Shoulder impingement syndrome (SIS) is a prevalent and painful condition that results from the compression of soft tissues in the subacromial space, leading to functional limitations and discomfort.1 Conservative treatments are typically the first line of management; however, when these measures fail, arthroscopic surgery becomes a viable alternative. Arthroscopy enables minimally invasive diagnosis and treatment of both intra- and extra-articular shoulder pathologies through small incisions.2
Most studies report favorable outcomes of arthroscopic surgery for SIS, including reliable pain relief, functional improvement, and expedited return to activities compared to nonsurgical treatment.3 Additional arthroscopic benefits include lower complication rates and enhanced diagnostic capabilities compared to open surgery.4 However, outcomes are influenced by patient factors, impingement severity, and concomitant pathology.5,6 Given the complexity of SIS management decisions, an evidence synthesis is needed to clarify the role and expected outcomes of arthroscopic surgery. This systematic review aims to critically appraise the effectiveness, safety, and comparative efficacy of arthroscopic surgical interventions for SIS.
Study Objectives
-
To assess postoperative pain relief and functional improvement in patients undergoing arthroscopic surgery for shoulder impingement syndrome.
-
To evaluate the rates of complications and re-operation following arthroscopic surgery for shoulder impingement syndrome.
-
To compare the outcomes of arthroscopic surgery with conservative treatments such as physical therapy or corticosteroid injections for shoulder impingement syndrome.
Methods
This study adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)7 to systematically review the outcomes of arthroscopic surgery for patients with shoulder impingement syndrome. An electronic search was conducted on databases such as PubMed, Web of Science, SCOPUS, and Science Direct to identify relevant studies in English that investigate the effectiveness and safety of arthroscopic surgery for shoulder impingement syndrome. The search strategy involved using keywords related to arthroscopic surgery and shoulder impingement syndrome outcomes. Two independent reviewers screened the search results, selected eligible studies, extracted data, and evaluated the quality of the included research using appropriate assessment tools.
Eligibility Criteria
Inclusion criteria
-
Studies that evaluate the outcomes of arthroscopic surgery for patients with shoulder impingement syndrome.
-
Studies that report on the effectiveness, safety, or comparative effectiveness of arthroscopic surgery for shoulder impingement syndrome.
-
Studies that include adult patients diagnosed with shoulder impingement syndrome.
-
Studies published in the English language.
-
Studies with available full-text articles.
Exclusion criteria
-
Studies that do not specifically focus on arthroscopic surgery as an intervention for SIS.
-
Studies that only report on the surgical technique of arthroscopic surgery without outcome measures.
-
Studies that focus on pediatric patients or patients with a different shoulder pathology.
-
Studies published in languages other than English.
-
Conference abstracts, case reports, editorials, letters, and reviews that do not present original research data.
Data Extraction
To ensure accuracy and thoroughness, search results were managed using Rayyan (QCRI).8 Titles and abstracts of retrieved articles were screened for relevance based on the predefined inclusion and exclusion criteria. Studies meeting the inclusion criteria were subjected to full-text review by the research team. Discrepancies were resolved through consensus-based discussion. A standardized data extraction form was used to record key study information, including title, authors, publication year, study location, participant demographics, gender distribution, and outcomes related to arthroscopic surgery and shoulder impingement syndrome. A custom-designed assessment tool was employed to evaluate the risk of bias.
Data Synthesis Strategy
A qualitative synthesis of the research findings was performed using summary tables generated from the extracted data. Upon completion of data collection, the most appropriate approach for analyzing and presenting the data from the included studies was determined.
Risk of Bias Assessment
The methodological quality of included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tool for prevalence studies.9 This nine-item checklist assigns a score of 1 for a positive response and 0 for a negative, unclear, or inapplicable response. Quality ratings were categorized as high (score > 8), moderate (score 5-7), or low (score < 4). Two researchers independently appraised study quality with disagreements resolved through discussion.
