
Introduction
Still the treatment of Perthes disease is challenging with multiple modalities and tailored according to multiple factors in each patient with no consnsus on the appropriate modality of treating child with perthes disease.1
The most important determining factors in the prognosis of the perthes disease are age, gender and the stage of the disease. But the femoral head deformity is the most crucial and determinant of outcome so the treatment of perthes depends predominantly on decreasing and or avoidance of Femoral head (FH) deformity to eliminate or decreasing degenerative hip joint disease.2
Therefore , the surgical treatment of perthes disease usually is targeting to modulate the forces exerted on the head and acetabulum, which can be done by improving the coverage of the acetabulum by pelvic osteotomy including shelf acetabuloplasty that it supports the labrum and stimulates growth of the acetabulum and therefore decreases the load on the soft head.2–4
Still, shelf osteotomy counted by some authors as salvage procedure in late stages of perthes disease.5–8 While others have endorse the use of a shelf as a labral support osteotomy to contain the extruded portion of the femoral head in the earlier stages of the perthes disease.2,9–16 Some use shelf acetabuloplasty in treating patients with hinged abduction,7–9,12,14,15 others endorse shelf augmentation contraindicated in the presence of hinge abduction.10–12,16 In our study we exclude patients with hinged abuction because of it may affect the results.
In our hospital we start using shelf acetabuloplasty in perthes disease in sporadic cases with no statistical collection of these cases but from 2017, march we start to do the technique with follow up the children and assessing the results of the shelf on the course of the head deformity resulting from perthes disease.
Material and methods
A prospective case series study was performed From March 2017 to March 2023 and was handled 20 cases (20 hips, 11 right and 9 left) with unilateral LCPD were treated with shelf osteotomy in the stage fragmentation. The 20 patients were operated from March 2017 to 2021 and follow up was up to March 2023.
Inclusion criteria include child under 12 years, perthes hip whatever the stage. Child with hinge abduction are excluded from this study .
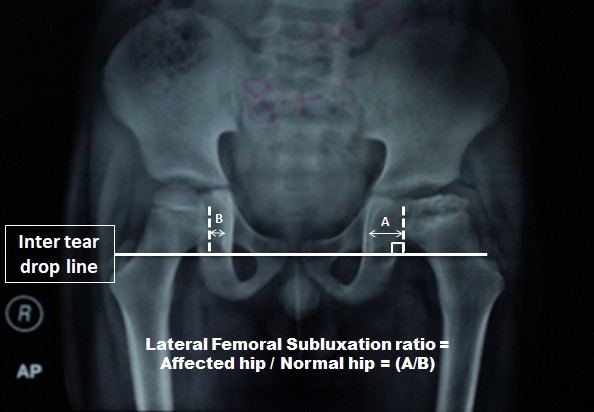
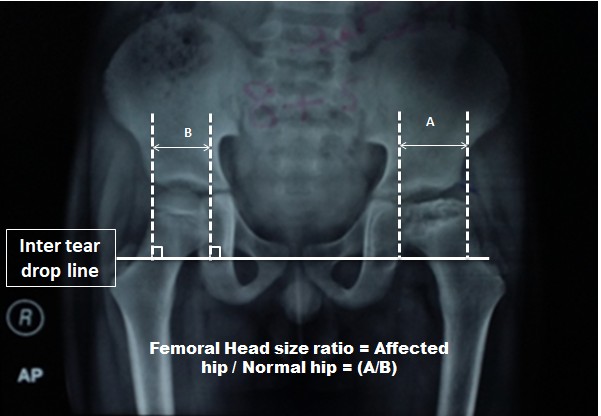
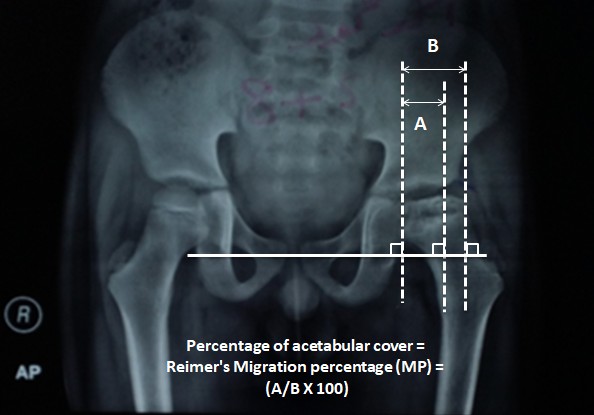
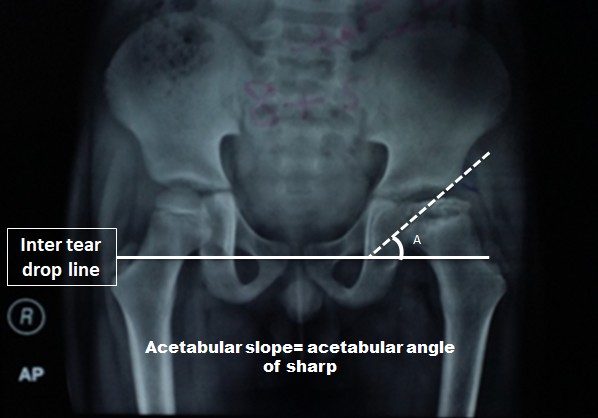
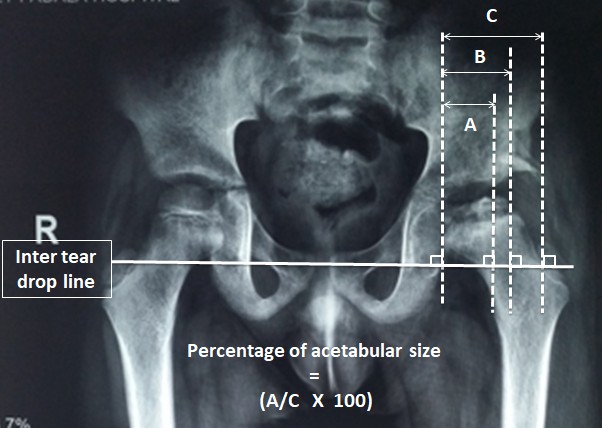
We estimated all cases clinically preoperatively and at final follow-up for pain (using VAS score ) ROM, hip disfigurement, and LLD, also radiographically measuring subluxation ratio [Figure 1], Size of femoral head (FH) [Figure 2], Reimer migration percentage (MP) represents acetabular coverage [Figure 3] and sharp’s angle [Figure 4]. Postoperatively and at the final check-up we measured the acetabular size (acetabular length relative to shelf) [Figure 5], Shelf cap ( the length of the acetabulum and shelf relative to the femoral head) [Figure 6] and sharp’s acetabular angle.


