



I. INTRODUCTION
The anterior talofibular ligament (ATFL) is one of the three lateral ankle ligaments that functions to prevent excessive inversion and plantar flexion of the foot. It’s the main ligament ensuring the stability of the ankle joint. ATFL originates from the anterior margin, above tip of the lateral malleolus about 10mm from the anterior edge, attaching to the talar body. Ankle sprains are a common injury, especially in sports, up to 50% of all injuries.
Most acute ankle sprains can successfully be treated conservatively with a short period of rest, cooling (ice), compression, and elevation to reduce the edema (the RICE principle). However, recurrent ankle sprains can lead to chronic ankle instability (CAI) in about 30-40% of cases,1 resulting in chronic pain, decreases function, especially in increasing the risk of ankle joint degeneration. The typical mechanism of ankle sprains involving excessive inversion and plantar flexion of the foot, which makes the ATFL most vunerable to be torn (up to 90%).2
Surgical treatment involves more than 60 different surgical procedures to stabilize the lateral ankle ligaments with the goal of restoring ankle stability, reducing the risk of re-sprains in the future and long-term joint degeneration. The success rate is around 80-90%. Various techniques have been developed over the years, with the modified Broström technique being considered the gold standard due to its anatomical and mechanical restoration of the ankle joint.2 In recent decades, the InternalBrace augmentation technique using SwiveLock and FiberTak anchors has been widely used combining with Broström’s method, ensuring proper tensioning, shortening immobilization time, early functional rehabilitation. Patients can return to activities and sports post-surgery in a short period of time. Additionally, about 93% of patients with chronic lateral ankle instability also have intra-articular problems, which Arthroscopy remains the gold standard for diagnosing and repairing for those injuries.3 Several studies have reported good clinical outcomes using the modified Broström technique with InternalBrace augmentation. However, this technique has not been previously implemented in Vietnam, and we are the first to introduce it at the Viet Duc University Hospital. Therefore, we conducted this study with two main objectives:
-
Describe the clinical features and image diagnosing of lateral ankle instability due to ATFL injury.
-
Evaluate the outcomes of repairing the anterior talofibular ligament using open modified Brostrom repair with InternalBrace augmentation combining with ankle arthroscopic surgery at the Viet Duc University Hospital.
II. METHODS
2.1. Methods
This was a descriptive, retrospective study, and all data were collected from clinical records. 15 patients were diagnosed and underwent surgery to repair the anterior talofibular ligament at Viet Duc University Hospital from 2019 to 2022.
The inclusion criteria were as follows:
- patients over the age of 18 with chronic lateral ankle instability;
- patients with at least 3 months of failed conservative treatments before the operation;
- Patients that diagnosed with chronic lateral instability of the ankle joint due to a torn ATFL that has been surgically repaired.
- full medical records and consent to participate in the study.
Exclusion criteria: Patients from the study that had systemic diseases, neuromuscular disorders, obesity, bony deformity of the ankle or foot on the affected side, previous surgery of the affected limb, ATFL torn on the talar side or a nonexistent ATFL.
2.2. Surgical Technique
Instrument preparation
Equipment: Arthrex machine, endoscopy system: screen, light source, a 2.7 mm arthroscope with 30° obliquity, 3.5 mm drill, 3.5 mm bonecutter shaver , small joint shaver.
Instruments: 2 SwiveLock 3.5 x 15.8 mm and 4.75x19.1 mm containing FiberTape sutures, 2 single FiberTak 2.9 mm anchors from Arthrex, 4.75 and 3.5mm drills.
Technique
The patient is placed in the supine position and a tourniquet is placed on the upper thigh, place the foot on the leg support
Patients are given spinal anesthesia.
If any intra-articular pathology has been diagnosed pre-operatively, then an ankle arthroscopy is performed before the ATFL repair.
Phase 1: Ankle joint arthroscopy
-
Identify anatomical landmarks and entry portals.
-
Inject 15-20ml of saline into the ankle joint to widen the joint space.
