INTRODUCTION
Legg-Calvé-Perthes disease (LCPD) is known as a self-limiting pediatric orthopedic pathology that affects the hip due to ischemia with consequent aseptic avascular necrosis of the femoral head. It can cause a subchondral stress fracture with subsequent bone resorption and repair, resulting in growth disorders such as: femoral head deformity, joint deformity and/or degeneration.
Patients usually report pain in the injured joint, which intensifies during or after exercise and also affects the range of movement of the hip. However, trendelenburg gait or claudication is characterized as the main sign.1 The main complaints are pain localized in the hip with irradiation to the thigh and knee and claudication; however, some cases present painless claudication.
Described in 1910 in the United States as an obscure disease of the hip joint, it later evolved into pseudocoxalgia and currently the concept developed in Germany prevails that it is a juvenile deforming arthrosis, more prevalent in males, with onset in the 4-9 year age group and with bilateral involvement in around 10% of cases.2
Its incidence varies between 0.4/100,000 and 29.0/100,000 children under the age of 15.3,4 It usually appears between the ages of 4 and 9, with an increase in prevalence between the ages of 5 and 7. Bilateral involvement is seen in 10 to 24% of patients and the disease is up to five times more common in males.5,6
It is common to find limited internal rotation and abduction, as well as limited hip flexion of approximately 20 degrees.7 In some patients, there is shortening of the affected extremity, and most of these symptoms are related to loss of hip joint alignment.8,9
Radiography used to be the gold standard for confirming the diagnosis, even if it failed in the early stages of the disease. Another possible test is bone scintigraphy, which can show regions of ischemia, delimit the degree of involvement of the epiphysis and its revascularization. Another possible imaging resource is magnetic resonance imaging, which is useful for showing early necrosis, extension and the sphericity of the femoral head, which helps with preoperative management, especially to assess better joint congruence in cases of femoroacetabular subluxation.10,11
Considering the natural history, it is well established in the literature that 57% of cases have a good evolution and prognosis even without treatment. However, 20% have poor outcomes regardless of treatment. The aim of this study is therefore to compare the effectiveness of treatment for Legg-Calvé-Perthes disease in relation to its staging: the limits of conservative treatment.
MATERIALS AND METHODS
It consists of a systematic literature review, built according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). In addition to a four-phase flow diagram, it prioritizes clarity and transparency in the execution of the systematic review and the selection of studies.12 The search for articles took place in September 2023, in the databases linked to the Medical Literature Analysis and Retrieval System Online (MEDLINE), and the SPICE strategy was used to identify the relevant studies:
-
Setting: patients with Legg-Calvé-Perthes disease
-
Perspective: individuals undergoing a surgical or conservative approach for the treatment of Legg-Calvé-Perthes disease.
-
Intervention: Surgical correction
-
Comparison: Stulberg classification for analyzing the effectiveness of established treatments.
-
Evaluation: effectiveness of the surgical technique.
The descriptors in health sciences (DECS) / MESH TERMS were used in combination, according to the following structures: “Legg-Calvé-Perthes disease” OR “Perthes disease” AND “Orthopedic procedures”.
Inclusion and exclusion criteria
Studies with these criteria were included: (1) age group < 18 years (2) patients undergoing surgical and/or conservative treatment for Legg-Calvé-Perthes disease (3) evaluation of the Stulberg scale (4) studies published between 2008-2023 (5) original studies.13
The exclusion criteria were: (1) experimental animal studies (2) non-original studies - literature reviews (3) opinion studies (4) studies that did not meet the other criteria mentioned above.
The studies were selected by two reviewers who independently analyzed the studies. The DECS and Boolean operators above were used to select studies published in the last 15 years (2008 - 2023).
The systematic review was registered in the International prospective register of systematic reviews (PROSPERO) under ID CRD42023491081.
