Introduction
Peripheral nerve injuries (PNIs) are observed in approximately 2-3% of trauma patients. According to Seddon’s classification, PNIs range from neurapraxic injuries, the mildest form, typically caused by focal ischemia or compression, to axonotmesis, characterized by axonal disruption without damage to the perineurium or epineurium, and neurotmesis, the most severe category involving complete axonal disruption. Both axonotmesis and neurotmesis can result in muscle denervation and subsequent loss of muscle function.1–4
PNIs can result in significant disabilities and morbidity, impacting patients both physically and mentally. Early identification and treatment of PNIs are vital to prevent disabilities arising from irreversible nerve and target organ degeneration. Treatment modalities for PNIs include nerve autografts, nerve allografts, nerve transfers, end-to-side coaptation, and nerve conduits. Those techniques we used to day is not a new technology, that has been introduced more than 100 years ago. These options have drawbacks such as sensory loss, scarring, and neuroma formation (autografts), rejection (allografts), and donor site morbidity leading to loss of function (nerve transfers). Additionally, nerve conduits are only suitable for short nerve defects (less than 3 cm). Current advanced of the technique itself involving sutureless and tension-free repair.1 However, given the outcomes of existing treatment modalities and the slow pace of peripheral nerve regeneration, there is an urgent need for novel therapies to expedite nerve regeneration, delay target organ degeneration, and enhance target organ regeneration.4–6
Stem cell transplantation therapy, along with its derived products, represents one of the most promising advancements in regenerative medicine globally, offering new hope for PNI management. Both in vitro and in vivo studies have demonstrated the potential of these pluripotent cells to facilitate the regeneration of damaged nerves.7 This literature review will focus primarily on the role of stem cell transplantation therapies in managing PNI.
Materials and Methods
Information sources
A comprehensive literature search was conducted using PubMed, Embase, and ScienceDirect, with no language restrictions. The search was performed in May 2024.
Search strategy
A combination of free text and Medical Subject Headings (MeSH) terms was employed in the search strategy. The specific search terms used were: “((peripheral nerve injury) OR (peripheral nerve injuries)) AND ((stem cell) OR (stem cell therapy) OR (stem cell transplantation therapy) OR (stem cell exosome) OR (stem cell secretome) OR (paracrine factor)) AND (therapy).” Duplicate studies were removed, and the titles and abstracts of the remaining studies were subsequently evaluated as a preliminary screening. Afterwards, we read the full texts to exclude studies that did not cover the management of peripheral nerve injury by regenerative medicine.
Pathophysiology and Classification of Peripheral Nerve Injury
Three primary mechanisms cause PNI: cut, stretching, and compression. In the cutting mechanism, nerve injuries, whether complete or incomplete, can result from lacerations by glass, firearms, or knives. PNIs due to stretching are most commonly caused by dislocations associated with displaced fractures. In such cases, the extent of the neurological deficit depends on the degree of applied strain. Severe and continuous stretching can lead to nerve tears. Compression injuries can occur through direct or indirect mechanisms. Indirect compression involves vascular compression, while direct compression can damage the myelin sheath or the axon itself, thereby impairing nerve conduction. Prolonged exposure to compression, stretching, laceration, extreme temperatures, and chemical injuries can cause conduction blocks. If the compression becomes more severe, demyelination and focal ischemia can occur.8,9