_in_patient_8_(the_percentage_of_the_cove.jpeg)



Surgical tactics
Modified bikini cut, Tensor-sartorius interval, Splitting of the apophysis of the iliac crest with a knife, elevation of gluteal muscles from ileum subperiosteal was done up to the capsule of the hip joint. Z-shaped cut of The reflected head of the rectus. Recession of the iliopsoas at pelvic border to drcrease pressure on FH. A curvilinear slot is produced in the subchondral bone of the anterolateral aspect of the acetabular roof, 3–3.5 cm in length, 2–3 mm in height, and 1–1.5 cm in depth, in an ascending direction from lateral to medial and from distal to proximal. One or two cortical grafts are harvested from the iliac wing, tightly inserted in the slot, with an extrusion of 1–1.5 cm lying on the hip capsule after its exposure and incision of the outer layer of the capule (“filleting” with a scalpel), and secured with the reflected head of the rectus femoris. This is sutured back to its origin on the direct head, keeping 5– 6 mm of the most lateral aspect of the graft, exposed in such a way as to be in contact with the cancellous and cortical graft harvested from the same iliac wing, and put on top of it . In 7 out of 20 patients an adductor tenotomy was also performed these seven patient had limited abduction of the hip. All kids were kept in hip spica for 1 month then allowed for full weight bearing after a month
Statistical analysis
Data were coded & entered using Graph Pad InStat version 3 program . Quantitative variables are presented as mean ± SD, while qualitative variables as percentages. Qualitative variables were compared among groups using the Chi-square test (χ2) test, whereas continuous variables were compared with the analysis of variance test [e.g., paired T-test]. P value < 0.05 was considered statistically significant whereas P value > 0.05 was considered statistically non- significant.
Results
Our patients’ ages were ranging 5-11 years old with average 8.6 ± 2.1years old. 12 cases were over 8 years while 8 cases under 8 years. These cases followed up 4.9 ±0.82 years old (3-6 years).
3 cases were Catterall II, 7 cases were Catterall III and 10 cases were Catterall IV, according to Herring Lateral pillar 2 cases were B while 7 cases were B/C and 11 cases were C [Table 1].
Hip pain was observed in Four patients the pain score was 4/10 in 2 cases and 6/10 in 2 cases and treated by NSAIDs and physiotherapy, the pain might be attributed by the shelf was done in a deformed head. The hip ROM is improved especially the internal rotation from 15±3.2 to 35.9 ± 4.1 degrees, the abduction range improve from 20 ±2.1 preoperative to 40 ±3.1 degrees postoperative . None of our patients has limping at the last follow up. Seven of our patients had LLD about 3.2± 0.1 mm averge .
