
The introduction
The sensation of a sudden jerk experienced when moving a joint is known as snapping syndrome.1,2 Notably, medial hamstring snapping is infrequent.1–6 Osteochondroma is the predominant benign bone neoplasm. Typically, it originates in the metaphyseal area of the developing skeletal structure surrounding the knee and proximal femur.7–10 It tends to manifest without symptoms, although manifestations may arise from compression of adjacent tissues or from a traumatic impact.7,11
We present a rare case of medial hamstring snapping knee syndrome caused by a proximal tibial osteochondroma, an exceedingly uncommon condition with only one previous report.12
Ethical Considerations
The patient provided written consent for his case presentation.
Case presentation
A 21-year-old female visited the orthopedic clinic with a 4-month history of persistent left knee pain. Her pain began after falling on both knees while carrying heavy items up the stairs. Gradually, she felt a clicking sound and pain on the lateral side of her left knee, along with a snapping sensation on the posteromedial side. The symptoms persisted and intensified during activities such as ascending and descending stairs, kneeling, and walking. The patient was prescribed NSAIDs without improvement. Subsequently, she was referred to a hospital for physical therapy but discontinued it after two weeks due to increased discomfort. Her range of motion remained unaffected, and she had no history of locking, giving way, or knee swelling. She did not recall any significant past injuries and had no prior medical or surgical history.
Upon examination, her knee showed no obvious deformities, significant swelling, abrasions, discoloration, or abnormal warmth. Palpation of the left knee revealed tenderness in the lateral patellar retinaculum along with pain during the patellar compression test, while snapping of the medial hamstring occurred during active extension and flexion without any associated pain. There was no effusion, and the knee exhibited a full range of motion. She was neurovascularly intact in both lower extremities.
Plain radiography revealed a protuberant bony mass at the proximomedial aspect of the tibia, with no fracture, dislocation, or significant joint space abnormalities (Fig.1A and 1B).
_ap_view__(b)_lateral_view_x-ray_of_the_patients_left_knee_reveals_a_bony_exostosis_(w.png)
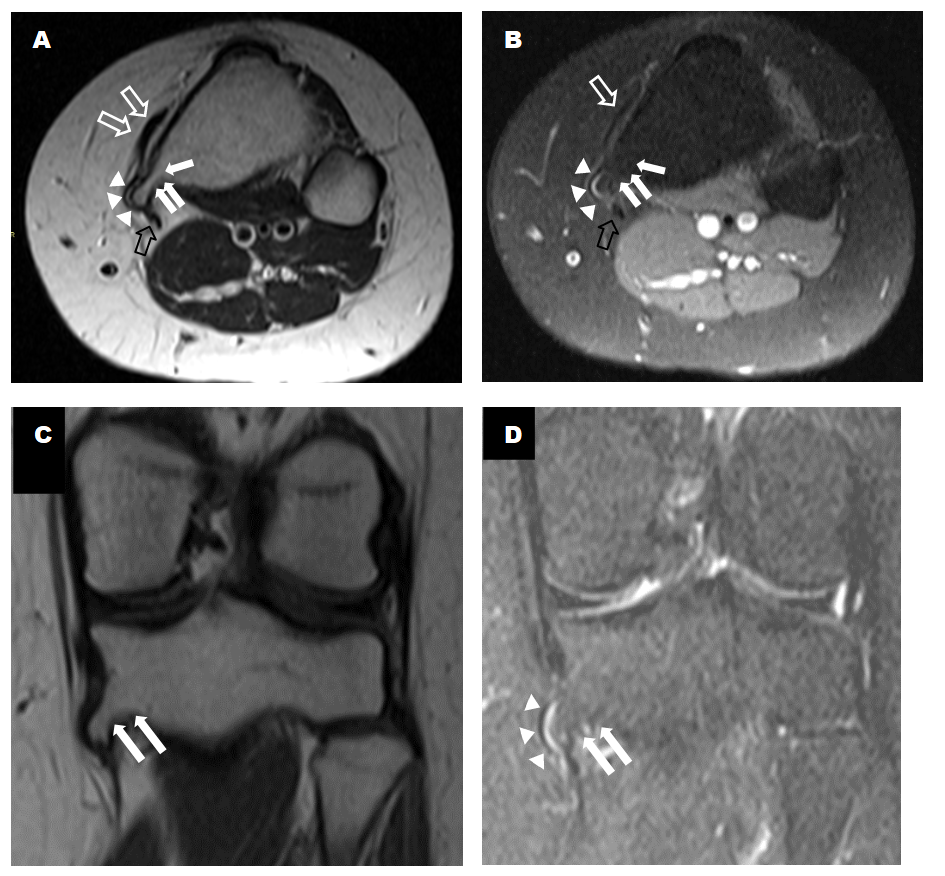
Further investigation with magnetic resonance imaging (MRI) revealed a small bony overgrowth, approximately 1 cm in size, along the medial aspect of the proximal tibial metaphysis. This overgrowth, identified as a pedunculated osteochondroma, showed cortical and medullary osseous continuity. No significant underlying bone marrow edema or pathological fracture was evident. Additionally, there was no cartilage cap thickening or aggressive features (Fig.2A, 2B, 2C, and 2D).
