaken by orthopaedic residents at their senior years or by consultants with an experience of 3 to 10 years. The mean duration of the operation was 42 minutes (35–55 minutes) and 74 minutes (52-110 minutes) in groups I and II respectively. There was a significant difference in operative time between the two groups. The average length of the incision was 84 mm (70–105 mm) and 96 mm (88- 140 mm) in groups I and II respectively. The plate length most commonly used was 4 and 6 holes for groups I (73%) and II (83%) respectively. The most commonly used hook depth was 18 mm in both groups. The average hospital stay postoperatively was 2 days (1-5 days). There were 5 cases (1 in group I, 4 in group II) of postoperative wound infection; they were all managed by conservative methods. Otherwise, there were no postoperative complications. No cases needed premature metal removal. The minimum follow up period was 12 months after plate removal.
Table 2 summarizes some of the postoperative data. Plate removal in group I was undertaken in an average of 5.3 months (range of 4.0-6.2 months). In group II, plate removal was undertaken after confirmed bone healing. This took an average of 8.2 months (range of 7.1 to 11.7 months).
In group I, the average Constant-Murley score at hook plate removal was 60.7 (95 % Confidence Interval between 54.7 and 61.9) as compared to 71.6 and 80.3 at 3 and 6 months after plate removal respectively. At 1 year, the score was 92.1 (95% Confidence Interval between 88.7 and 94.4). In group II, the average Constant-Murley score at hook plate removal was 40.6 (95 % Confidence Interval between 38.7 and 42.9) as compared to 53.8 and 74.1 at 3 and 6 months after plate removal respectively. At 1 year, the score was 89.1 (95% Confidence Interval between 82.7 and 92.4). There was a significant difference in Constant-Murley score between groups I and II at time of plate removal and after 3 months. However, there was no significant difference in this score between the two groups at 6 months and one year after plate removal.
The incidence of subacromial erosion at time of plate removal was found to be 32.8% (21 patients out of 64) in group I in comparison to 62.5 (20 out of 32) in group II. There was a statistically significant difference between the two groups in this regard. The association between subacromial erosion and symptoms (pain and significant limitation of motion) was assessed in both groups. We found that, at plate removal, subacromial erosion was associated with symptoms in 36.2% and 41.7% out of those who developed subacromial erosion in groups I and II respectively. However, there was no statistically significant difference in the incidence of these symptoms between patients who developed subacromial erosion from those who did not within the same group or between patients who showed subacromial erosion in the two groups. The incidence of these symptoms at one year after plate removal decreased to 12.4% and 27% in groups I and II respectively.
The incidence of significant AC joint displacement (at least 5 mm subluxation) after removal of the plate in group I was found to be 17.1% (11 out 64 patients) and 20.3% (13 out of 64 patients) at 6 months and one year respectively. No displacement exceeded 10 mm. The incidence of symptoms within this subgroup of patients (pain, limitation of motion or cosmetic prominence of the clavicle) was found to be 18.2% and 9.6% at 6 months and one year respectively with no significant difference from patients who did not show AC joint displacement after plate removal.
The relation between the Constant-Murley score and the number of years of experience of the operating surgeon was evaluated. The number of patients who achieved a high Constant-Murley score of 88 and more after 1 year from plate removal in both groups was 76 (80.8%); out of these patients, 46% and 38% were operated on by surgeons who had an experience of 5 years and more and 2 years and less respectively. However, there was no significant difference between these two subgroups.
In group II, there were 3 (9.3%) cases which developed partial nonunion. However, no complications requiring revision surgical procedures were recorded in either group. There were no cases of metal failure or re-fracture.
Discussion
The aim behind this study is to evaluate the results of hook plate fixation for cases of AC joint dislocation and distal clavicle fracture in terms of clinical and radiological healing, patient’s satisfaction and any possible associating complications. We also compared the outcomes of these two injuries. The demonstration of such outcomes can help orthopaedic surgeons to become more familiar with such a modality of treatment as it is still considered as a relatively new method at least in our locality and those regions of a similar setup. The overall final clinical results were found to be good in both groups as was reported in other studies which indicated that hook plate fixation is a safe and effective option in these injuries.20,24–28
Different fixation methods were tried for AC joint dislocation and distal clavicle fractures before using the hook plate. These included the K. wires, the tension band wiring, coracoclavicular screws and plates of various types.29–32 A significantly high rate of complications was linked to these fixation methods including metal loosening, failure and migration.33 Moreover, the distal clavicular fractures pose a surgical difficulty as it is needed to achieve a good stability while maintaining adjacent joint motion and avoiding metal complications in such high stresses region.