Currently, there are two main classifications of nerve injury based on the lesions.10,11 Seddon’s classification divides nerve injury into three categories based on the presence and severity of demyelination, axonal damage, and damage to nervous connective tissue.11 The classification consists of neuropraxia (involving only myelin damage), axonotmesis (involving axonal integrity damage), and neurotmesis (involving complete nerve and connective tissue severance). On the other hand, Sunderland’s classification outlines five types of nerve injury based on the injured structures.10 Type I injuries describe protected conduction blocks. Type II injury involves axonal discontinuity accompanied by a conduction block. Type III signifies axonal and endoneurial discontinuity. Type IV involves disruption of the perineurium, endoneurium, and axons, and Type V indicates complete transection of the nerve trunk, including the epineurium.10–12
Management
Managing PNI presents challenges. A critical aspect of PNI management involves determining whether to adopt a conservative approach, await nerve regeneration, or pursue surgical intervention. Current evidence suggests earlier surgical intervention improves axonal survival post-injury and addresses potential issues such as retraction and fibrosis.2 Closed PNIs are typically managed through observation to monitor nerve regeneration, utilizing nerve conduction tests and electromyography approximately three weeks post-injury. In cases of open penetrating injuries, surgery is ideally performed within 7 to 10 days post-injury.4,13–15 Conventional direct suturing is viable when the distance from the nerve edge is less than 5 mm. Suturing larger gap may exacerbate the strain on the nerve edge, potentially worsening prognosis.14 The suture-epineurium border is the site of concentrated strain at the nerve repair site. This stress concentration may end up in suture breakdown, intraneural hemorrhage, and further scarring. In these circumstances, regenerated axons may not receive enough myelination at the distal stump, causing them to move away from areas of high-stress concentration and resulting in neuroma.3
For larger gaps, a different management approach is warranted, often involving nerve grafting. Nerve grafting is categorized into two main types: allograft and autograft. Allograft or nerve conduit is typically utilized for nerve defects smaller than 3 cm, while autografting is preferred for defects larger than 3 cm, proximal injury, and critical nerve condition. Autografting remains the gold standard for managing neglected nerve injuries. Currently, allografting has not demonstrated superior outcomes compared to autografting.14–16
Nerve Regeneration
The nervous system exhibits remarkable plasticity, with neurons capable of generating new dendrites and synapses. However, the regenerative capacity of the nervous system is very limited. While the peripheral nervous system demonstrates somewhat greater regenerative potential compared to the central nervous system, it remains constrained in its ability to regenerate following injury. Regeneration within the peripheral relies on the preservation and activity of both the cell body and Schwann cell. If these components are compromised, dendritic and axonal defects may fail to recover. The regeneration of the peripheral nervous system is possible thanks to the presence of the glia cells in the peripheral nervous system, the Schwann cells. Schwann cells play a pivotal role in peripheral nerve regeneration by transitioning to a proliferative phenotype, facilitating the formation of basal lamina, and promoting neuronal regeneration.17–20
Collateral sprouting
Collateral sprouting serves as a mechanism by which nerves preserve muscle function following injury to the innervating nerve. This process involves the extension of collateral nerve fibers to both maintain function and regenerate the injured nerve. Collateral sprouting represents the primary regeneration mechanism for axonal defects ranging from 20% to 30%. Typically, collateral sprouting initiates around four days post-injury and persists for 3 to 6 months afterward. While collateral sprouting holds the potential for optimal neuron regeneration, the process is time-consuming. Consequently, during the 3 to 6-month period of neuron regeneration, the innervated muscle may experience atrophy.10,17,21