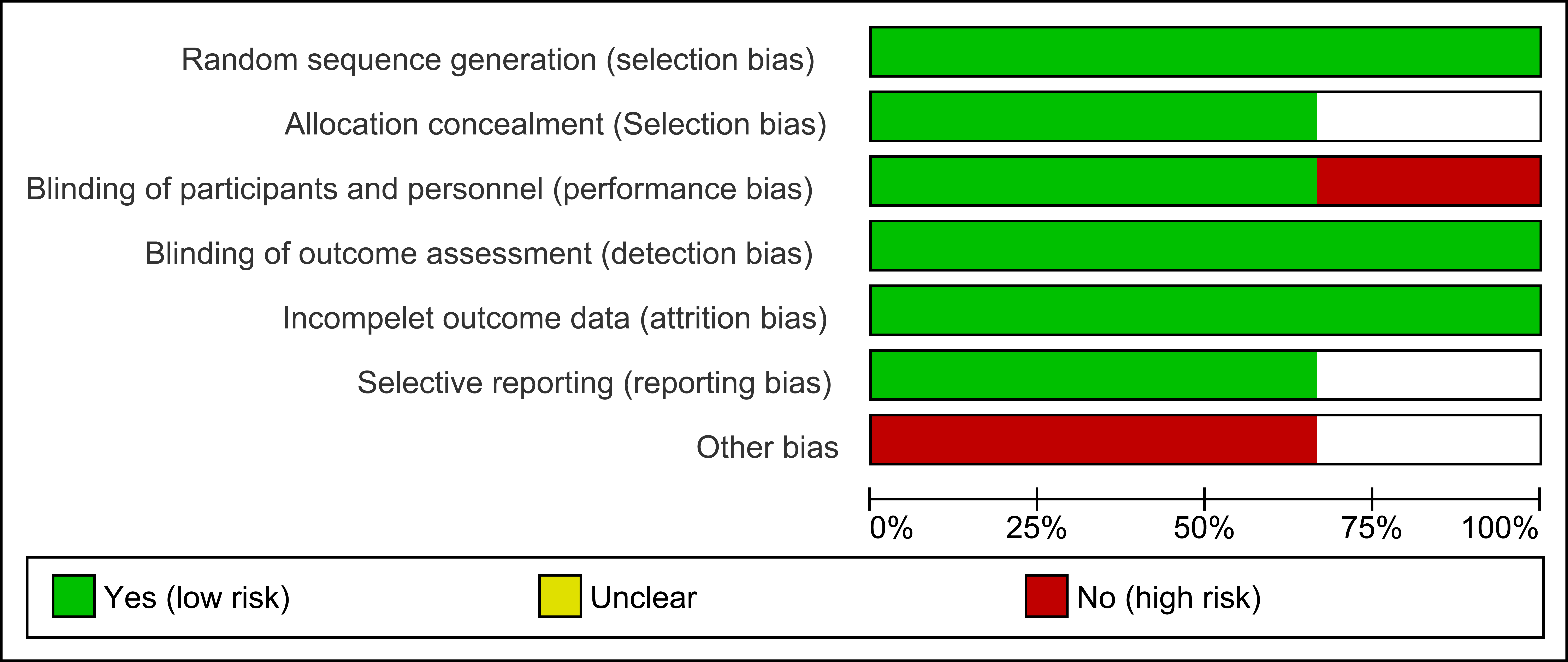
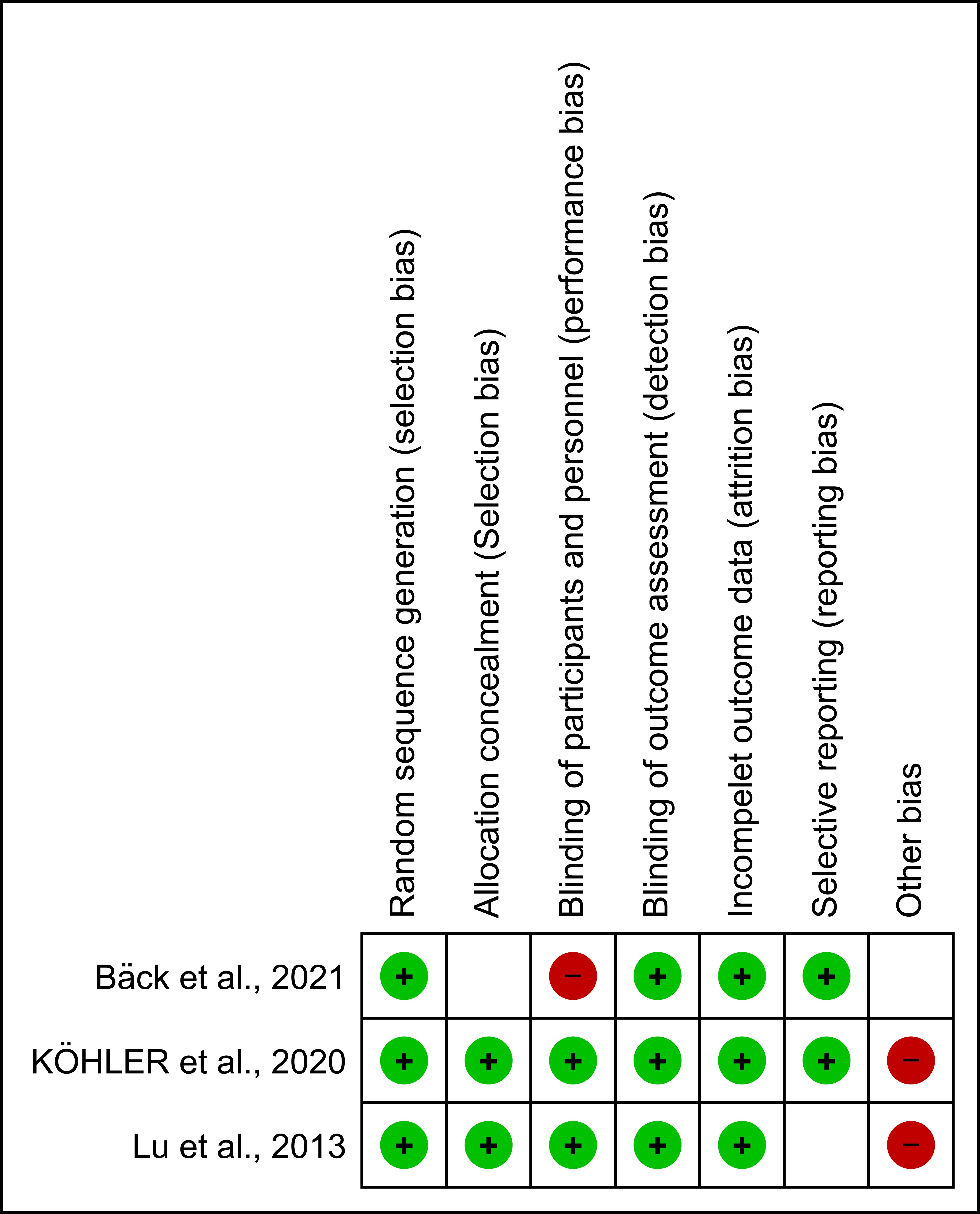
The risk of bias in randomized controlled trials was evaluated using the Cochrane Collaboration’s Risk of Bias (ROB) tool.10 Results are visually presented in a color-coded table, with red indicating high risk of bias, green indicating low risk, and yellow indicating uncertain risk due to insufficient information.
Results
Search results
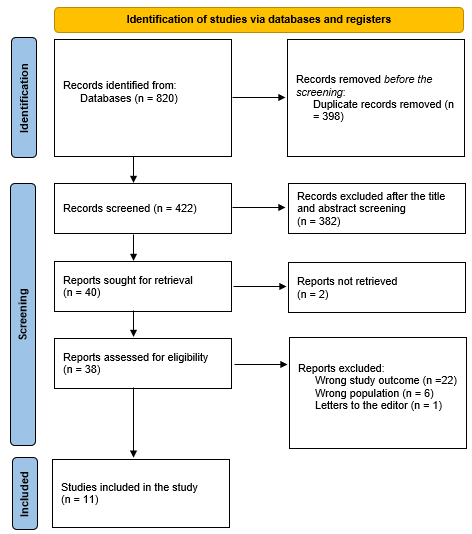
A comprehensive literature search yielded 820 potential study articles. After removing 398 duplicates, the titles and abstracts of 422 studies were screened for relevance, resulting in the exclusion of 382 articles. Two articles from the retrieved literature could not be accessed. The remaining 38 articles underwent full-text assessment, leading to the exclusion of 22 studies due to incorrect results, 6 studies due to inappropriate study designs, and 1 editor’s letter. Ultimately, 11 research papers met the inclusion criteria and were included in this systematic review. Figure 1 illustrates the study selection process using a PRISMA flowchart.
._study_selection_is_summed_up_in_a_prisma_flowchart.png)
Characteristics of the included studies
Table (1) presents the sociodemographic characteristics of the included studies. The 11 studies comprised a total of 782 participants, with 360 (46%) being female. The studies were conducted across various countries, including Sweden (3 studies),11–13 Finland (1 study),14 Pakistan (1 study),15 Norway (1 study),16 