

Introduction
In a 1992 Internal Medicine Grand Rounds presentation that focused on medical education, Dr. Frank Griffin, Jr. made the comment that “understanding is the key to learning”.1 His contention was that for information to be effectively retrieved, it must first be efficiently stored. The storage of information is contingent on understanding the material. Commenting about classic medical school education, Griffin said that the focus is usually on acquiring a “morass of details,” which precludes the commitment of time to consider concepts. Memorizing mounds of facts without having an effective conceptual framework to store them is often an unsuccessful learning style because memory frequently fails without understanding.
What can be deduced from the Griffin comments is that learning can occur in many different ways, with variable degrees of effectiveness. It was noted by Torre et al that a crucial distinction should be made between meaningful versus rote learning.2 All too often, medical education presents volumes of information with no instruction on how to meaningfully learn. Such rote learning becomes an obstacle to truly understanding the information.
To facilitate learning that is meaningful, a conceptual approach is deserving of consideration. When information is first approached conceptually, there is mechanism for both organizing and distinguishing the information. We propose that concept maps are a framework to accomplish this goal.
Of the many strategies for metacognition (that is, thinking about thinking), concept mapping is proven to improve meaningful and independent learning.3 First developed by Joseph Novak at Cornell University in the 1970s, concept maps are graphical representations of a given concept and provide an opportunity to better understand a topic. The sequential levels of a concept map, referred to as levels of hierarchy, allow the learner to go from broader to more refined layers of knowledge. An additional feature of concept maps that facilitates understanding is the ability to create cross-links between various items on a map. In doing so, insights can be drawn from seemingly disparate bits of information. Concept maps are useful for readers of all levels – from medical students needing a guide to learn the material, to residents using a guide to help organize previously learned information, to clinicians refining their ability to communicate complex information to students and patients.
The numbers and types of orthopaedic infections can be daunting. Without a conceptual approach to them, an insightful degree of understanding them is difficult. In this paper, we propose using concept maps as an organizational approach to these infections and have created a map that we believe provides such a perspective. This paper is not meant to serve as an approach on how to treat, but rather as a storage system with the ability to assist in understanding orthopaedic infections. To our knowledge, this information has never been presented in this way. We are not proposing that this is the only way to think about orthopaedic infections but present it as an example that is easily understandable to the reader.
The Core Considerations
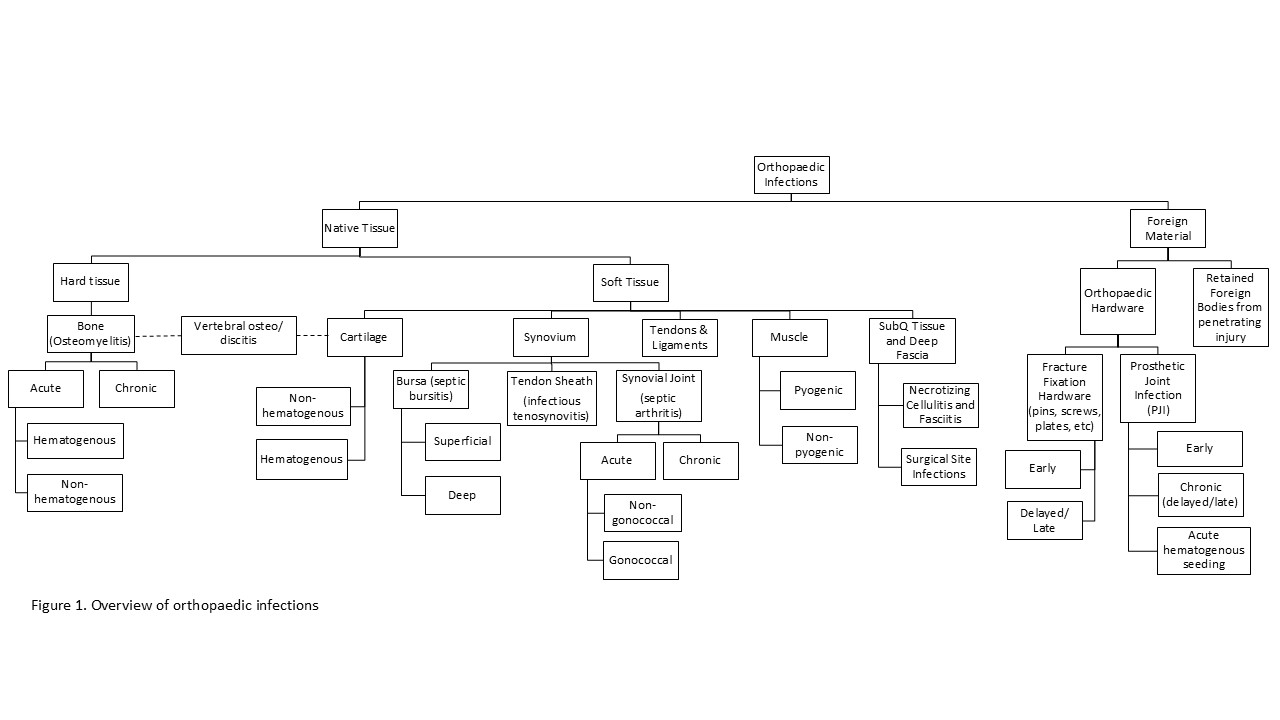