RESULTS
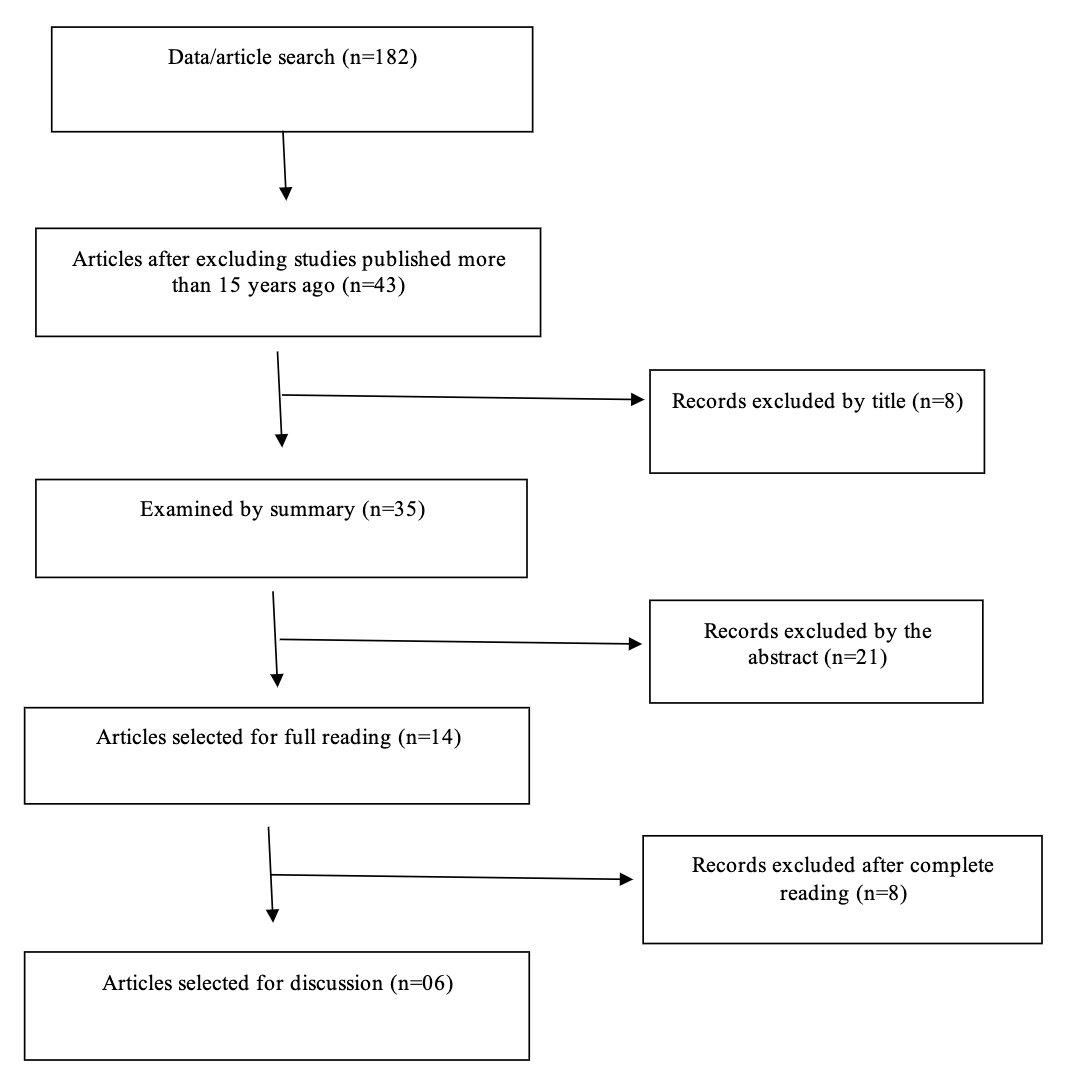
Initially, 182 articles were selected, from which those with more than 15 years of publication were excluded, leaving 43 papers. The titles and abstracts were analyzed in relation to the approach used for the treatment of Legg-Calvé-Perthes disease, and 29 articles were removed, with 14 selected for full reading. At the end of the process, 6 articles were chosen.
Figure 1 shows the flowchart used to select the articles using the PRISMA methodology (Figure 1).