Germany (1 study),17 Malaysia (1 study),18 China (1 study),19 USA (1 study),20 and India (1 study).21 The publication years ranged from 199616 to 2021.14 The study designs included prospective cohorts (6 studies),11–13,18,20,21 randomized controlled trials (3 studies),14,17,19 a quasi-experimental study (1 study),15 and a retrospective cohort (1 study).16
Table (2) summarizes the clinical characteristics and outcomes of the included studies. Follow-up duration varied from 6 months15,16 to 12 years.12 Three studies15,18,21 reported no complications following arthroscopic surgery, while two studies reported low complication rates of 5% for arthroscopic subacromial decompression (ASAD),14 4% for diagnostic arthroscopy (DA),14 and 19.4% for arthroscopic acromioplasty.12
The findings suggest that ASAD is effective in reducing pain and improving function in patients with shoulder impingement syndrome (SIS) regardless of age or symptom duration.13–15,18,19,21 High long-term patient satisfaction was also reported following ASAD.11,13 Arthroscopic acromioplasty demonstrated good short-term outcomes for refractory or chronic SIS, with superior results compared to open acromioplasty over time.12,20
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tool, with scores categorized as low (<4), moderate (5-7), or high (>8). The risk of bias in randomized controlled trials was evaluated using the Cochrane Collaboration’s Risk of Bias (ROB) tool, with results presented in color-coded tables (Figures 2 and 3).