Our proposed framework is based on what is infected and how it becomes infected. The first level of hierarchy on our map is a consideration of the type of substance that is infected: native tissue infections versus foreign material, i.e., implants. Foreign material infections are inherently different from native tissue infections in that rather than biologically active tissue being infected, it is an inert surface with no direct blood supply for delivery of antibiotics and immune cells. Additionally, the organism(s) causing the infection are most often introduced when the foreign object is introduced into the body, though not always, as we will discuss later. Within native tissue infections, we further sub-classify infections, based on previously published divisions, as hard tissue and soft tissue.4–6 An overview of orthopaedic infections concept map can be seen in Figure 1.

1. Hard Tissue
Hard tissue infections are infections of the bone, osteomyelitis. Osteomyelitis can be classified in a variety of ways, but for simplicity in forming a mental framework, we prefer to first divide it into acute and chronic, as seen in Figure 2. Osteomyelitis is best considered chronic when the infection has lasted greater than 6 weeks or when there is radiological evidence of sequestrum formation.5,7,8

Although we propose a classification system for forming a mental framework, clinically, osteomyelitis is classified using the Cierny-Mader Classification system, in which both the physiological condition of the host and the bone lesion is classified. Within this system, there are four types of bone lesions based off anatomical position: Type I—medullary; Type II—superficial; Type III—localized; Type IV—diffuse.9 Each of which can either be acute or chronic. We will discuss each of these in relation to our proposed conceptualization system.
1.1. Acute Osteomyelitis
Acute osteomyelitis is best conceptualized by mode of infection, with the two main categories being hematogenous and exogenous (non-hematogenous) spread.
Hematogenous spread results from bacteria from a distant site in the body entering the bloodstream (bacteremia) and later seeding medullary bone, Type I.9 The most common organisms being S. aureus and P. aeruginosa.6,10 Hematogenous osteomyelitis occurs in children with the metaphysis of long bones being the most susceptible regions due to their vascular anatomy.4–6,8 In childhood, growth cartilage in avascular. The growth plate is instead supplied by blood dumped into venous sinusoids just beneath the growth plate. Small arterioles heading to the growth plate bend away and dump into these sinusoids. This acute bend along with the increase in vessel size from arterioles to sinusoids leads to an area of slower blood flow and pooling allowing bacteria to easily accumulate and lead to infection.5,6,8 Low amounts of phagocytic cells in these vascular loops also lend to the development of infection and abscesses.5,8 In adults, these sinusoids are eliminated as the resorption of growth cartilage leads to vascular connections forming between the metaphyseal and epiphyseal vessels.4,6 As such, hematogenous osteomyelitis is rare in healthy adults and is more seen in immunocompromised patients (greater risk of infection overall), sickle cell disease (bone infarcts and marrow thrombosis), intravenous drug users, hemodialysis patients (repeated vascular access) and vertebral osteomyelitis.4,5
Non-hematogenous or exogenous osteomyelitis is different from hematogenous in that rather than the infection arriving by blood and starting in the medullary of the bone, it most often results from penetration of the skin and the periosteum being disturbed in some way thus introducing bacteria and infection to the bone.5,6 Due to this, exogenous osteomyelitis is often polymicrobial compared to a single organism that is often seen is hematogenous osteomyelitis.8 Recall that the periosteum serves as a protective outer barrier for bone; this layer can become interrupted through trauma or surgery allowing for direct contamination or through erosion from nearby abscesses leading to contiguous spread.