The six articles selected involved children with Legg Calvé Perthes disease undergoing surgical or conservative treatment for the condition. The Stulberg classification was analyzed, which is based on the radiological aspects of the hip joint in the active and maturation phases and is a strong predictor of the disease’s prognosis. A total of 356 patients were included. Of these, 87 underwent surgical treatment and 269 underwent conservative treatment.
Table 1 contains Stulberg’s classification.14–19
Table 2 shows the Stulberg classification of patients undergoing surgical or conservative treatment for Legg-Calvé-Perthes disease.14–19
Conservative treatment was used in four studies. In Arkader et al,14 21 children were in the conservative group, of whom 15 underwent adductor tenotomy, plaster cast or abduction brace and physiotherapy, and 6 underwent physiotherapy only. Of the 22 children who underwent surgical treatment, 16 underwent femoral varus rotation osteotomy (VDRO) and 6 Chiari pelvic osteotomy (CPO). In this study, there were twice as many Stulberg III patients in the conservative group compared to the surgical group.
Nakamura et al. showed that 76% of patients who underwent flexion varus osteotomy (FVO) had good radiographic results (Stulberg class I or II), while 36% of the conservatively treated group fell into this class. In the study by Alves et al, all the patients underwent conservative treatment, in which, according to the Stulberg criteria, 23.00% were in class 1, 30.00% in class 2, 2.27% in class 3, 12% in class 4 and 8.00% in class 5.
In Rosenfeld et al’s study, treatment was carried out using Atlanta braces and splints, with one hundred and fifty-six results (81%) being good (Stulberg class I or II), seventeen (9%) fair (Stulberg class III), and nineteen (10%) poor (Stulberg class IV). In the study by Bhuyan et al, all patients underwent osteotomy, ten patients had good results (Stulberg class I and II), eleven fair (class III) and two poor (class IV).
Pecquery et al. showed that of the twenty-one patients (mean age 10.4 years) who underwent surgical treatment, thirteen had good results (Stulberg class I and II), four fair (class III) and four poor (classes IV and V).
DISCUSSION
The Stulberg classification has significant value in assessing radiological results in patients with Perthes’ disease, making it possible to determine the prognosis of the disease. The results of this study show that there is still a lack of consensus on the factors that interfere with the ideal treatment for the disease. However, it was possible to observe that patients over the age of six who were treated conservatively had higher Stulberg scores than those who underwent surgery. It can therefore be said that conservative treatment is more effective in younger patients with less advanced disease, but is less effective in older patients with signs of a worse prognosis.20,21
Much has been discussed in the literature about the constitutional factors of the pathology in question, such as the abnormal growth of children. Delayed musculoskeletal development is present before the onset of the disease, but bone maturation returns to normal after the disease is cured. Birth weight is lower in children diagnosed with Perthes’.22
There are possible anomalies associated with a higher prevalence of hernias, ectopic testicles and renal anomalies in women. The etiology is not well described, but it is produced by avascularization of the femoral head. Biopsies usually reveal stages of necrosis and experimental studies have shown that the epiphyseal vessels that reach the femoral neck between the bone and the capsule (inelastic) are susceptible to increased hydrostatic pressure in the hip: worsening clinical symptoms. On the other hand, there is a causal relationship between Perthes disease and transient synovitis of the hip, as 1.5% to 18% of cases of synovitis develop into Calvé.2,4
In the initial phase, the clinical manifestation resembles transient synovitis, with claudication predominating over pain, abduction and internal rotation with limitations and only after an initial period of joint irritation does discomfort begin. There is atrophy of the thigh muscles with consequent flexion-adduction contracture and shortening of the affected lower limb. The use of complementary tests allows the disease to be differentiated and classified, for early treatment and reduction of sequelae.23,24
Firstly, in the avascular phase, the increase in calcium in the necrotic bone makes it favorable to microdamage, which affects the mechanical properties of the femoral head. Necrosis leads to damage to bone cells, osteoblasts and osteoclasts, causing microfractures to go unidentified and/or unrepaired. Then, in the revascularization phase, the necrotic bone will be resorbed, further affecting the mechanical properties.11 The hip is one of the main load-bearing joints, so it is important to consider the forces applied to the joint, as these influence the degree of deformity of the femoral head. The duration of each phase varies greatly, however, in general, the necrosis and fragmentation phase lasts around six months; the reossification phase, from 18 months to three years; and the final phase, until bone maturity.25