Axon regeneration
Axon regeneration represents the predominant regeneration mechanism for nerve defects exceeding 90%. Peripheral nerve regeneration comprises three essential steps: Wallerian degeneration, axon regeneration, and end-organ reinnervation. The successful completion of each step is critical for achieving favorable regeneration outcomes. Failure at any stage can significantly impede the regeneration process, resulting in poor overall results.17,21
Wallerian degeneration, a critical process in nerve regeneration, is orchestrated by Schwann cells. These cells transform to facilitate axonal growth, expressing various proteins, including PMP-22, Krox-20, P-0, and Connexin-32, and promoting the expression of c-Jun and neurotrophic agents like NGF. This transformative process contributes to the regeneration of new Schwann cells, which play a vital role in debris phagocytosis and macrophage recruitment. Wallerian degeneration is completed following Schwann cells and macrophages’ phagocytosis of all debris. Macrophages secrete inflammatory cytokines such as IL-1 to aid Schwann cell proliferation, forming Bungner bands. These bands subsequently create a conduit that facilitates axonal regeneration.21–23
Axon regeneration commences shortly after Wallerian degeneration. The distal portion of the proximal axon initiates regeneration by forming filopodia, which extends from a growth cone at the leading edge. The mobility of this cone is influenced by key molecules such as semaphorins, ephrins, netrins, and slits. Fibrotic tissue can impede axon regeneration. The rate of regeneration in the proximal segment of the nervous system typically ranges from 2 to 3 mm/day, while in the distal segment, it averages 1 to 2 mm/day.20,21
End-organ reinnervation is equally crucial to axon regeneration in the nerve regeneration process. Successful end-organ reinnervation is essential for ensuring the efficacy of the entire regeneration process. Without successful reinnervation, the efforts of axon regeneration become futile, as the regenerated neurons cannot properly innervate the organ. Failure in end-organ reinnervation can lead to patient disability, emphasizing the critical importance of this aspect of nerve regeneration.17,20,21
Stem Cell
Stem cell sources
Stem cells have the extraordinary ability to self-renew and specialize into various cell types. Stem cells are classified into three main groups based on their differentiation potential: pluripotent, multipotent, and unipotent. Pluripotent stem cells can differentiate into all cell types of the body’s tissues. Multipotent stem cells can differentiate into various cell types within a specific lineage, including those derived from the ectoderm, mesoderm, and endoderm. Unipotent stem cells, while limited in their differentiation potential, can replicate and generate one specific cell type while maintaining self-renewal property.24,25
Embryonic stem cells (ESCs) are among the most prominent stem cell types currently known, originating from the embryo’s inner cell mass at the blastocyst stage. ESCs are highly regarded for their pluripotent nature, offering promising medical prospects. Theoretically, they can differentiate into any cell type within the human body, thus holding the potential to replace damaged tissues.26–28 However, the use of ESCs is accompanied by ethical considerations. Obtaining ESCs necessitates the isolation of the inner cell mass, which involves the dissolution of the blastocyst. This process is ethically contentious as it is perceived as the destruction of a human embryo.26,27,29