Bacteria alone, on the basis of direct contamination are often insufficient to produce osteomyelitis, and instead often requires a disruption of adequate blood flow to the bone.5,10 Trauma and surgery, in addition to introducing microorganisms into the bone, can disrupt blood flow to bone. This results in a proper immune response not being able to reach the bacteria and can also create areas of necrotic bone, serving as a nidus for proliferation.5,8,10 Like a foreign body, areas of necrotic bone are inert avascular sites where biofilms can form, making it extremely hard to treat and eradicate.10
Trauma and surgery can lead to Type III and IV osteomyelitis. Type III, localized osteomyelitis, involves both the medullary and cortex, and is in a single location within stable bone. In addition to trauma and surgery, instances where medullary or superficial osteomyelitis extend to involve both can cause Type III lesions. Type IV, diffuse osteomyelitis, also involves both the medullary and cortex, but as the name suggests is diffuse leading to bone or axial instability, either before or after required extensive debridement and resection. The most common examples of Type IV are infected non-unions and through-and-through metaphyseal/ epiphyseal lesions.9
Exogenous osteomyelitis from contiguous spread is due to pressure ulcers or soft tissue infections like an abscess eroding away the periosteum and infecting the underlying bone.5 This mostly differs from direct contamination in that it the infection starts superficial, Type II, and can progresses to Type III or IV.
Osteomyelitis due to contiguous spread is most often seen in patients with neuropathy and/ or peripheral vascular disease, particularly diabetics who often have both. Patients with neuropathy have decreased sensation, frequently leading to pressure ulcers over bony prominences. Pressure ulcers occur at bony prominences due to these being weightbearing areas. Blood flow in these regions is diminished and/or cut off due to the pressure being applied onto arteries and/or capillaries at the bony prominences. The decreased blood flow leads to skin and tissue breakdown forming ulcers that can become infected.11 Similarly, patients with peripheral vascular disease have poor blood flow leading to poor wound healing from minor traumas, i.e., diabetic foot infections. Due to inadequate blood flow in each of these scenarios, antibiotics and a proper immune response are unable to reach the associated infections. If left untreated, these chronic infections can progress, erode the periosteum, and extend to the bone.4,6
1.2. Chronic Osteomyelitis
Osteomyelitis is best considered chronic when the infection has lasted greater than 6 weeks or when there is radiological evidence of sequestrum formation, but there are several factors that differentiate chronic osteomyelitis from acute.7 All these factors have one thing in common, the body is unable to elicit a proper immune response to fight off the infection.
A sequestrum is avascular necrotic bone and is a radiologic indicator of chronic osteomyelitis.7 As a bone abscess spreads, it cuts off blood supply to portions of bone by stripping the blood supply from the overlying periosteum as well as through thrombosis of endosteal vessels, leading to osteonecrosis and the formation of a sequestrum.5,8 With no blood supply to the sequestrum, a proper immune response and antibiotics are unable to reach the bacteria sequestered within it, allowing for the infection to persist. The body attempts to wall off the infection by producing reactive immunocompetent bone around the abscess and sequestrum called an involucrum.5,6,8 If the body is unsuccessful at walling off the infection, the abscess will continue to spread and destroy the surrounding cortex.6
Osteomyelitis associated with vascular insufficiency such as in diabetics, as discussed earlier in relation to contiguous spread, is considered chronic and is one of the most common causes of chronic osteomyelitis. Similarly, osteomyelitis associated with foreign bodies, such as surgical implants or penetrating injuries, is another form of chronic osteomyelitis.7
Infections due to certain slow-growing organisms that often cause a granulomatous reaction are also considered chronic osteomyelitis in contrast to pyogenic organisms that cause an acute, rapidly progressive course. Examples of these insidious organisms that cause chronic osteomyelitis include acid-fast bacilli such as M. tuberculosis and various fungal species such as Blastomyces dermatitidis, Coccidioides sp., Histoplasma capsulatum, Sporothrix schenckii, Candida species, Cryptococcus, and Aspergillus.7,8,10
In addition to 6 weeks being deemed a temporal mark for chronic osteomyelitis, relapse, or persistence of infection after being treated is considered a chronic form.7
2. Soft Tissue
Soft tissue infections are infections of the cartilage, synovium, tendons, ligaments, muscles, subcutaneous tissue, or deep fascia.
