
I. Introduction
Musculoskeletal, bone, and cartilage injuries are increasing due to demographic aging and the growing focus on exercise, underscoring the need for advanced treatment and rehabilitation strategies to enhance patient care and quality of life.1 The emergence of regenerative medicine has paved the way for successfully recreating healthy tissues.2
Regenerative medicine, a rapidly advancing field, encompasses tissue engineering as a critical component that seeks to restore damaged tissues and improve overall functionality. Recent innovations in orthopedic tissue engineering focus on regenerating bone, cartilage, and musculoskeletal tissues using engineered constructs to improve patient outcomes and quality of life.3 The trajectory of orthopedic surgery has shifted with the advent of minimally invasive surgical techniques that reduce surgical and postoperative trauma.4
Orthopedic tissue regeneration relies on four essential components: cells, signals, scaffolds, and a suitable mechanical environment. Strategies to combine these components are intensively researched to ensure clinically effective tissue regeneration.3
Grafts can be developed from various stem cell types, such as mesenchymal, embryonic, and pluripotent stem cells, each evaluated for their potential in tissue regeneration. Scaffolds, which can be derived from natural materials, synthetic substances, or devitalized extracellular matrices, offer benefits and limitations depending on their source.5
Given the highly grafted nature of bone, vascularization is crucial to ensure successful tissue integration and long-term graft viability.6 Vascular tissue engineering aims to create functional vascular networks within engineered tissues, facilitating their growth and integration into the host. Integrating vascular surgery techniques into orthopedic tissue engineering holds promise for addressing complex cases like non-union fractures and avascular necrosis.7,8
This review examines the advancements, challenges, and future directions of vascular tissue engineering in orthopedics, focusing on innovations in scaffold design, biomaterials, progenitor cell grafts, angiogenic factor delivery, and the application of vascularized grafts for bone, cartilage, and joint repair.
II. Materials and Methods
A comprehensive literature review was conducted to explore vascularized bone grafts and tissue engineering approaches in orthopedics. The search included articles published in peer-reviewed journals, accessed through PubMed, ScienceDirect, and Google Scholar. Search terms included “vascularized bone grafts,” “orthopedic tissue engineering,” “scaffold design,” “vascular tissue engineering,” “angiogenesis,” and “growth factor delivery.” Studies were selected based on relevance to bone and cartilage regeneration, with an emphasis on recent advancements in scaffold materials, cell-based therapies, and vascularization techniques.
III. The Role of Vascularization Strategies in Enhancing Bone and Cartilage Healing
Importance of vascularization
Non-union fractures remain a frequent complication in orthopedic surgery despite significant research advancements. Adequate vascularization plays a key role in ensuring successful bone regeneration by providing the callus tissue with the essential oxygen, nutrients, and growth factors.9 Similarly, the successful treatment of large segmental bone defects is also hindered by factors like infection, tumor resection, and soft tissue damage. Thus, effective healing relies heavily on restoring a large volume of bone, making vascularization strategies crucial for supporting bone regeneration and remodeling.10
Vascularized bone grafts
Vascularized bone grafts (VBGs) have proved superior to non-vascularized bone grafts (NVBGs) because VBGs contain living osteocytes and active blood flow, allowing for direct healing and better preservation of biomechanical properties and mineral content, thereby reducing bone resorption and enhancing healing potential.11 Unlike NVBGs, which rely on creeping substitution through a dead bone matrix, VBGs can effectively remodel and integrate into the recipient site even in avascular environments, preventing complications like non-unions, infections, and graft failure.12,13
Table 1 represents a detailed comparison of various vascularized bone grafts, outlining their locations, indications, vascular contributions, potential complications, and additional clinical considerations.11,14–21 Figure 1 represents an overview of scaffold-based platforms for stem cell and growth factor delivery in bone tissue engineering.