Taking these considerations into account, using the hook plate to treat AC dislocation and distal clavicular fractures has become increasingly popular in the last decade.34 The hook plate is associated with a good mechanical purchase to both the acromion and the clavicle while it preserves the mobility of the AC joint. Moreover, it is a relatively simple procedure with a minimal dissection required.
However, the hook plate needs a second operation to remove it as its undue retention is associated with problems of subacromial erosion, frozen shoulder, or rotator cuff injury. Studies have denoted that retaining a hook plate for greater than 5 months can cause increasing incidence of subacromial erosion and unfavorable functional scores.35,36 There is no consensus about the optimal time of hook plate removal. However, it is generally accepted to remove the plate as soon as the ligamentous healing or bone union has been achieved.23
In our study we found that the Constant-Murley score at time of plate removal and at 3 months after is better among patients of group I than group II. This can be explained by the relatively earlier hook plate removal in group I (average of 5.3 months as opposed to 8.2 months in group II) as ligamentous healing takes shorter time than bony healing. So, it is concluded that the longer the retention of the plate, the lower the functional score is to be expected. However, we also found that the difference in the functional score between the two groups became nonsignificant after 6-12 months. This denotes that the functional score keeps improving after the plate removal. In a study by Joo Han Oh et al37 they compared the Constant-Murley score between two groups of AC joint dislocation and distal clavicle fractures treated by hook plate. They found that at time of plate removal, the score was good and not significantly different between the two groups despite they removed the plate at an average of 6 and 9 months in patients with AC joint dislocation and distal clavicle fractures respectively. The difference in results might necessitate more studies in this regard but with larger sample size.
In the current study, we found that the incidence of significant (more than 5 mm) AC joint displacement at 6 months and 1 year after plate removal in cases of AC joint dislocation was 17.1 % and 20.2% respectively. There was no significant association between such displacement and symptoms as compared to patients who showed no radiographic displacement. Moreover, despite that the displacement was found to be slightly higher at 1 year after plate removal, the incidence of symptoms was less. The significance of such findings is that simple repair of the the coracoclavicualr ligament as in our study was an adequate adjunct to hook plate fixation to avoid symptomatic AC joint displacement after plate removal. Similar results were obtained from other studies.38,39 However, in a study by Chung-Ting Liu et al,40 they recommend coracoclavicular ligament augmentation specially for cases of AC joint dislocation type V as they found that the incidence of subacromial erosion and AC joint displacement were higher when no ligament augmentation was undertaken. We think that ligament augmentation entails more soft tissue dissection and more operative time and that simple ligament repair is adequate.
In this study, we found that a high Constant-Murley scores after one year from plate removal were achievable by orthopaedic residents as well as by senior consultants with no statistically significant difference in the final outcome between patients operated on by these two categories of surgeons who had different levels of experience. This indicates that this operative procedure is simple to perform even by resident doctors provided that it is undertaken under supervision of their more experienced team members.
The limitations of this study include the relatively small sample size. The Constant-Murley score was used to evaluate the outcomes of these shoulder procedures while the numeric evaluation of each part of the range of motion was not considered. Furthermore, we used plain radiographic assessment of the shoulder. MRI and CT scan studies imply a better evaluation of the injury and the surgical outcome. MRI is specially of value to assess the ligamentous element of the injuries involved in this study. Also, we think that the subacromial erosion is to be better assessed on CT scan. A similar consideration applies to the bony union in clavicle fractures in group II which would be better evaluated by CT scan. The AC joint dislocation is not a part of group II injuries. The possibility that this might have affected the final clinical outcome cannot be ruled out. Also, we think that a longer follow up could be necessary for such injuries.
Conclusion
The clinical results of hook plate fixation were initially better for patients with ACJ dislocation than distal radius fractures due to shorter time between fixation and plate removal. However, on the long run, the results were good in both categories of patients after plate removal. The subacromial erosion was higher in patients with distal clavicle fracture since they had to keep the plate for a longer time; however, there was no strong relationship between the subacromial erosion and any untoward functional outcomes. In summary, the hook plate fixation is a valid option for the mentioned injuries and is easy to perform even by surgeons with limited experience. However, it needs plate removal as soon as healing is achieved.
Acknowledgement
Acknowledgement to the Iraqi Ministry of Higher Education and Scientific Research for funding this study and to Dundee University, UK for collaboration.
Conflict of interest
We declare no conflict of interest.
Ethical standards
Approval of the Ethical Committees of the Al Hussein Teaching Hospital, College of Medicine, University of Thi Qar was obtained before any data were collected. Written consent was obtained from all patients and/ or their parents/guardians.
Funding
The research is funded by the Iraqi Ministry of Higher Education and Scientific Research.