2.1. Synovium
Synovium membranes produce synovial fluid that allows for movement between adjacent tissues. Synovium lines bursae, tendon sheaths, and diarthrodial joints.12 The synovium is highly vascular and lacks a basement membrane, making it susceptible to hematogenous seeding.13 The high vascularity also makes it resistant to infection due to it being readily accessible by host immune cells. Hematogenous spread is usually seen in relation to septic arthritis, while direct contamination is most common in bursa and tendon sheaths. Once bacteria or microorganisms are introduced to the synovial fluid, they readily multiply as synovial fluid serves a good medium for growth.5 Figure 3 provides a concept map for synovial infections.

2.2. Bursa (Septic Bursitis)
Bursitis is the inflammation of bursa leading to excess fluid production causing swelling and pain. It can be caused by overuse, prolonged pressure, or arthritis. When caused by infection, it is considered septic or infectious bursitis.
Septic bursitis can occur in superficial or deep bursa. Common routes of infection include direct contamination, contiguous spread, or hematogenous seeding. The most common inciting organism is Staphylococcus aureus followed by Streptococcus species. Common sites of infection include prepatellar, olecranon, and trochanteric.14
Septic bursitis most commonly occurs in superficial bursae due to direct contamination from micro-trauma or direct puncture to the overlying skin.14,15 The superficial location and sparse overlying connective tissue make superficial bursae easily accessible to inoculation from microtrauma.15 Contiguous spread from overlying skin infections and soft tissue infections such as cellulitis is also a common cause of superficial septic bursitis.14
Deep septic bursitis can also be caused by contiguous spread from nearby infections but is more commonly caused by spread from septic arthritis and hematogenous seeding.14
2.3. Tendon Sheath (Infectious Tenosynovitis)
Tenosynovitis is the inflammation of the fluid-filled synovium in tendon sheaths leading to swelling, pain, and contractures.16 When caused by infection, it is called infectious tenosynovitis.
Infectious tenosynovitis, like superficial septic bursitis, commonly occurs due to direct inoculation from micro-trauma or direct puncture to the overlying skin as well as contiguous spread from soft tissue infections.15,16 Hematogenous seeding is another possible cause. Tendon sheaths in the periphery, like the hands and feet, are most commonly affected.15
Like septic bursitis, Staphylococcus aureus and Streptococcus species are the most common inciting organisms. Other organisms of significance include Eikinella corrodens in human bites and Pasturella multocida in animal bites.16
Important: infectious/pyogenic flexor tenosynovitis is an orthopaedic emergency and occurs over a series of three surgically significant stages. Stage 1: Exudative distension of the tendon sheath; Stage 2: Purulent filling; Stage 3: Necrosis and destruction of the sheath and tendon. IV antibiotics and surgery are almost always needed.16
2.4 Synovial Joints (Septic Arthritis)
Arthritis is the inflammation of joints leading to swelling and pain. When synovial joints become infected, it is called septic arthritis.
The most common route of infection of septic arthritis is through hematogenous seeding from bacteremia. Unlike septic bursitis and tenosynovitis, septic arthritis is less likely to be caused by direct inoculation from microtrauma or puncture due to the joint being deeper than bursa and tendons, and the joint having a tough fibrous capsule that protects it.15 Major punctures such as fishing hooks, surgery, or joint injections can lead to septic arthritis. Corticosteroid injections have the combined effect of causing immunosuppression and introducing bacteria into the joint. Contiguous spread from adjacent osteomyelitis or other soft tissue infections may also occur.6,17,18 This most commonly occurs in children from nearby osteomyelitis due to the configuration of the joint capsule being beyond the epiphyseal growth plate in some bones, allowing bacteria to enter the joint space from infections in the metaphysis.6,18
Since hematogenous spread is the most common cause of septic arthritis, it is easy to understand how monoarticular or polyarticular infections can occur. The most common organisms involved are usually ones that cause bacteremia such as Staphylococcus aureus, Streptococcus species, and Neisseria gonorrheae.17,18
Host factors also have a significant impact on susceptibility to infection. Preexisting arthritis and joint damage increase susceptibility due to the damaged tissue being less able to illicit an antiphagocytic reaction towards bacteria.18,19
Septic arthritis is devastating due to the inflammatory response and resulting joint damage. Once infection occurs, chemotactic factor is released by cells, promoting neutrophil migration into the synovium. The acute inflammatory response results in increased synovial fluid, causing increased intraarticular pressure, ischemia, and release of chondrolytic enzymes from the lysosomes of neutrophils, mediating cartilage damage.17,18 Therefore, surgical drainage and arthrocentesis are important—not only to help clear the infection, but also to relieve the pressure that leads to ischemia and cartilage death. In addition to host response mediated damage, bacterial toxins and enzymes like bacterial matrix metalloproteases and microbial surface components can lead to joint destruction. Staphylococcal adhesins promote the binding of the bacteria to intra-articular proteins allowing bacteria to adhere and eat away at the cartilage.17 These adhesin proteins are partly what make Staphylococcus aureus so virulent.20
Septic arthritis is classified as either acute or chronic, with acute arthritis being much more common.
