1. Introduction
Osteoarthritis (OA) is a progressive and chronic disease that can result in the patient’s increased pain and loss of function.1 It is considered one of the most common causes for joint pain and disability, while often also regarded as an age-related condition due to the increased occurrence of OA in patients that are 45 years old and above.2 OA is typically manifested by the loss of cartilage caused by a possible imbalance between the cartilage biosynthesis and degradation. The loss of cartilage that occurs due to damage or aging is not able to restore itself mainly due to the lack of circulation.3,4 Thus, various symptomatic treatments applied to temporarily alleviate pain, maintain, or improve joint function, and reduce disability of OA can only occur during early stages of onset, though unfortunately, none shows activity of slowing or reversing the progression of cartilage degeneration.5 Other measures such as surgery, can also be taken to assist in alleviat-ing OA symptoms such as osteotomy, total knee arthroplasty, or even arthroscopy. Even so, total regeneration of the damage cartilage still requires further additional treatment applications.2,6
Mesenchymal stem cells (MSCs) are an emerging research interest in the field of re-generative medicine due to its potential of multilineage differentiation into other cells, as well as its immunomodulatory potential in alleviating chronic autoimmune responses, or inflammation, on the damaged site.7–10 MSCs can be obtained from many different sources within the body such as bone marrow, adipose tissue, dental pulp, synovium, muscle, and other tissue.11,12 In current clinical practice of MSCs treatment, the generally used MSCs are that of Bone-Marrow derived mesenchymal stem cells (BM-MSCs) and Adipose-derived stem cells (ASCs).8,13,14 Both MSCs are constantly used due to their high affinity in expressing the best form of MSCs therapeutic features and multilineage differentiation capabilities. Although between both, ASCs is slowly viewed to be a much safer and effective alternative compared to BM-MSC, due to the found risk and limitation of BM-MSCs invasive harvest procedure that is associated with in-creased pain and morbidity.12–14 Despite that, BM-MSCs is currently still used in clinical practice due to its extensive therapeutic features and high affinity during treat-ment. Therefore, MSCs offers a promising solution to alleviate symptomatic knee (OA) through its pleiotropic and therapeutic features.9
The efficacy of using MSCs in the treatment of OA was found through several meta-analyses to have a significant impact on the treatment and was focused on improving physical function and psychometric measures of pain.2,15 Although various available data and research studies regarding MSCs has shown its potential in clinical use, there are still limited data of MSCs regarding actual long-term safety and efficacy in larger clinical trials.2,11 In some cases, MSCs was also found exhibiting limited survivability during injection in the target area, which offers another challenge in determining the underlying cause. This led to several conducted studies done to identify solutions in enhancing MSCs survivability and its scope of regeneration towards OA, through injecting MSCs using the intra-articular route or utilizing MSCs as an additional treatment therapy of existing treatment methods for OA.16–19 Intra-articular injection assist in enhancing MSCs efficacy by reducing amount of MSCs that are misdirected to a different target site and trapped due to its poor homing mechanism .4,6,20 This is due to in-tra-articular injection route being close to the joint injury site of OA, therefore reducing chances of “lost” MSCs.3,21
Aside from MSCs capable of acting as a main alternative in treating OA, the possibil-ity of MSCs acting as an additional treatment therapy in conjunction with previous treat-ment methods of OA is also present in multiple research studies.22–25 As mentioned previously, the current OA treatment methods are generally focused on reducing pain on the joint area through steroid injection or through bone realignment and joint re-placement. Another treatment option known as arthroscopy is also viable but is highly not advised due to its short-term pain alleviation for OA.26–29 However, one of the ad-vantages of arthroscopy as opposed to the current guidelines, is that arthroscopy assist in alleviating pain, inflammation, and restoring the damaged meniscus, through debris cleaning and surface-level meniscus repair, rather than injecting a pain-reliever or even removing bone sections through knee osteotomy, which can lead to a lot of possible com-plications.26,28,29 Arthroscopy is also minimally invasive than the other treatment methods, with less chances of risk. The treatment method of arthroscopy has shown to be effective in OA, just not in the long run. However, with the potential pairing with MSC therapy and arthroscopy, the structure repair of arthroscopy could be potentially boosted by the regenerative capabilities of MSCs, therefore leading to pain alleviation and cartilage regeneration through a minimally invasive and less risky procedure compared to other treatments.22,23 Additionally, arthroscopic procedure can manage to alleviate inflammation by removing inflamed synovium tissues,26–29 which can assist in MSCs survivability during transplantation and improve its effectiveness.