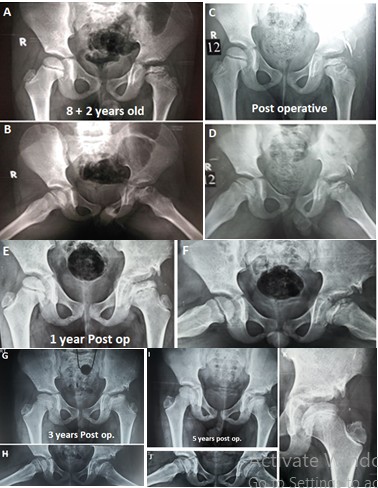
Non union of the shelf is zero in our cases [Figure 7 A-K]. Subluxation ratio of the FH decreased from 1.45±0.02 preoperative to 1.22±0.03 postoperative (at final follow up) (P<0.0001). The size of FH increased from 1.13 ± 0.1preoperative to 1.30 ± 0.04 postoperative (P=0.002) and the coverage of the shelf decreased from 145.7 ± 3.1% early postoperative to 105.5 ± 2.6 % at final follow up (P<0.0001) which attributed by the the increase of the size of the FH. There were decrease in Acetabular angle of sharp from 46.6±3.5 preoperative to 43.9±2.4 postoperative (P=0.0002). the acetabular coverage of the femoral head increased from 66.6 ±2.1 % preoperative to 74.2 ± 3.2 % postoperative (P<0.0001 which means, with time the shelf has shrunk while the acetabular growth is stimulated [Table 2].

In younger children than 8 years, the acetabulum continued to grow and so the size of the acetabulum increased from 48.8 ± 2.6 % to 69.9 ± 1.6 % while in older children than 8 years, the size of the acetabulum increased from 55.8 ± 2.8% to 69.5 ± 1.7% [table 3], so there is significant increase the acetabular coverage in relation to the shelf in younger children (P<0.02) than older ones which is attributed by the formation of coxa magna so the coverage decreases in older children.
The final outcome depending on Stulberg grading shown in Table 4 as follows, 4 cases categorized as stulberg 1, 12 cases categorized as stulberg 2, 3 patients categorized as stulberg 3 while 1 patient only as stulberg 4 and zero patient as Stulberg 5. The difference between Stulberg groups 2 and 4 was significant (P<0.001) and it was also significant between Stulberg groups 3 and 4 (P<0.001).
In younger children less than 8 yrears, the predictive value of the Catterall and Herring grades to Stulberg was significant (P<0.01) while it was non significant in older kids.
Discussion
Deformity of the FH is primarily depend up on the extrusion, so the main indication of doing surgery in this study was the extrusion of the femoral head. We did adductor tenotomy and iliopsaos recession in all patients to reduce the irritability of the hip after surgery and decrease extrusion and improve hip ROM which is also supported by many surgeons.1,5,6,10–13,15
In the study of Dimitriou et al16 12 cases of perthes aged 9-12 years after shelf showed good results with averge follow-up of 4 years. Kadhim et al17 perform as meta-analysis comparing Stulberg in children in early and late stages of perthes treated by shelf the results were good (stulberg I,II,III) in early (85% ) than late stages (69%). Near results observed in study done by carsi et al1 (84.4%). Also good results observed in 22 of 27 hips after shelf in the study of Daly et al.10 In this study the results of shelf in early stages were excellant 95% (stulberg I,II,III) than late stages 5% (stulberg 4).
In this study, the femoral head subluxation improved from 1.45 to 1.22 following shelf acetabuloplasty also the size of the femoral head improved from 1.13 to1.30 while shelf cap decreased and the coverage of the acetabulum improved.
Shelf osteotomy does not destroy the acetabular epiphysis but could stimulate growth as evidenced by increase of the acetabular coverage in our study and other studies2,7–13,15,18
The stulberg grouping done in our study is demonstrative as none of our patient reach the skeletal maturity but all were in remodeling stage.
Limitations of this study include a relatively small number of cases, no nonoperative control group, and a relatively short follow-up, which may make the statistical analysis unreliable.
Conclusion
shelf acetabuloplasty in early extruded femoral head and before extrusion improves and restores pain-free hip movements improves sphericity of the femoral head and stulberg outcome in children with perthes disease .
Ethics approval and consent to participate
Informed consent was obtained from all legal substitute decision makers of individual participants included in the study.
Consent for publication
Informed consent was obtained from all legal substitute decision makers individual participants included in the study to publicate the results.
Availability of data and material
all data and materials are available
Competing interests
The authors declare that they have no conflict of interest.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
There is no funding source.
Authors’ contributions
-
Mohammed Elmarghany, M.D (Surgeon, manuscript preparation, performed measurement, statistical analysis)
-
Tarek M. Abd El-Ghaffar M.D (review the manuscript, help in surgery)
-
Ahmed Elgeushy, M.D (manuscript preparation, performed measurement)
-
Yehia Hasanin, M.D (performed measurement)
-
Ehab Elzahed , MD (performed measurement)
-
Mohammed I Abulsoud, M.D (measurements and statistical analysis)
-
Ahmed M. Khairy, MD (collecting data, assist in surgery)
-
Mohamed N.Akl, M.D1 (collecting data, assist in surgery)
-
Mohammed Adel, M.D1 (collecting data, assist in surgery)
-
Jorge Knorr, MD2 (collecting data, assist in surgery, revise the manuscript)
Acknowledgment
we express the greatest gratitude to professor Eissa Ragheb Refai, professor Abdel-Hakim Abdallah Massoud, and professors of orthopedic surgery, Al-Azhar University Cairo, Egypt. We always can not deny their support and encouragement all over our work.