2.5.1. Acute Septic Arthritis
Acute septic arthritis is usually divided into non-gonococcal and gonococcal based on clinical features. The clinical thought process influencing this approach is based on a clinically relevant treatment consideration. Patients with non-gonococcal septic arthritis, for which S. aureus is the most likely pathogen, usually require evacuation of purulent material from the joint space to prevent acute joint destruction that occurs due to a brisk inflammatory reaction. In contrast, gonococcal septic arthritis does not usually result in joint destruction and, therefore, does not mandate drainage for either cure or joint preservation.
Non-gonococcal is the cause of 80% of septic arthritis with Staphylococcus aureus being the most common cause followed by Streptococcus species. These infections are often associated with drug abuse, cellulitis, abscesses, endocarditis, and chronic osteomyelitis.21 Other less common organisms include gram-negative bacilli like Pseudomonas aeruginosa and Escherichia coli which are common in intravenous drug users and invasive urinary tract infections, respectively. Non-gonococcal septic arthritis usually involves a single joint (unless chronic degenerative disease exists leading to multiple joints getting infected) and is very destructive, usually requiring drainage of the joint.20,21
Gonococcal septic arthritis is common in sexually-active adolescents and can be mono- or polyarticular. When associated with disseminated disease, it can present with migratory arthralgias, tenosynovitis, and dermatitis. The main difference surgically compared to non-gonococcal septic arthritis is that gonococcal septic arthritis is commonly non-erosive and does not always require drainage.20 The less erosive nature is not fully understood but can be due to the lack of staphylococcal adhesins that allow Staphylococcus aureus to directly adhere to cartilage. Another proposed idea is due to the gonococcal surface protein Porin that diminishes the inflammatory response by down regulating complement proteins.22
2.5.2. Chronic Septic Arthritis
Chronic septic arthritis is rare and usually caused by more insidious organisms like mycobacteria, fungi, and saprophytic bacteria that produce a more indolent infection.18,21 These produce low-grade synovitis. The chronic granulomatous reaction that occurs can eventually lead to substantial tissue destruction late in the disease course.21
2.6. Tendons and Ligaments
Although infectious tenosynovitis (tendon sheath infection) is well studied and reviewed in the literature, infection of tendons without a sheath is rarely discussed. Similarly, articles discussing infection of ligaments are scarce as well. When reviewed, infections of tendons and ligaments are typically in the context of infected grafts postop— a form of direct contamination.23,24 Other causes include contiguous spread from nearby soft tissue infections.25 Examples of isolated infections of ligaments or tendons or hematogenous spread directly to these tissues were not found in our literature search.
