Abbreviations
L2,3,4 2nd, 3rd, 4th lumbar vertebrae
CM Centimeters
MRI Magnetic resonance imaging
STIR Sagittal T2 short tau inversion recovery
1. Introduction
The quadriceps femoris is an important group of four muscles (rectus femoris, vastus lateralis, medialis, intermedius) situated in the anterior thigh compartment. Because its origin and insertion span the hip and knee joints, it plays a major role in individuals’ abilities to perform everyday activities, such as walking and running, by functioning to dynamically stabilize the hip and knee joints, flexing the hip and extending the knee, and maintaining posture and balance. The direct and indirect heads of the rectus femoris muscles arise from the anterior inferior iliac spine and the superior acetabular ridge, respectively, and inserts onto the patella via the quadriceps femoris tendon.1 The muscle is innervated by the femoral nerve arising from the 2nd, 3rd, and 4th lumbar vertebrae (L2, L3, and L4), and its blood supply comes from the femoral artery. Injuries to the rectus femoris muscle are often seen in athletes playing sports involving swinging and kicking motions, as in American football, rugby, and soccer. The incidence of rectus femoris injuries has not been reported widely in the literature due the high force and rare occurrence of such injuries. Most cases published today involve professional athletes of different sports and age groups. The significance of this topic lies in the fact that these types of high-grade muscular injuries are uncommonly seen in nonprofessional athletes, and little evidence about the topic has been published in the literature, even on the professional athlete’s side. Thus, there are no reliable guidelines for the management of these high-grade injuries. This case report study presents a rare and unique case of a grade III direct head of rectus femoris myotendinous tear in a young recreational athlete. Our aim in this study was to report an important scientific observation that was encountered in a clinical setting and to explore the diagnosis and treatment outcomes available in the published studies, leading to expanding our knowledge base and complementing the scientific literature. Grade III injuries to the rectus femoris muscle can cause prolonged morbidity even for young patients, as they could require surgical interventions with either proximal tendon excision, suture reattachment, or tendon repair using suture anchors, followed by an extended rehabilitation program. Therefore, more studies on the prevention and treatment of these injures are needed.