-
Enter the ankle joint through the anterior lateral and anterior medial portals.
Evaluate and treat intraoperative injuries
-
Remove bone spurs causing joint space narrowing.
-
Remove scar tissue, irritated synovial tissue, fibrous bands.
-
Remove loose body, drill to stimulate the damaged bone and cartilage.

Phase 2: Anterior talofibular ligament repair using the Modified Broström technique with InternalBrace augmentation
-
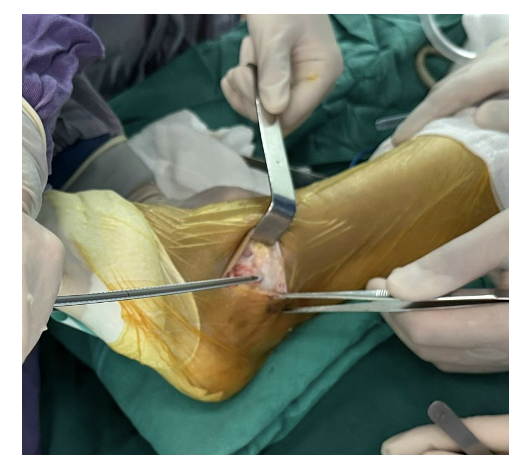
Make a curved incision along the anterior and inferior borders of the lateral malleolus about 3-5 cm.
-
The remnant of the ATFL is identified and exposed.
-
Drill and insert 2 FiberTak anchors on the anterior edge of the lateral malleolus to suture the torn ATFL remnants and the bone membrane to the attachment point on the anterior edge of the lateral malleolus.
-
Place the talus offset within the ankle joint cavity 2 cm distal to the outer aspect of the talus, pointing towards the talus body at the 7:30 position on the left foot and 4:30 position on the right foot. Drill a 3.4 mm hole in the non-articular portion of the fibular bone at a 45° angle posteriorly from the outer aspect of the foot. Taper the fibular bone hole with a 4.75 mm drill. Insert the SwiveLock 4.75 mm containing FiberTape into the fibular bone hole

-
Hold the foot in a maximum plantarflexed and inverted position, secure the FiberTak anchor sutures onto the bone membrane. This position ensures optimal tension of the repaired ligament.
-
Drill the fibular hole over 1.5 cm from the tip of the lateral malleolus, evenly distributes between the FiberTak anchors.
-
Pass both FiberTape sutures through the SwiveLock 3.5mm eyelet. With the foot in a neutral and slightly dorsiflexed position, insert the anchor into the drilled hole and mark the FiberTape at the black mark on the SwiveLock. Slide the eyelet down to the top line on the suture and secure it into the drilled hole. Before securing the anchor, place the small curved end of the pincer between the FiberTape suture and the original ATFL to prevent overtightening.

- Finally, suturing the inferior extensor retinaculum to fibula or capsule.

- Trim excess sutures, close the surgical wound layer by layer, and apply wound dressing.

Postoperative care and rehabilitation:
-
After the operation, the ankle is immobilized in a slightly everted position by use of a cast.
-
Rehabilitation exercises including isometric contraction of muscle groups around the ankle joint are started from the first day after surgery, and weight bearing are permitted after 4 weeks.
-
The cast is removed 6 weeks after surgery.
-
The patients were clinically evaluated before the operation and at follow-up by use of the American Orthopaedic Foot & Ankle Society (AOFAS) score.
-
On the basis of the postoperative AOFAS score, the outcome was rated as excellent (90 to 100), good (80 to 89), fair (70 to 79), or poor (<70).
-
Change wound dressing once every two days in two weeks.
-
Follow-up and evaluation after surgery:
Schedule patients for follow-up visits, record data in the study protocol.
SPSS 20 was used for statistical analysis.
Assess treatment outcomes using the AOFAS score, VAS score, and the anterior drawer test.