_axial_t2__(b)_axial_pdfs_(c)_coronal_t1__(d)_t2fs_mri_weighted_images_showed_proximal_.png)
The anterior cruciate ligament (ACL) appeared thickened with intermediate signal intensity, indicative of a mild-to-moderate sprain, without a definitive tear. The posterior cruciate ligament (PCL), medial and lateral collateral ligaments, and menisci appeared intact. Notably, there was evidence of trochlear dysplasia. Additionally, there was mild displacement of the pes anserinus tendinous insertion without gross tendon tear or bursitis. The patellofemoral joint was grossly intact, with no significant joint effusion.
The treatment plan focused on rehabilitation, emphasizing strengthening the quadriceps femoris and hamstring muscles to address the patient’s symptoms and improve knee function. The patient needs to diligently follow this regimen and return for a follow-up in six months to evaluate progress and adjust the treatment plan if necessary. If symptoms do not improve, surgical excision of the osteochondroma will considered.
Discussion
Snapping knee syndrome is relatively uncommon, characterized by symptoms that predominantly manifest on the lateral aspect of the knee, whereas occurrences on the medial side are rare.13,14 Symptomatic snapping knee syndrome can result from various extra-articular and intra-articular structures, such as the biceps femoris tendon, discoid meniscus, popliteus, and semitendinosus tendons, iliotibial band, and intra-articular tumors.15 Among these, snapping caused by osteochondroma is exceptionally rare.12 Although osteochondromas are benign bone tumors commonly observed, they typically do not cause symptoms unless there is trauma or compression of nearby tissues.7–11
In our case, the patient presented with knee pain attributed to patellofemoral pain syndrome (PFPS) based on her history and physical examination. The diagnosis aligns with the characteristic presentation of PFPS, a condition marked by discomfort localized behind or around the patella, which typically intensifies during activities that place a load on the patella when the knee is bent.16,17 PFPS is frequently associated with risk factors such as female sex and engagement in physical activities that impose repetitive mechanical stress on the knee joint, including jogging, crouching, and stair climbing.16,18–20 She also had medial snapping caused by a proximal tibial osteochondroma, confirmed through imaging, which precipitated following the trauma. The management involved a structured physiotherapy program aimed at muscle strengthening to address both the PFPS and the snapping, with careful monitoring to guide further therapeutic decisions.
Imaging is essential for diagnosing snapping knee syndrome and identifying other potential causes as part of the differential diagnosis. While clinical history and physical examination are fundamental, advanced imaging modalities, such as MRI, are invaluable in confirming the presence of conditions like osteochondroma, as demonstrated in our case. These imaging tools not only aid in pinpointing the underlying cause but also assist in ruling out other potential sources of knee pain, thereby ensuring accurate diagnosis, facilitating targeted treatment, and guiding the prognosis.
Conclusion
Medial hamstring snapping knee syndrome due to osteochondroma is a rare cause of post-traumatic knee pain and snapping. Thorough clinical assessment and imaging are critical for an accurate diagnosis. While conservative management is the first-line approach, surgical excision may be necessary if symptoms persist or the osteochondroma increases in size. Timely intervention can lead to improved patient outcomes.
Contributions
Khawla Almutairi and Reem Almutairi contributed equally to all aspects of the case report, including the introduction, case report, and discussion. Both are co-first authors and share equal responsibility for the study. Ismail Almogbil supervised the project and provided general guidance during the manuscript preparation. All authors have reviewed and approved the final version of the manuscript.
Acknowledgments
No assistance with the article
Funding
No financial support and sponsorship
Conflicts of interest
No conflicts of interest