2. Case Presentation
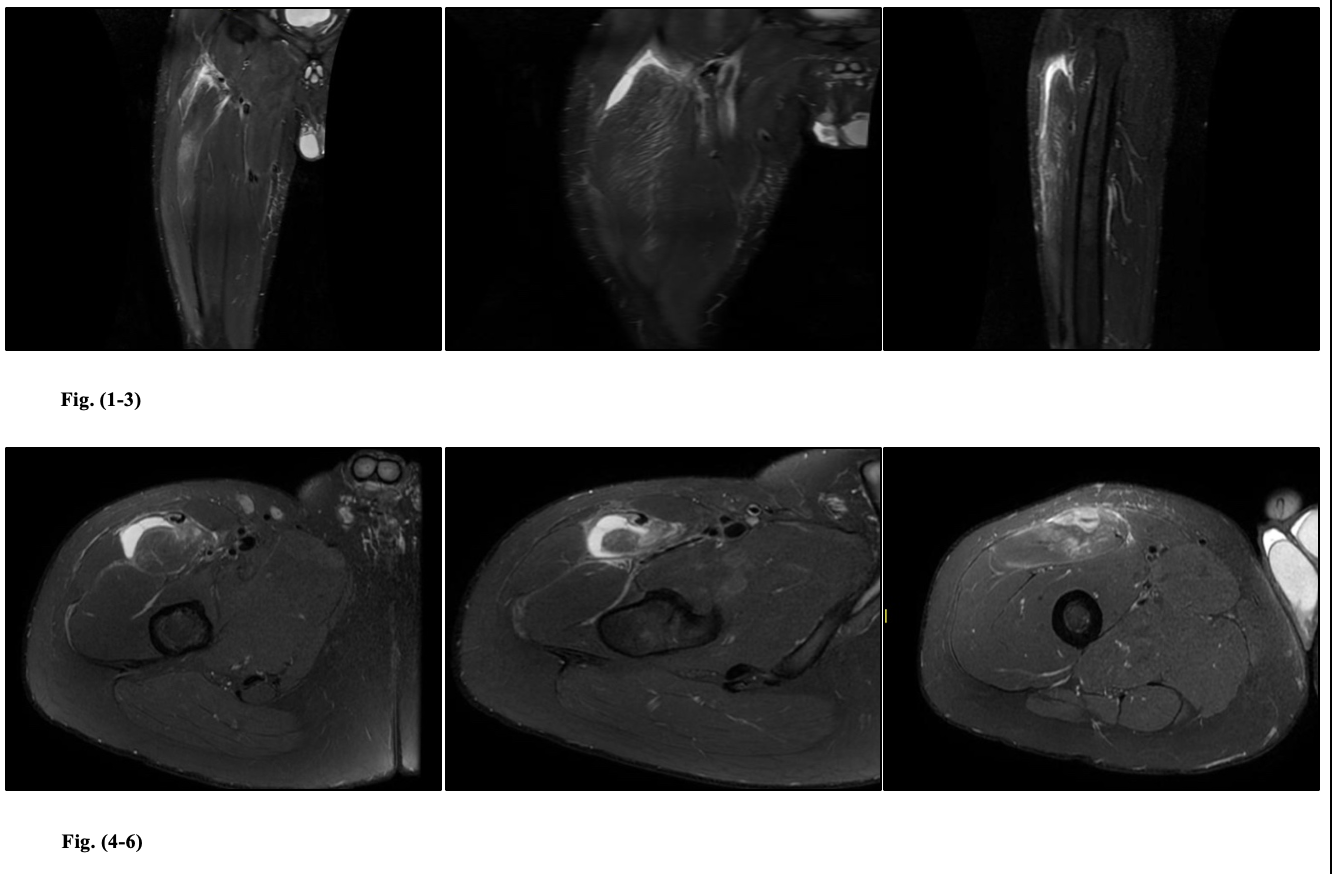
A 37-year-old healthy male presented to the clinic with right mid-thigh pain and difficulty bearing weight on the affected leg after a football match. The patient described the injury as severe anterior thigh pain following a failed attempt of kicking the ball using his right dominant leg and with full force. Clinical examination showed antalgic gait and no palpable mass or ecchymosis but severe pain on palpation of the right rectus femoris muscle. Range of motion of the right hip and knee was preserved but with severe pain associated with loss of strength. The patient was started on analgesia for pain control and given instructions for rest and elevation with ice-packing and protected weight bearing with crutches. The patient was followed up after 1 week. The pain had improved, but he was still depending on crutches for mobilization. Examination of the right thigh showed that lower thigh ecchymosis had developed, and proximal palpation of the rectus femoris muscle induced severe pain. In addition, right hip and knee motion were affected by loss of strength. A magnetic resonance imaging (MRI) scan of the right thigh was requested for confirmation and injury staging and illustrated a near complete tear of the proximal right rectus femoris direct head musculotendinous junction, with partial distal retraction (7.22 cm; Figures 1-3). A small central gap with focal central intramuscular hematoma (7.5 cm × 3.15 cm × 1.3 cm; Figures 4-6). The scan showed also partial residual edema surrounding the muscle fibers with partial residual anterior thigh subcutaneous edema and muscle fiber edema involving the visualized distal musculotendinous junction of the right iliopsoas muscle. The diagnosis and future management were discussed with the patient, and he was consulted regarding the nonoperative and operative options for his injury. The patient was started on a nonoperative physical therapy rehabilitation program and planned to be followed in the outpatient clinic regularly.