2.7. Muscle (Infectious Myositis)
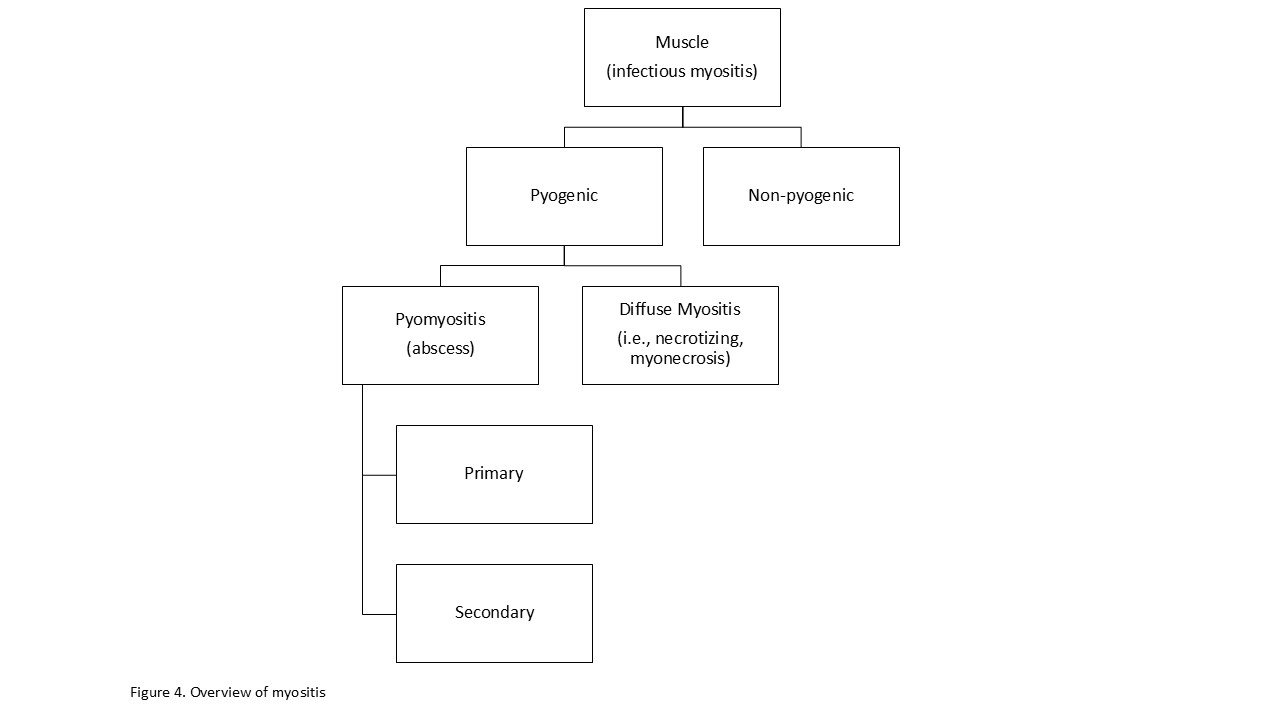
Infection of skeletal muscles, infectious myositis, is uncommon due to the high vasculature nature of healthy muscle making it resistant to infection.6 A wide range of organisms can cause it though, including bacteria, fungi, viruses, and parasites, all of which present differently based on the causative agent. Because of the extensive variety of presentations and inciting organisms, it is best to first differentiate infectious myositis based on pyogenic and non-pyogenic infections.26 Pyogenic infections can be subdivided into pyomyositis and diffuse myositis. This is displayed on our concept map in Figure 4.

2.7.1. Pyomyositis (abscess)
Pyomyositis is an acute bacterial infection of skeletal muscle leading to pus and abscess formation. The most common organism involved is Staphylococcus aureus. Other organisms include Streptococcus species, Clostridium species, and fungi.26 Pyomyositis can be classified as either primary or secondary and is often caused by direct contamination from trauma or contiguous spread. It is rarely caused by bacteremia and hematogenous seeding as it requires concurrent muscular damage.26,27
Pyomyositis due to bacteremia is considered primary pyomyositis. Hematogenous seeding can occur in blunt trauma causing a hematoma within muscle, or occlusion of blood vessels leading to muscle necrosis and formation of an avascular bed ideal for bacteria proliferation.6,27 Muscular damage is required for infection to occur as healthy skeletal muscle is resistant to infection.6,26,27
Secondary pyomyositis is caused by contiguous spread or penetrating trauma. The most common cause of contiguous spread is adjacent osteomyelitis.26
2.7.2. Diffuse Pyogenic Myositis
Unlike pyomyositis that causes a contained abscess, other pyogenic infections of muscle cause a more diffuse infection with muscle necrosis that present as medical emergencies. Common examples of these are Streptocococcus pyogenes (Group A Streptococcus) necrotizing myositis, gas gangrene (clostridial myonecrosis), and non-clostridial (crepitant) myositis. Depending on the offending agent, the route of infection can be due to hematological seeding or direct contamination from trauma.26 Of importance, these often can lead to acute compartment syndrome, an orthopaedic emergency requiring a fasciotomy.