III. RESULTS
Patient characteristics
Age and gender : According to the study, the average age was 31.8 ± 4.1 years (26 - 41), with a male/female ratio of 1.5. The age group of 20-40 accounted for 93.3% of the patients.
Causes and mechanism: The main cause of lateral ankle instability due to ATFL injury was trauma, accounting for 100%, with trauma mainly caused by activities, sports, and traffic accidents at 41.6%, 60%, 6.7% respectively. The mechanism of ankle inversion accounted for 83.3%. The percentage of right ankle injuries compared to the left ankle was 60% and 40% respectively.
Time, recurrence, and treatment from injury to surgery
The average time from injury to surgery was 34.6 ± 26.8 months, ranging from 4-72 months. The number of trauma recurrences was 4.5 ± 2.3, ranging from 2 to 10 times. Proper first aid and treatment after trauma accounted for only 26.7%, with the rest not receiving proper first aid and treatment accounting for 73.3%.
Clinical and paraclinical characteristics
Frequency of clinical symptoms
All patients had pain and joint laxity. Anterior ankle pain with limited dorsiflexion accounted for 93.3% of patients with anterior impingement. The average positive anterior drawer test was 12.46 ± 2.4 mm, ranging from 10-16 mm.
Degree of joint degeneration on X-ray by Van Dijk: In the study, patients with lateral ankle instability due to ATFL injury were assessed for joint degeneration by Van Dijk, with 9/15 (60%) having no joint degeneration, 4/15 (26.7%) having mild degeneration, and 2/15 (13.3%) having moderate degeneration. Injuries on X-ray and MRI in lateral ankle instability.
On paraclinical examination including X-ray and MRI, bone spurs were found in 40% of patients, chondral injuries in 40% of patients, synovitis in 66.7% of patients, and 100% of patients had a complete anterior talofibular ligament tear on MRI.
Surgical outcomes
The average surgical time was 36.75 ± 6.75 minutes, ranging from 34-60 minutes.
Accompanying intra-articular lesions in ankle arthroscopy :
Postoperative Complications
In the study, no cases were found vasculars or nerves damaged, wound infection, or ankle joint infection.
Short-term Results
-
100% of patients had their wounds heal initially.
-
100% of patients were satisfied with the surgical results.
Long-term Results
According to our study, patients were followed up for a minimum of 14 months, a maximum of 58 months, with an average of 39.9±15.4 months.
Postoperative symptoms have significantly improved, specifically:
-
Pain symptoms were reduced to 6/15, representing 40%, including mild pain in 2 patients and moderate pain in the entire ankle in 2 patients who had preoperative joint degeneration.
-
Swelling was observed in 25% of patients compared to 80% before surgery; mild swelling on the outer side of the ankle joint appeared in the afternoon and evening but decreased after elevating the foot and resting.
-
100% of patients had ankle stability after surgery.
Assessment of Joint Laxity Post-Surgery The average anterior drawer test measurement was 3.6 mm, ranging from 2 to 6 mm.
Treatment Outcomes According to AOFAS Score and VAS Pain Score
The AOFAS score after surgery was within the good and excellent range for 100% of patients. There was a significant improvement in ankle joint function according to the AOFAS score and VAS pain score comparing before and after surgery (p<0.001).
Return to Daily Activities
93.33% of patients returned to their normal daily activities, and 80% resumed sports activities.