Research has increasingly focused on adult stem cells in response to ethical concerns surrounding embryonic stem cells (ESCs). Adult stem cells or mesenchymal stem cells (MSCs) are derived from mature tissues and have been successfully isolated in several forms, including bone marrow mesenchymal stem cells (BM-MSCs), adipose-derived mesenchymal stem cells (AD-MSCs), fetal tissue-derived stem cells (fetal-MSCs), skin cell precursors (SKPs), dental pulp stem cells (DPSCs), neural stem cells, and muscle-derived stem cells (SkSCs). However, adult stem cells possess a notable limitation compared to ESCs: they lack pluripotency. Adult stem cells can only differentiate into a limited range of cell types, typically multipotent or unipotent. Additionally, adult stem cells may exhibit a higher likelihood of genetic impairment than ESCs, posing further challenges to their therapeutic potential.28,30
Stem cells application in peripheral nerve injury
Peripheral nervous system regeneration heavily relies on Schwann cells. However, Schwann cell isolation and culture in vitro pose significant challenges. While some studies suggest that stem cells may not differentiate into Schwann cells to promote neuron regeneration, they release neuroprotective proteins such as NGF and BDNF. Induced pluripotent stem cells (iPSCs), BM-MSCs, and AD-MSCs are among the most commonly used stem cells in peripheral nervous system management studies. Nevertheless, research on stem cell use in this context remains primarily confined to animal models, with limited translation to human applications.2,21,26,31,32
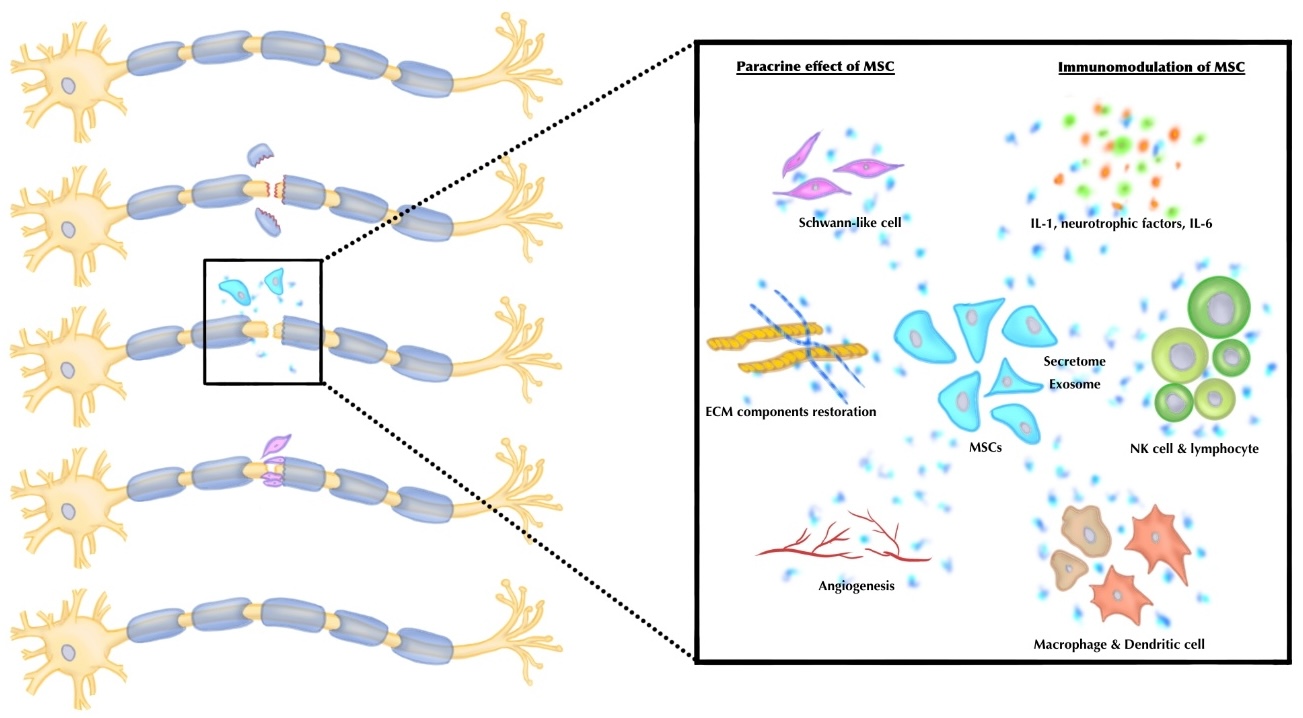
MSCs have a dual role in the regeneration of damaged tissue (Figure 1). The first role is to replace the injured tissue cells. The second role is to promote the intrinsic regenerative capacity of the injured tissue. MCSs do this by secreting growth factors and cytokines in the injured tissue. MSCs can also modulate the immune response to maximize tissue healing. In the PNI, MSCs secrete trophic factors that are important for the remodeling and regeneration of the tissue. Trophic factors improve angiogenesis and stimulate tissue regeneration. MSCs, on the other hand, also inhibit scar tissue formation, which can reduce the healing process of the nerve. MSCs are activated by lymphocytes at the site of injury. Then, it can delay the immune response to decrease autoimmunity and cytotoxicity.33–36
_application_for_nerve_regene.jpeg)
MSCs have fast proliferation, which is of great interest in tissue healing. MSCs also have paracrine and autocrine activity and trans-differentiation potential. MSCs are able to produce and secrete a lot of exosomes to give a whole range of effects. During the tissue healing process, MSCs produce neurotrophins which play a crucial role in stimulating the neuronal and glial response. Neural growth factor (NGF), brain-derived neurotrophic factor (BDNF), glial-cell-line-derived neurotrophic factor (GDNF), ciliary neurotrophic factor (CNTF), and neuregulin-1 (NRG-1) are among the neurotrophins that MSCs can make. Besides promoting local neuronal or glial cell growth and differentiation, the MSCs can specifically differentiate into glial or neuronal cells. However, the study regarding this ability is currently only focused on very limited stem cells, such as Wharton jelly stem cells (UC-MSCs), avascular amniotic mesoderm (AMSCs), and subcutaneous white adipose tissue (ADSCs). These stem cells can maintain their regeneration after injury, as stated in a few in vivo studies.33–36
The most extensively studied stem cells in previous research have been BM-MSCs. However, the challenges associated with collecting cells from bone marrow have prompted a search for alternatives. Recent studies have shown a growing preference for AD-MSCs due to their ease of collection and isolation. Additionally, AD-MSCs exhibit more rapid growth compared to BM-MSCs.27,31,37 AD-MSCs also have lower immunogenicity and can improve neural regeneration by modulating the microenvironment and inhibiting inflammatory responses.38–40 AD-MSCs have been found to promote favorable functional outcomes and axonal regeneration in PNIs, leading to higher axon density. Previous studies have demonstrated that the addition of AD-MSCs to PNI treatment protocols can enhance myelination and increase axon diameter, further highlighting the therapeutic potential of AD-MSCs in nerve regeneration.41,42