Vascular surgery techniques for limb salvage
In addition to the use of vascularized bone grafts for reconstructing non-union fractures and large bone defects, vascular surgery techniques play an equally critical role in limb salvage procedures. In cases of severe trauma or compromised blood flow, techniques such as arterial bypass and vein grafting become essential for restoring circulation and ensuring the viability of both soft tissue and bone. Lower extremity bypass surgery involves using an autogenous vein, like the ipsilateral greater saphenous vein (GSV), to bypass arterial obstructions, identified through preoperative vascular imaging, from a proximal to a distal site.22 This procedure is especially crucial for patients with chronic limb-threatening ischemia and distal occlusive disease, where autologous veins are preferred over prosthetic grafts for better long-term outcomes.23 The small saphenous vein (SSV) can also be used in patients when harvesting the GSV is difficult.24
Advancing beyond current approaches, the integration of novel scaffold designs, improved growth factor delivery systems, and cell-based techniques are driving the future of vascular tissue engineering in orthopedics.
IV. Advances in Vascular Tissue Engineering for Bone Regeneration
Although VBGs are commonly used for bone repair, drawbacks such as the limited availability of autologous bone grafts and issues like donor site morbidity, along with the potential for rejection in allogeneic grafts, can increase the risk of implant failure.25 Thus, engineered vascular tissues have emerged as a viable alternative, with an emphasis on incorporating pro-angiogenic factors like vascular endothelial growth factor (VEGF) into scaffolds to promote the blood vessel formation within the engineered constructs, facilitating osteogenesis and tissue integration.25 Additionally, scaffold designs that mimic the natural bone micro-environment can significantly improve the vascularization process and lead to faster bone regeneration.26
a. Cellular Techniques
Cellular techniques are pivotal in creating functional vascular networks for bone regeneration in orthopedic applications. Endothelial cells (ECs) initiate angiogenesis by forming the framework for vascular networks, ensuring nutrient delivery, oxygen supply, and waste removal critical for bone healing.27 Mesenchymal stem cells (MSCs) enhance vascularization by differentiating into multiple cell types and releasing pro-angiogenic factors like VEGF, supporting endothelial proliferation and maturation.28 Induced pluripotent stem cells (iPSCs) provide scalability and potential for patient-specific therapy, crucial for long-term vascular integration.29 Advances in nano-polypeptide hydrogels and 3D printing improve scaffold designs, facilitating stem cell differentiation and angiogenesis.30
The integration of cell-based approaches in orthopedic tissue engineering represents a promising avenue for developing vascularized bone constructs. Across multiple studies, the synergistic use of MSCs and ECs has emerged as a fundamental strategy to promote both angiogenesis and osteogenesis, enhancing bone healing in large defects.29,31–33
The inclusion of induced pluripotent stem cells (iPSCs) adds versatility, allowing for differentiation into multiple cell types and enabling patient-specific therapies, which are critical for achieving better integration and functional outcomes in engineered bone tissues.34,35 Replicating natural developmental processes, such as endochondral ossification, further strengthens the formation of mature bone structures, underscoring the importance of physiological pathways in engineering vascularized bone.32,36
Innovations in scaffold-free techniques, like temperature-responsive cell sheets, allow for the autonomous formation of functional tissue analogues.33 These methods not only enhance scalability but also improve vascular integration, addressing critical challenges in treating complex orthopedic defects.33 Further innovations in cell-based approaches include automated systems that streamline the production of multi-layered tissue constructs, enhancing scalability and reproducibility. These systems utilize robotic platforms to assemble cell sheets, enabling efficient production of pre-vascularized structures suitable for large, complex orthopedic defects.33,37 However, given their recent advent, studies are yet to yield decisive data pertaining to the advantages of using such systems.
b. Growth factor delivery
Effective growth factor delivery is essential for promoting angiogenesis and bone regeneration in orthopedic tissue engineering. VEGF drives blood vessel formation, while factors like basic fibroblast growth factor (bFGF), platelet-derived growth factor (PDGF), and angiopoietins stabilize and mature vascular networks, crucial for integrating engineered constructs into bone tissues.38 Strategies such as incorporating VEGF into biodegradable scaffolds provide sustained angiogenic stimulation during scaffold degradation, fostering vascular growth and bone healing.39 Combining VEGF with bFGF enhances endothelial cell proliferation and migration, accelerating early vessel formation.40,41 Nanoparticle encapsulation of VEGF and PDGF enables controlled release, stabilizing vascular networks within bone defects.42
Hydrogels, with their hydrophilic properties, deliver VEGF and angiopoietin-1 locally and efficiently, ensuring mature vascular networks for enhanced osteogenesis.43 Gene delivery techniques further enable sustained VEGF production, supporting long-term angiogenesis in large bone defects, particularly when combined with bFGF or PDGF for vascular stabilization.44,45
Electrospun fibers and microspheres integrated into scaffolds offer sequential release of VEGF, bFGF, and PDGF, promoting vascular density and maturity essential for orthopedic repair.46,47 These approaches ensure targeted angiogenesis, creating vascularized environments critical for effective bone regeneration.