3. Discussion and Conclusion
Rectus femoris is the most common injured muscle in the quadriceps muscle group. The occurrence of rectus femoris injuries to nonprofessional (recreational) athletes is only seen seldomly in the literature. Muscular tears of the rectus femoris can be classified as mild (grade I), moderate (grade II), or severe (grade III) based on patients’ symptoms and degree of strength loss on physical examination. MRI grading is derived from the extent and severity of the injury. Focal high signal intensity (grade I), partial tear (grade II), complete tear with or without muscle retraction (grade III).2 Multiple risk factors have been mentioned in the literature in association to rectus femoris tears, including intrinsic factors such as functional lower limbs asymmetries in soccer players.3 Other factors, such as muscle tightness and lack of flexibility, have also been studied as possible risk factors for muscle injuries in young athletes.4 The mechanisms of these injuries are usually seen with eccentric contraction in activities requiring sudden force of hip extension and knee flexion, as in kicking and running. A patient will present with anterior thigh pain with various degrees of severity that can be associated with different levels of decreasing muscular strength and weight-bearing status. These tears are diagnosed using history and physical examination combined with advanced imaging studies. MRI has always been considered the tool of choice for the diagnosis and classification of these injuries.5 MRI is a powerful tool that clinicians use to identify the exact location of the muscular tear, as it can involve the origin of the muscle, its myotendinous junction or insertion site. In addition, a clear severity classification and grading of the of the tear can be obtained from these images. Other associated findings can also be noted, such as muscle retraction, formation of hematoma, and development of myositis ossificans.5 The advantages of using MRI as a diagnosis modality can extend to determines the chronicity of the injury, as old tears will illustrate a distinguish findings of fibrous changes and muscle atrophy.6
__right_thigh_coronal_and_sagittal_t2_hort_tau_inversion_recovery_(stir)_showing_extens.png)
Rectus femoris muscular tears have been widely treated conservatively, with no clear guidelines in the literature. Grade III rectus femoris tears are near complete or complete tears that can affect the origin of the muscle direct or indirect head, the myotendinous junction, the muscle intrasubstance area, and the insertion point at the upper pole of the patella. Treatment can be nonoperative or operative, depending on the patient’s physical and physiological condition, activity demands, and future expectations. Other factors to be considered in the management decision are patient age and physical status, whether the patient is a professional or recreational athlete, and the patient’s compliance with physical therapy or a postoperative rehabilitation program. Bogwasi et all (2023) systematic review have concluded that successful conservative treatment has offered the fastest return to play for all proximal rectus femoris injuries. First line surgical intervention was a more suitable option for elite athletes, due to a faster return to play time compared with failed non operative cases that required surgery later on. In a similar case study , nonoperative management of a high-grade musculotendinous rectus femoris injury in a recreational athlete has shown a similar return-to-play time between elite athletes and recreational athletes.7 Conservative management was also discussed in a case series of 11 patients; all athletes with proximal muscular avulsions were treated nonoperatively and had a high chance of returning to professional American football.8 However, failed nonoperative treatment cases tend to heal with fibrosis and scar tissue formation, causing chronic pain and decrease strength that may obligate further surgeries for scar excision.9,10 These cases necessitating a later surgical intervention were reported in a group of 5 athletes with chronic symptomatic tears of the reflected head of the rectus femoris; ultimately, all patients post operatively returned to collegiate-level athletics.11 First line surgical treatment with suture anchor repair is continuing to show good outcomes in the literature, allowing athletes to eventually return to their preinjury level of play.12 Multiple short- and long-term complications were associated with the operative treatment, including symptomatic lateral femoral cutaneous nerve neurapraxia and recurrent proximal rectus femoris avulsion injuries within 6 months of surgery.13 In conclusion, proximal rectus femoris muscle injuries can present with a variety of symptoms and examination findings, high clinical suspicion is needed in these cases, Our case report had shown that conservative treatment with early physical therapy program had improved patient pain and functional outcome score . Similar positive results were seen in other case studies adhering to conservative management. Future studies and evidence-based research are needed on the subject. Furthermore, the development of a validated functional outcome assessment for such muscular injuries is required, for accurate measurement of patient prognosis and treatment satisfaction.
Declaration
-
The author declare he has no competing interests in this study (financial or nonfinancial).
-
IRB Approval: Institutional review board approval obtained
Acknowledgment
- The author would like to thank Dr. Sulaiman Al Habib Medical Group (HMG) for providing access to the data used in this study