Femoral head deformities occur when the forces applied to the femoral head are greater than its capacity to resist the deformity, from a mechanical point of view.26 One study observed that the mechanical properties of devascularized bones are compromised as a result of various mechanisms that occur during the different stages of the disease.27
In the treatment of LCPD, one of the big questions is which therapeutic option to start with, a conservative or operative option, in order to improve the final clinical and radiological outcome. It is necessary to have in-depth knowledge of the natural evolution of the disease, as well as the potential benefits of the different modes of treatment available.28
Today, there is a growing global consensus among pediatric orthopedic surgeons that surgical therapeutic methods are preferred in cases of severe involvement of the femoral head and late onset of the disease. On the other hand, conservative therapy is initiated in cases of mild severity and/or early onset.29,30
Conservative treatment, such as weight relief, abduction splints and range-of-motion therapy, was indicated by pioneering orthopedic doctors. Today, however, non-surgical treatment focuses in particular on reducing mechanical stress with additional observation and physiotherapy. There is growing agreement in the pediatric orthopedic community that the presentation of DCL at an age < 6 years is related to a more favorable outcome, justifying a non-surgical approach.26 However, surgical treatment is necessary in hips with late presentation (>6 years) of the pathology and greater severity in the initial presentation, to prevent deformity of the femoral head and subsequent probable early osteoarthritis.31,32
Numerous surgical and non-surgical treatments for LPCD have been established.27 The primary objective of the operative options is to contain the femoral head within the acetabulum to prevent deformation of the femoral head and premature osteoarthritis of the hip. This is made feasible by varus femoral osteotomy, an innominate osteotomy and other forms of pelvic osteotomies, such as Pemberton or Dega acetabuloplasty and triple osteotomy.29 Chiari osteotomy and shelf arthroplasty are considered salvage procedures. They help to improve acetabular coverage, but lead to incongruity of the hip joint. Surgical treatments can be divided into femoral, pelvic and combined procedures.33
In general, surgical treatment is not indicated in the early stages, which present total and painless range of motion of the hip and are of low radiological risk in relation to the femoral head, such as Catterall grades I or II and Salter and Thompson group A. Patients with a larger area of injury to the femoral head may be candidates for surgical treatment, such as innominate osteotomy of the pelvis or osteotomy of the hip stem, in order to keep the femoral head as congruent with the pelvis as possible. Shelf arthroplasty has been indicated for children over 08 years of age or in Catteral groups III and IV.34,35
Since the degree of deformity of the femoral head varies between patients, treatment is decided according to the particularities of each case.33 Therapeutic options range from monitoring and observation to surgical procedures on the femur and hip.32 The choice depends on the stage of the disease, the radiographic characteristics of the joint restraint and the patient’s clinical condition.33 However, all treatments are aimed at preventing deformity of the femoral head, maintaining the sphericity of the femoral head and the congruence of the femur-acetabulum relationship and avoiding secondary degenerative arthritis, which leads to total hip arthroplasty in 5% of cases. Early diagnosis and treatment help prevent collapse, progressive deformity and impingement of the femoral head.36
CONCLUSION
Patients with Legg-Calvé-Perthes disease differ in therapeutic typology according to age group. This translates into a scenario of diagnostic urgency for a better functional outcome and reduced risk of exposure to complications and procedures. The Stulberg classification is a strong predictor of prognosis for the disease, since the cases with the worst evolution are characterized by deformity with loss of sphericity, as well as flattening of the femoral head, anomalous epiphyseal development, varus thigh, osteonecrosis and differences between the sizes of the lower limbs. The data collected by the studies, although with insignificant differences in terms of the number of patients classified in each Stulberg class for conservative and surgical treatment, showed that conservative treatment is more effective before the age of six, associated with a better prognosis, while surgical treatment is better recommended at older ages, or in cases of failure of conservative treatment applied at the indicated age (<06 years).
This study has no conflicts of interest.