Stem cell therapy is also being explored to treat neuromuscular junction (NMJ) injuries. Currently, ESCs are frequently utilized for this purpose, but ethical concerns have increased interest in iPSCs in recent studies. In vitro studies have shown that ESC-derived motor neurons can form functional NMJs and communicate with muscles. iPSCs have provided valuable insights into the mechanisms underlying NMJ function, particularly in understanding myogenic precursors marked by CD34. Recent research has indicated that iPSCs can differentiate into motor neurons, particularly lower motor neurons (LMNs), further highlighting their potential in NMJ injury treatment.41,43 The iPSC-derived myoblasts, particularly those expressing selective CD34 markers, exhibit similarities to PAX7-derived myoblasts and muscle tissue biopsy samples in immunohistochemistry examinations. Muscle fibers and motor neurons begin to grow from the first day of co-culture, marked by the presence of neurites. Contact between neurites and myotubes typically occurs within two weeks. Staining for AChR-α is conducted to identify neuromuscular clusters in muscle fibers, which appear as large clusters. NMJ formation is typically completed within 21 days of co-culture.41,43,44
Secretome of mesenchymal stem cell
The secretome is a complex combination that includes vesicular components like microvesicles and exosomes and soluble protein components like growth factors and cytokines. These components are important in transferring genetic material and proteins to other cells. The secretome is currently known as the mediating factor of the therapeutic effect of stem cells. Current studies state that secretome could enhance endogenous repair and modulate the immune response, thus promoting better regeneration. There is a debate about whether the MSC itself proliferates and differentiates into the target cell or whether the paracrine effect of the secretome promotes better regeneration and remodeling.7,45
Using secretome as free cell therapy has major advantages over stem cell therapy. Secretome can improve cell survival post-transplantation. It also has a lower immunogenicity than a direct living cell transplantation alone because of the secretome’s lower cell surface protein content. Secretome reduces the need for a high cell count for transplantation and the possibility of phenotypic changes due to in vitro isolation and differentiation. Secretome is more cost-effective and useful for clinical applications because of its increased production rates in carefully regulated laboratory settings. The therapeutic effect of secretome is likewise customizable. We can assess the secretome for potency, safety, and dosing to improve our knowledge of this treatment. Moreover, keeping the secretome without losing its therapeutic value is possible.7,45
Exosome of mesenchymal stem cell
Exosomes are lipid-based, spherical, extracellular vesicles with a single membrane that are bilayer and operate as messengers between cells on the nanoscale. Because exosomes from a particular cell type provide sets of biomolecules exclusive to that cell, exosomes have been viewed as miniature replicas of their parent cells. Exosomes have garnered significant interest in the medical field for diagnosis and treatment. Many studies are being conducted on stem cell-derived exosomes, or SC-Exo, because of their immunomodulatory, regenerative, anti-inflammatory, and anti-microbial capabilities. SC-Exo delivery has shown much promise as a cell-free treatment for many illnesses. Exosomes released by stem cells have more benefits than their parent cells because of their tiny size, great stability, reduced immunogenicity, lack of carcinogenic potential, and simpler storage conditions. Furthermore, it has been discovered that stem cells behave in a paracrine manner via their soluble secretome, which includes exosomes. Stated differently, SC-Exo inherit anti-inflammation, immunomodulation, and tissue regeneration properties from their parental cell of origin. When combined, SC-Exo is a powerful stand-in for stem cell therapy that doesn’t have the drawbacks of its cellular counterparts.46,47