2.7.3. Non-pyogenic Myositis
Viruses, parasitic agents, and other rarer bacteria can cause non-pyogenic skeletal muscle infection and inflammation. Common examples include influenza, Trichinella spiralis (trichinosis), Taenia solium (cysticercosis), and Borrelia burgdorferi (Lyme disease).
3. Foreign Material
With infections, foreign material is different than living native tissue as it is inert and does not elicit an antiphagocytic reaction towards bacteria, allowing for bacteria to readily adhere to it and multiply.16 With no blood supply of its own, host immune cells and antibiotics cannot adequately reach the bacteria to fight them, allowing for infection to take place and persist. Infections of foreign material are further complicated by biofilm formation.
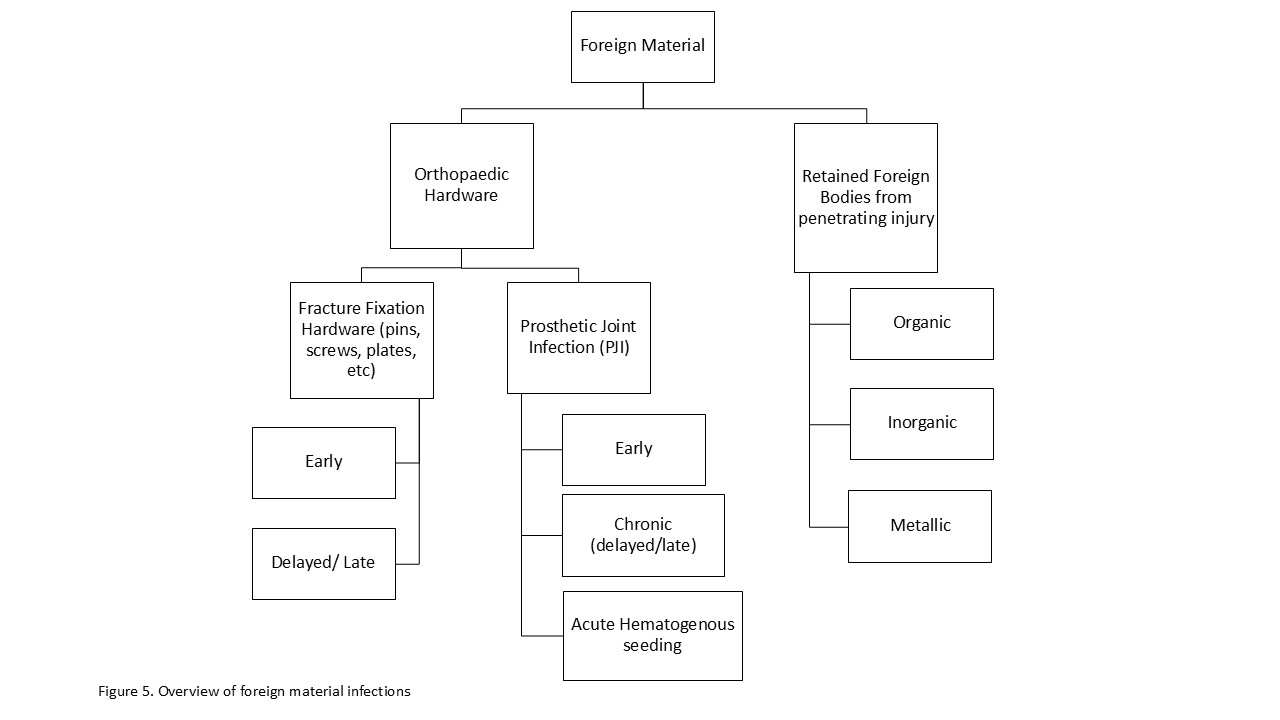
A biofilm is a colony of bacteria adhered to an inert surface surrounded by an extracellular matrix of polysaccharides/glycocalyx. The formation of a biofilm starts with adhesion of bacteria to an inert surface, such as necrotic bone, foreign body, or prosthetic implant. Adhesion occurs due to a combination of attractive forces and polysaccharides on the bacterial surface. Following adhesion, the bacteria proliferate and produce a mucopolysaccharide extracellular matrix. Once the biofilm is formed, it is hard to eradicate the infection due to the biofilm serving as a protective barrier for the bacteria from penetration by host immune cells and antibiotics, leading to chronic infection.8,10 Infected foreign material must be surgically removed to eradicate the infection. Foreign material can be classified as retained foreign bodies from trauma or orthopaedic hardware. Figure 5 displays our concept map of foreign material infections.