Recent studies have explored various applications of factors like BMPs and PDGF in bone tissue engineering, focusing on effective delivery methods and combinatory approaches to enhance outcomes.48 For instance, PDGF-BB loaded onto tricalcium phosphate (TCP) particles is noted for promoting cell recruitment and revascularization, with applications in fractures and joint fusions.49,50 In clinical trials, it demonstrated comparable effectiveness to autografts, with over 66% fusion rates observed at 24 weeks postoperatively.49
FGF2 and BMP-2, combined with VEGF on silica-coated nanohydroxyapatite and gelatin scaffolds, were shown to stimulate vascularization and bone regeneration in calvarial defects, with varied release rates across growth factors.51 For BMP-2, polyelectrolyte film coatings on hollow poly(lactic-co-glycolic) acid (PLGA) tubes allowed tunable release, facilitating rapid bone formation in femoral defects.52 A similar focus on BMP-2 and TGF-beta1 was seen in silk fibroin-based scaffolds, which promoted mesenchymal and osteoblast proliferation, enhancing osseointegration.53
The combination of BMP-2 and FGF-2 on gelatin nanofibers stimulated osteogenic gene expression, while PDGF on poly-lactic acid (PLLA) nanofibers promoted vascularized bone regeneration in mouse calvarial defects.54–56 Finally, VEGF and BMP-2 incorporated into microspheres with chitosan hydrogels achieved sustained release, leading to bone repair and callus remodeling in rabbit mandibular defects over 12 weeks.56 Table 2 represents a summary of key growth factors utilized in bone tissue engineering, highlighting their sources, biological roles, mechanisms of action, and primary functions when integrated into scaffold-based applications.57–62
c. Scaffold-based approaches
Scaffold-based techniques are central to vascular tissue engineering, designed to replicate the extracellular matrix (ECM) and support cell growth, differentiation, and vessel formation.63 These scaffolds use a variety of biomaterials—natural, synthetic, or a combination of both—tailored to mimic the structural and functional properties of native tissues.
Natural polymers such as collagen, gelatin, and fibrin are biocompatible and degrade into non-toxic by-products, promoting endothelial cell proliferation, ECM synthesis, and osteoblast adhesion and integration.64 In contrast, synthetic options like polylactic acid (PLA), polycaprolactone (PCL), and polyglycolic acid (PGA) provide superior control over mechanical properties, degradation rates, and resistance to physiological stresses,65,66 making them ideal for load-bearing orthopedic applications. Hybrid scaffolds, combining natural and synthetic materials, enhance osteoconductivity while maintaining structural integrity, enabling vessel maturation, bone formation, and defect healing.67,68
Advanced fabrication techniques, including 3D printing and electrospinning, allow precise control over scaffold porosity, pore size, and distribution.66,67 These features are critical for nutrient diffusion, capillary network formation, and cellular infiltration, directly supporting vascular and bone regeneration.69 Furthermore, modifications to scaffold surface roughness (0.2–2 µm) and charge properties optimize osteoblast activity while preventing bacterial adhesion, reducing the risk of infection in orthopedic implants.70,71
Smart Scaffolds represent a significant innovation in orthopedic tissue engineering, enabling scaffolds to sense and respond to external and internal stimuli.72 These include exogenous triggers, such as light or mechanical forces, and endogenous factors, like inflammation or bacterial activity, which can activate localized drug delivery or adaptive scaffold deployment.72 Such dynamic systems align with the functional demands of bone repair and regeneration, making smart scaffolds highly effective for targeted therapeutic outcomes.