._risk_of_bias_graph.png)
._risk_of_bias_summary.png)
Discussion
Shoulder impingement syndrome (SIS) is a debilitating shoulder condition with an oftentimes complex and controversial treatment course. Nonoperative strategies are first-line, but their efficacy is not universally durable. Arthroscopy has emerged as a promising surgical alternative to open procedures, offering a minimally invasive approach to addressing shoulder pathology. However, its role and relative benefits for SIS remain incompletely defined.
This systematic review synthesizes available evidence on arthroscopic surgery outcomes for SIS, finding generally positive results. ASAD appears to yield meaningful improvements in pain and function for patients across age groups and symptom chronicity,13–15,18,19,21 with two studies supporting sustained patient satisfaction.11,13 Arthroscopic acromioplasty outcomes were superior to open surgery for refractory SIS cases, particularly long-term.12,20
These findings align with a meta-analysis by Liu et al. which found comparable clinical outcomes between arthroscopic decompression and conservative care for SIS, leading the authors to recommend initial nonoperative management with consideration of arthroscopy if symptoms persist.22 Similarly, Dong et al. advised that surgical options may be entertained for chronic SIS, with ASAD preferred over bursectomy or open decompression.23
The current review reinforces arthroscopy as a viable treatment for SIS refractory to conservative care, as it enables comprehensive diagnostic evaluation and therapeutic flexibility. Systematic reviews have found no clear differences in outcomes between ASAD and bursectomy24 or open decompression,25 nor definitive superiority of any surgical approach to nonoperative treatment.26 This equivalence underscores the need for judicious patient selection and an individualized stepwise treatment approach incorporating both surgical and nonsurgical modalities.
The low complication rate associated with arthroscopic surgery for SIS is encouraging, mirroring the safety profile reported in the broader arthroscopy literature. Observed complications, most frequently stiffness and capsulitis, appear amenable to conservative treatment and self-resolve. Careful patient selection, meticulous surgical technique, and specialized surgeon training likely contribute to these favorable safety outcomes.
Despite the apparent benefits of arthroscopic surgery for SIS, several knowledge gaps persist. Foremost is the lack of high-quality comparative effectiveness data across the clinical spectrum of SIS. Trials evaluating arthroscopic surgery against both nonoperative regimens and alternate surgical approaches, stratified by impingement etiology and severity, could refine indications and identify subpopulations likely to derive the greatest benefit.
Standardization of conservative treatment protocols and outcome assessment instruments is also critical. Establishing a benchmark nonoperative regimen would enhance study comparability and applicability to clinical practice. Consistent use of validated patient-reported outcome measures and quality of life instruments could improve documentation of the subjective patient experience.
Cost-effectiveness is another key consideration, as the rising utilization of arthroscopy for SIS carries significant economic implications. Robust economic evaluations, ideally conducted alongside clinical trials, are needed to quantify the incremental benefits of arthroscopy relative to alternative treatment approaches. These analyses should adopt both healthcare sector and societal perspectives to capture direct and indirect costs.
Finally, the optimal postoperative rehabilitation approach for arthroscopic SIS surgery remains undetermined. Trials comparing different exercise modalities, progressions, and intensities could help maximize recovery and functional outcomes. The efficacy of additional conservative adjuncts such as manual therapy and electrotherapeutic modalities also merits further exploration.
Limitations of this review
This review is not without limitations. The heterogeneity of included studies in terms of design, population, intervention, and outcome measures precludes a meta-analysis. The preponderance of observational studies limits causal inferences. Small sample sizes and inadequate follow-up in some studies may compromise the reliability and generalizability of findings.
Nonetheless, this review provides a comprehensive synthesis of current evidence on arthroscopic surgery outcomes for SIS. The robust search strategy, systematic screening and data extraction methodology, and application of validated quality appraisal tools enhance the validity of findings.
Conclusion
Arthroscopic surgery, particularly subacromial decompression, appears to be a safe and effective treatment option for SIS refractory to conservative management. Available evidence suggests arthroscopic approaches yield meaningful improvements in pain and function, high patient satisfaction, and lower complication rates compared to open surgery. However, comparable outcomes may be attainable through well-structured exercise therapy, emphasizing the importance of exhausting nonoperative options before considering surgery.
Opportunities for future research include high-quality randomized trials comparing arthroscopy to alternative treatments across the SIS spectrum, economic evaluations to establish cost-effectiveness, and studies optimizing postoperative rehabilitation. Consistent use of validated outcome measures and longer-term follow-up would strengthen the evidence base.