IV: DISCUSSION
Clinical and Paraclinical outcomes
Chronic ankle instability is common in young, active individuals, and appropriate reconstruction or repair of the ligaments ensures stabilization of the joint, improving quality of life and athletic performance. In our study, the average age was 31.8 ± 4.1 years (26-41), with the age group from 20 to 40 accounting for 93.3%, and a male/female ratio of 1.5. Ramirez4 reported a male/female ratio of 1.8 and an average age of 33.25 ± 12.73 years, while Hoang Van Dung5 reported an average age of 32 ± 12.8 years, with 87.2% being under 50 years old. 100% of the cases were due to injury, with daily activities, sports, and traffic accidents accounting for 33.3%, 60%, and 6.7% respectively. Inversion mechanism accounted for the majority with 83.33%. While 2 patients couldn’t recall the mechanism, they were involved in sports like football, which is a high-contact sport. Most patients suffered inversion injuries from daily activities like wearing high heels, running on uneven surfaces, etc.; or from sports like football, volleyball, basketball, etc. Sports-related injuries accounted for 50%, with over 50% related to basketball and 30% to football injuries.2 According to Hoang Van Dung,5 sports injuries accounted for the highest proportion at 46.2%, with inversion mechanism accounting for 79.5%.The average time from injury to surgery was 34.6 ± 26.8 months (4-72 months), with an average recurrence rate of 4.5 ± 2.3 times (2 to 10 times). Only 4 out of 15 patients received proper first aid and treatment after the injury, accounting for 26.7%. Therefore, the recurrence rate of ankle instability is high when the patients were not diagnosed and treated promptly. Preoperatively, all patients experienced pain, limited mobility in 93.3%, and swelling in 80%. Positive anterior drawer test corresponding to Grade II and above was seen in 100% of patients. According to Hoang Van Dung,5 pain was reported in 94.9% of patients, with 100% positive anterior drawer test. The degree of joint degeneration according to Van Dijk on X-rays showed 9/15 (60%) no degeneration, 4/15 (26.67%) mild degeneration, and 2/15 (13.3%) moderate degeneration. Patients with degeneration had prolonged injury time and multiple recurrences. According to Hoang Van Dung,5 degeneration rate was 38.5%, consistent with our study. Studies have shown that post-ligament injury, ankle joint degeneration may occur despite conservative treatment or even surgical intervention, with rates ranging from 13-78%. This rate increases if not treated correctly from the beginning.
Surgical technique
We performed ligament repair using the modified Broström technique, which has the advantage of anatomical repair using the remnants of the torn anterior talofibular ligament to suture without using autografts like non-anatomical reconstruction or peroneus brevis tendon graft like Hoang Van Dung.5 Additionally, this technique is reinforced by using the extensor retinaculum, ensuring the stability of the repaired anterior talofibular ligament. The addition of InternalBrace in our surgery, with the advantage of non-absorbable, non-irritating material, ensures proper tesioning and functions similar to a safety band. This allows for early range of motion of the ankle joint after surgery, protecting it from excessive inversion when the ligament is still in the early healing phase and reducing the risk of future injury. According to a study, the ultimate load of surgery with reinforcement was much higher than the initial repair of the anterior talofibular ligament (315N vs. 154 N) with no difference in stiffness and strength of the ligament between the improved Broström repair with reinforcement and intact ATFL.6 The average surgical time was 36.8 ± 6.8 minutes, ranging from 34 to 60 minutes. Similarly, Coetzee7 reported an average surgery time of 33.5 ± 8.3 minutes, ranging from 16 to 60 minutes. This combined arthroscopic and ligament repair technique is relatively new for us, and the mastery of the technique has shortened the surgery time.
Evaluation of surgical outcomes
During arthroscopy, we found (accompanying) intra-articular lesions in 14 out of 15 patients, accounting for 93.3% of cases. Therefore, ankle arthoscopy was suitable for these cases. Most patients had clinical and paraclinical signs of anterior impingement syndrome, allowing us to assess intra-articular lesions before surgery. Surgical findings in our arthroscopic evaluation included 66.7% scar tissue, synovitis causing impingement, 40% osteophytes leading to impingement, 40% chondral injury, and 100% complete tear of the anterior talofibular ligament. In chronic ankle instability, anterior joint impingement is often observed due to soft tissue or osteophytes. Similarly, Hua reported an 86% narrowing due to soft tissue and 26% narrowing due to osteophytes. Thus, anterior joint narrowing (AAI) is highly correlated with CAI. Arthroscopic surgery is a minimally invasive procedure used to address joint injuries in over 90% of chronic ankle instability cases. According to our study, patients were followed up for an average of 39.9 ± 15.4 months after surgery (14-58 months). Cho’s study8 followed up on 28 patients for more than 2 years after undergoing Broström surgery with augmentation of the ligament. Although intra-articular lesion in patients with chronic lateral ankle instability is usually diagnosed with MRI, its sensitivity and inter-observer reliability are low. Therefore, arthroscopic examination is strongly recommended because it improved patients’ residual symptoms and significantly increased patient satisfaction.