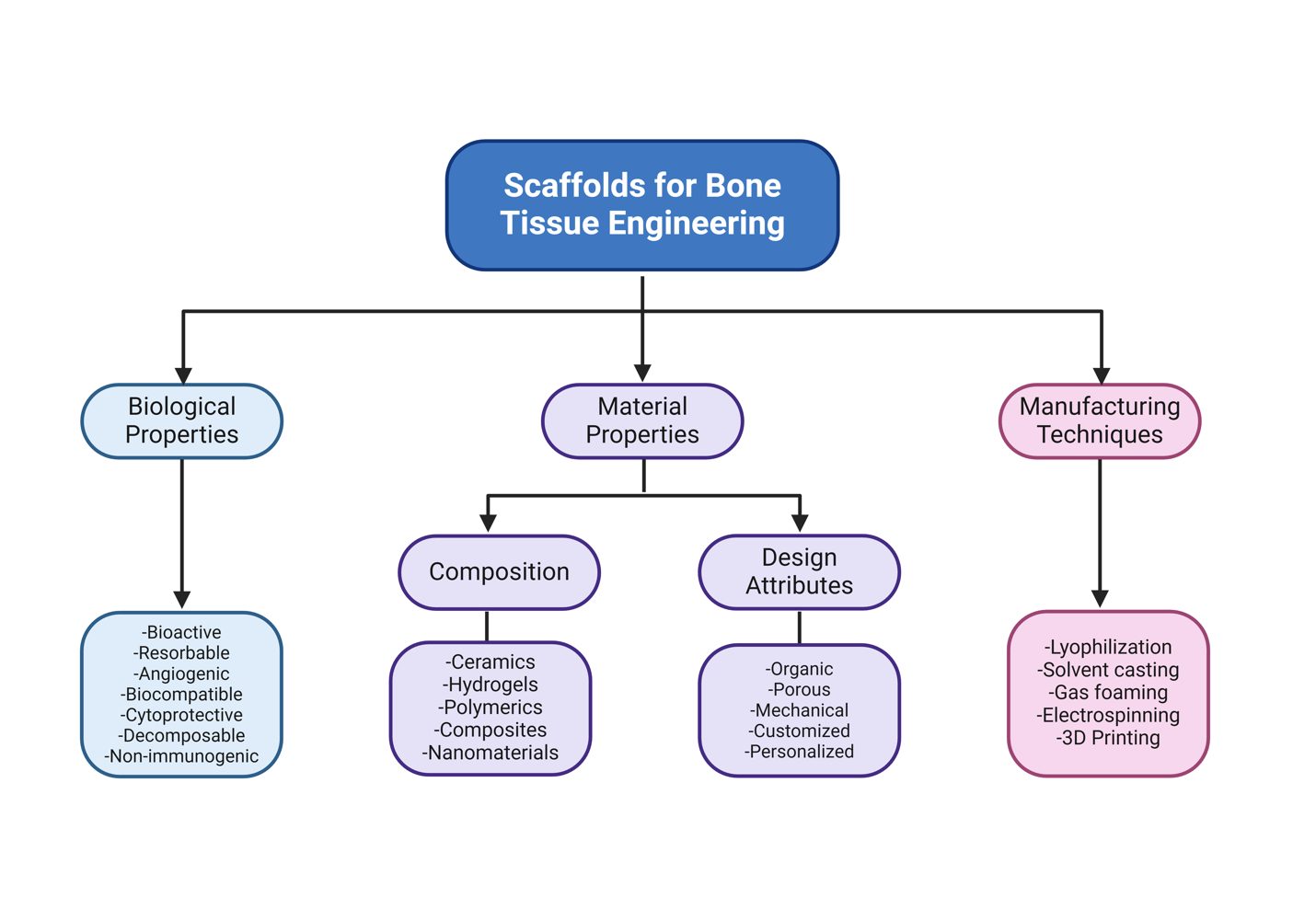
The impact of a scaffold on native cells is a key factor in material selection. Scaffolds can be osteoconductive, allowing bone growth (like calcium sulfates), or osteoinductive, actively stimulating bone formation in defects that would not heal on their own (like demineralized bone matrix).73 Recent advancements in scaffold design for orthopedics focus on enhancing vascularization, bone regeneration, and infection prevention.74 Biomaterials like modified collagen, elastin-like polymers, and bioactive ceramics improve cell adhesion, proliferation, and differentiation while 3D-printed scaffolds allow precise control of porosity, promoting nutrient exchange and capillary growth.75,76 Figure 2 highlights the key factors and technologies in scaffold design for bone regeneration.