3.1. Retained foreign bodies from trauma
Retained foreign bodies (RFBs) from trauma most commonly occur due to penetrating, lacerating, and crush injuries. RFBs can lead to an array of infections depending on the location of the RFB including osteomyelitis, septic arthritis, tenosynovitis, and various other soft tissue infections, even necrotizing fasciitis.28
RFBs can be classified as organic (wood splinters), inorganic (rubber, glass), and metallic.29 Organic material provides a favorable environment for bacteria to reproduce, so it should always be removed. Inorganic and metallic RFBs can remain without causing infection but should be removed if the object is likely contaminated. If the inorganic/ metallic RFB does become infected, it must be surgically removed.29
3.2. Orthopaedic Hardware
Orthopaedic hardware infections can be divided into prosthetic joint infections and fracture fixation hardware like pins, screws, nails, and plates. Regardless of the hardware infected, the pathophysiology of each involves the formation of biofilms by the infecting bacteria.
3.2.1. Fracture Fixation Hardware
Infections associated with fracture fixation hardware can be divided into early infections and late/delayed. Early infection (< 2 weeks) is acquired during the inciting trauma or implant surgery and is caused by virulent organisms like Staphylococcus aureus. Delayed (2-10 weeks) and Late (>10 weeks) infections are also usually acquired during the trauma or surgery but are mainly due to low virulence organisms like coagulase-negative staphylococci (e.g., S. epidermidis, S. hominis, S. haemolyticus). Delayed infections caused by virulent organisms are usually due to insufficient antibiotics during surgery leading to a delayed onset. Late infections may also be caused by virulent organisms from a low inoculum that cause a more insidious onset. In addition to direct contamination from trauma or surgery, hardware can become infected from contiguous spread from adjacent soft-tissue or surgical site infections. Hematogenous spread of infection is also a cause of late infections in fracture fixation hardware but is much less common compared to prosthetic joint infections.30
3.2.2. Prosthetic Joint Infections
Prosthetic joint infections (PJIs) are a major concern of joint replacement surgery. There are many classification systems of PJIs using time since surgery and route of infection. Using a modified Tsukayama’s classification, PJIs can be conceptualized by dividing them into early postoperative, chronic (delayed/late), and acute hematogenous seeding.31
Early postoperative infections occur during the first three months since surgery and are due to bacteria implantation during surgery.31–33 This can be from direct contact or aerosolized contamination of the prosthesis or periprosthetic tissue.33 They typically present as an acutely swollen joint, similar to septic arthritis, with the bone-prosthesis interface remaining unaffected. This offers a favorable prognosis, as early identification can allow for the possibility of preserving the prosthesis.32
Chronic PJIs can be subdivided as delayed and late-onset, and often present with implant loosening secondary to bone loss/ osteolysis at the bone-prosthesis interface from the infecting bacteria and host immune response.31–33 Due to this, two-stage arthroplasty exchange is often needed.33
Delayed onset PJIs present from 3 to 12-24 months postop and are acquired at the time of the surgery like early PJIs. These infections are instead caused by less virulent organisms that cause a more indolent course.33 It’s debated if these start at the bone-prosthesis interface or in the joint space but can spread to both.32,33 Late-onset PJIs occur after 12-24 months postop and can occur any time during the prosthesis’s life. They are frequently due to hematogenous spread but may also be caused by extremely indolent organisms introduced at time of surgery. If due to hematogenous spread, these are proposed to start at the bone-prosthesis interface.33
Acute hematogenous seeding infections are due to hematogenous spread, but in contrast to late-onset infections, these infect the joint space.31–33 They present similar to early postoperative PJIs and septic joints, and the implant can often be retained if treated appropriately.33
Author Contributions
Study concept and design: CJB, GBL, and GHK. Analysis and interpretation of data: CJB, GBL, and GHK. Drafting of the manuscript: CJB and GBL. Critical revision of the manuscript for important intellectual content: GHK. All authors have read and agreed to the published version of the manuscript.
Competing Interests
The authors declare that they have no conflict of interest.
Ethical Statement
The authors declare that they have no ethical statement.
Financial Support
This research received no external funding.