Stem cells delivery
Researchers have described a variety of stem cell delivery methods to the neural tissue, including embedding the cell in nerve conduits or scaffolds, directly delivering the cell locally through microinjection (using medium or enriched medium/secretome), or distributing the cell more widely through intravenous or intrathecal injection.48–50
MSC microinjection has a potentially good result. Local MSC injection increases axonal fiber counts, improves electromotor recovery, and enhances nerve regeneration. It also has immunological modulatory effects and enhances Schwann cells in a synergistic manner. On the other hand, it may also raise the pressure in the injured area, which might result in non-uniform cell distribution, ultrastructural damage, and subpar nerve regeneration.48–50
Intravenous (IV) MSC injection is used as an alternative to local microinjection. It could avoid iatrogenic nerve injury from needle injury and MSC leakage to the surrounding non-neural tissue. IV MSC injection focuses on the trophic function of the MSCs. However, the MSCs delivered via IV injection may not reach the nerve injury site optimally.50,51
Nerve conduits are tube-like sutures used to fill the nerve gap (after injury or neuroma removal). It can be inserted as an empty tube to encourage targeted axonal growth to the distal end of the nerve, or it may be augmented by embedding MSC and its associated products. There are two types of nerve conduits: natural and artificial. Veins, arteries, and muscles are examples of biological structures from which natural neural conduits are formed. Meanwhile, artificial conduits are made from manufactured materials such as polymers, plastics, or silicones.39,52,53
Seeding the MSC into the lumen of the conduit can be accomplished in several techniques. The first technique is to directly seed the suspension consisting of MSC and its medium into the nerve conduit’s lumen. It is easy, but lack of structural support for the transplanted MSCs.50,52–54 The second method involves injecting the cells into the nerve conduits while they are suspended in a matrix. While simplicity is lost in the process, the benefit of tailoring the extracellular environment to improve cell viability is gained. The most complex and time-consuming method is the third one, which entails growing cells and integrating them with the nerve conduit before implantation. It has the greatest potential for tissue engineering, though.36,48,52
Conclusion
PNI requires precise management to optimize outcomes. Early surgical intervention offers the advantage of improved axonal survival prognosis post-injury in complete nerve injury (axonotmesis or neurotmesis). Stem cells potentially enhance the regeneration rate after nerve injury by differentiating to nerve cells, paracrine effect, and immunomodulatory effect. Nevertheless, most stem cell research on PNI management is restricted to animal models. It is important to do more research, preferably randomized controlled trials, to see how well cell therapy, bioengineered scaffolds, and other regenerative medicine products help peripheral nerves and target organs heal in humans.
Corresponding Author
Dina Aprilya, MD
Fatmawati General Hospital
Prof. Soelarto building, 1st floor
RS Fatmawati Street, Jakarta 12430
Indonesia
Fax +6221-7660616
Tel +6289655106136
Email dina.cia.aprilya@gmail.com
Disclaimer
No patient or author details are included in the figures.
Conflict of interest
None declared
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector
Author contribution
All authors equally contributed, reviewed the results and approved the final version of the manuscript.
Ethical Approval
None. Because this paper is a literature review and not considered as human research. Thus, it does not typically require IRB review and approval.