V. Tissue Engineering Challenges in Orthopedics
Despite current advancements in vascular tissue engineering, there remain unique limitations in generating vascular tissue that retains biological functionality, particularly in orthopedics. Vascularization of load-bearing tissues such as bone and cartilage require full graft integration on multiple hierarchical levels which proves to be challenging due to graft necrosis, limited diffusion of nutrients, and lack of integration with host issue.77 Bone tissue is composed of extracellular matrix signaling factors and bone cells which function in the formation and remodeling of natural bone tissue, and any graft intended to repair and regenerate bone must contain osteoconductive, osteoinductive, and osteogenic properties.78 Vasculature repair in orthopedic tissues requires large perfusable blood vessel grafts at the injury site, then microvascular beds are needed as bone tissue faces a diffusion limit of 100–300 µm.78,79 To obtain functionality of grafted large blood vessels, specially designed biomaterials must be used to mimic the structural compositions of the different vascular layers.80 Some major limitations include recreating the distribution of cells within the three layers of vascular tissues in their natural arrangements. Moreover, reproducing a biocompatible surface that contains anti-thrombogenic properties remains a challenge.81 The gold standard for bone repair is comprised of autologous grafts which improve vascularization; however, the autograft supply is limited and can cause pain at the donor site.78 Sourcing decellularized xenogenic tissues for grafts has been used, which can avoid some complications of autologous grafts; however, severe immune responses to the graft may arise.82 Recent advances include the development of porous bioactive glass-ceramic scaffolds which enhance nutrient flow, yet the challenge of vascularization remains present.83 Another proposed alternative is using soft materials such as hydrogels for matrices as they can sustain cell viability for long periods of time; however, they face difficulty in integrating within the host tissue as their structure is easy to disrupt.57,84
Moreover, innervation has become a new focus in the development of vascularized tissue-engineered bone. Restoring sensory innervation and suppressing sympathetic nerve activation have demonstrated the ability to enhance the osteogenic properties of functional scaffolds.85
Despite the myriad advancements in the field of reconstructive surgery, one chief hurdle that remains to be overcome is the intrinsic properties of cartilage in being avascular – as well as aneural and alymphatic.86 However, recent studies have manifested the ability to vascularize tissue-engineered cartilage in animal models, which may pave the way for important clinical implications.87,88
Overall, vascularization in tissue engineering faces challenges such as incomplete vascular integration, limited diffusion of nutrients, long-term viability, difficulty in replicating native vascular architectures as well as obstacles in immune response and the mechanical stability of scaffolds.
VI. Conclusion
Orthopedic tissue engineering, especially in the realm of vascularized bone and cartilage regeneration, holds immense potential for addressing complex musculoskeletal injuries and degenerative conditions. Significant advancements in scaffold design, cell-based therapies, and growth factor delivery have demonstrated promise in promoting vascularization, essential for successful tissue integration and long-term graft viability. However, formidable challenges remain, particularly in achieving full vascular integration and replicating the hierarchical structure of native bone and cartilage. Innovations such as smart scaffolds, hybrid biomaterials, and gene delivery systems are paving the way toward more effective therapeutic options. Future research should prioritize overcoming the intrinsic limitations in scaffold vascularization and optimizing graft mechanical stability to improve clinical outcomes. The integration of vascular and orthopedic engineering techniques may ultimately establish new standards of care, enhancing patient recovery and quality of life.
Acknowledgements
The illustrations in figure 1 and figure 2 were created using BioRender (BioRender.com).
Authors’ Contributions
BS, VG, KE, and MH contributed towards the concept of the study, the literature review, data extraction, and writing the different sections of the manuscript. BS worked on Figure 1 and table 2. VG worked on table 1. MH participated in data extraction, writing the manuscript, its rigorous revision several times, and coordinated the flow of the work. MN is the corresponding author. He made substantial contributions to the concept of the study and followed up the work to ensure that it was original and complied with the research ethics and guidelines of this journal. MN also contributed to the development of the manuscript. All authors are accountable for all the contributions and integrity of the work. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Ethical review was not required because the study is a review of literature.
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.