We found that all patients had good wound healing after the initial surgery. We did not record any cases of vasculars or nerves damaged, infection, or technical complications such as over-tightening of sutures, bone fractures, or loosening anchors. However, the reported complication rate for lateral ankle ligament reconstruction surgery is 5.7%. Possible complications include continued pain after surgery, infection, postoperative instability, nerve damaged (3.8%), delayed wound healing (1.6%), joint stiffness, and narrowing of the joint due to tight ligament repair.3 After surgery, clinical symptoms significantly improved. Postoperatively, 6/15 patients experienced pain, accounting for 40%, with mild pain at the surgical scar site in 2 patients and moderate pain throughout the ankle in 2 patients with signs of joint degeneration, and preoperative pain; however, the postoperative VAS pain score improved from 7 to 3, but the patients were still able to tolerate the pain without requiring pain medication. Swelling was present in 25% postoperatively compared to preoperative 80%, with decreased swelling after surgery, appearing mild to moderate on the outer side of the ankle joint after movement, walking, or standing for long periods, occurring mostly in the evening and night, reducing after elevating the leg and resting. Harington9 reported reconstruction surgery for lateral ankle ligaments in 22 cases, resulting in significant improvement in ankle joint degeneration and clinical symptoms. Functional evaluation of the ankle joint post-surgery using VAS pain scale, AOFAS score, and anterior drawer test. According to our study, there was a significant improvement in the anterior drawer test from preoperative 12.5 ± 2.4 mm (10-16 mm) to postoperative 3.6 ± 2.2 mm (2-6 mm) (P<0.001). 100% of patients felt increased joint stability after surgery. Similarly, Cho8 reported an improvement from 12.1mm (6-18mm) preoperatively to 4.2 mm (2-7 mm) postoperatively at the final follow-up (P< 0.001). In our study, the postoperative AOFAS score ranged from good to very good, with 100% achieving this level. The average postoperative AOFAS score was 91.6 ± 7.8, ranging from 70-100 points. The average postoperative VAS pain score was 0.9 ± 0.8, ranging from 0-3 points. There was a significant improvement in ankle joint function based on the AOFAS score and VAS pain score before and after surgery (p<0.001). According to Xu’s study10 comparing two groups undergoing improved Broström surgery with and without suture tape augmentation, ROM, VAS score, AOFAS score improved pre- and postoperatively, with no significant difference between the two groups at the final follow-up. However, the augmentation group allowed for early ankle range of motion, increased stability, and reduced ligament strain, resulting in a difference in the FAAM score. Ramirez-Gomez4 studied 28 patients undergoing modified Broström surgery with suture tape augmentation, with an average preoperative VAS score of 6 ± 1.18 and postoperative score of 0.53 ± 0.92. The average preoperative AOFAS score was 65.89 ± 15.08, and postoperative score was 94.60 ± 6.88; with good and very good results at 100%. According to Yang’s study on 60 patients, including 22 patients with AAI and 38 patients with pure CAI, the AOFAS score in the AAI group was significantly lower before surgery (62.9 ± 11.7 vs. 72.9 ± 11.1; p = 0.002). However, there was no difference after surgery between the two groups, with the AAI group scoring 93.4 ± 7.4 and the pure CAI group scoring 92.3 ± 9.4.
V. CONCLUSIONS
In conclusion, combining the open modified Broström procedure and InternalBrace augmentation with ankle arthroscopic surgery in patients with ATFL repaired resulted in excellent outcomes and high patient satisfaction. With a combined success rate of 100%, all cases were satisfied with the treatment outcomes.