Regarding general MSCs treatment on OA, previous several systematic reviews have also reported improvements on the injury site, such as that of articular cartilage, sub-chondral bone, and joint-space width repair and regeneration.2,3,19,30 However, there are still limitations that the reviews provide such as heterogeneity complications of MSCs of the studies reviewed, as well as potential of risk bias assessment during publication. Thus, the assessment on MSC therapy on OA treatment application may be faced with challenges such as randomization, or potentially blinding. Although most have provided significant results regarding MSCs potential in treating OA.2,19
Therefore, the purpose of this study is to do a systematic review regarding the evaluation of MSCs effect on cartilage regeneration of knee osteoarthritis (OA), improving structural outcomes of the knee, as well as its efficacy during treatment methods of arthroscopy included in the studies.
2. Materials and Methods
2.1. Article Identification and Selection
This study was conducted in accordance with the Preferred Reporting Items for Sys-tematic Review and Meta-Analysis (PRISMA), following the NMA guidelines. Databases utilized as search platforms during the literature search include Cochrane (2022), EM-BASE (2022), MEDLINE (2022) and PubMed (2022). Literature from these databases was gathered through search terms: mesenchymal stem cells (MSC) in treating OA or OA arthroscopy and mesenchymal stem cells treatment (MSC). Additionally, the literature was also bounded to only accepting human studies and the English language. Furthermore, ethical approval and informed consent for the systematic review was not required since all data are acquired from previously released studies and provided no harm to participants within this study.
2.2. Study Inclusion and Selection
Other inclusion factors included in the study was studies with level of evidence I or II, which are studies with randomized controlled and non-randomized controlled trials, respectively. The study is avoiding level of evidence 3 or greater to avoid inaccurate or speculative accounts of data. As for the screening, four investigators (Y, B.P., R.H., and B) in-dependently screened the titles, abstracts, and full texts for literature control. The articles were followed with inclusion criteria and subsequent unmatched literature was discard-ed. References provided is also additionally screened to identify proper literature or missing literature used during query.
2.3. Data Extraction and Synthesis
Two authors (Y. and B.P) independently extract data on included studies and presented those data on a spreadsheet consisting of subject population, treatment details, followup duration, source of the immunophenotypic characterization of stem cells, number of injections, outcome measures, route of administration, type and source of stem cells, and the effect of each cell injections on the structural outcomes. An additional qualitative synthesis was also performed for the heterogeneity in both interventions and outcome measures.
2.4. Risk of bias assessment.
Four investigators (Y., B.P., R.H., and N.F.N.) independently assessed the risk of bias using Downs and Black scale, which consists of a series of twenty-seven questions relating to an overall quality report of the study, both external validity (study results) and in-ternal validity (bias or confounding). In detail, the scale measures the questions based on quality of reporting (10 questions), external validity (3 questions), internal validity (bias and confounding, 13 questions) and statistical power (1 question). Down and Black scale have a possible of maximum 32 points when answered, with 5 points provided by statis-tical power question. In this model, the scale was modified and simplified, with statistical power only receiving 1 point, greatly improving the statistical data, and providing a meaningful difference between the results. The final modified Downs and Black scale will be categorized by grade of “excellent” (25-28 points), “good” (20-24), “fair” (15-19), or “poor” (<15 points).
2.5. Data Analysis
Resulting data recorded through the Downs and Black scale will be assessed and de-termined of the included studies results regarding the potential effects of mesenchymal stem cells and its possible combined treatments through arthroscopy. Results analyses, as well as the potential discussion from the various studies data, will be compared between the study’s results to reach a unanimous inferred result within the literature discussion. An additional table that includes the important results of the various studies will also function as the base of data analysis of this systematic review.
3. Results
3.1. Study Characteristics and Selection
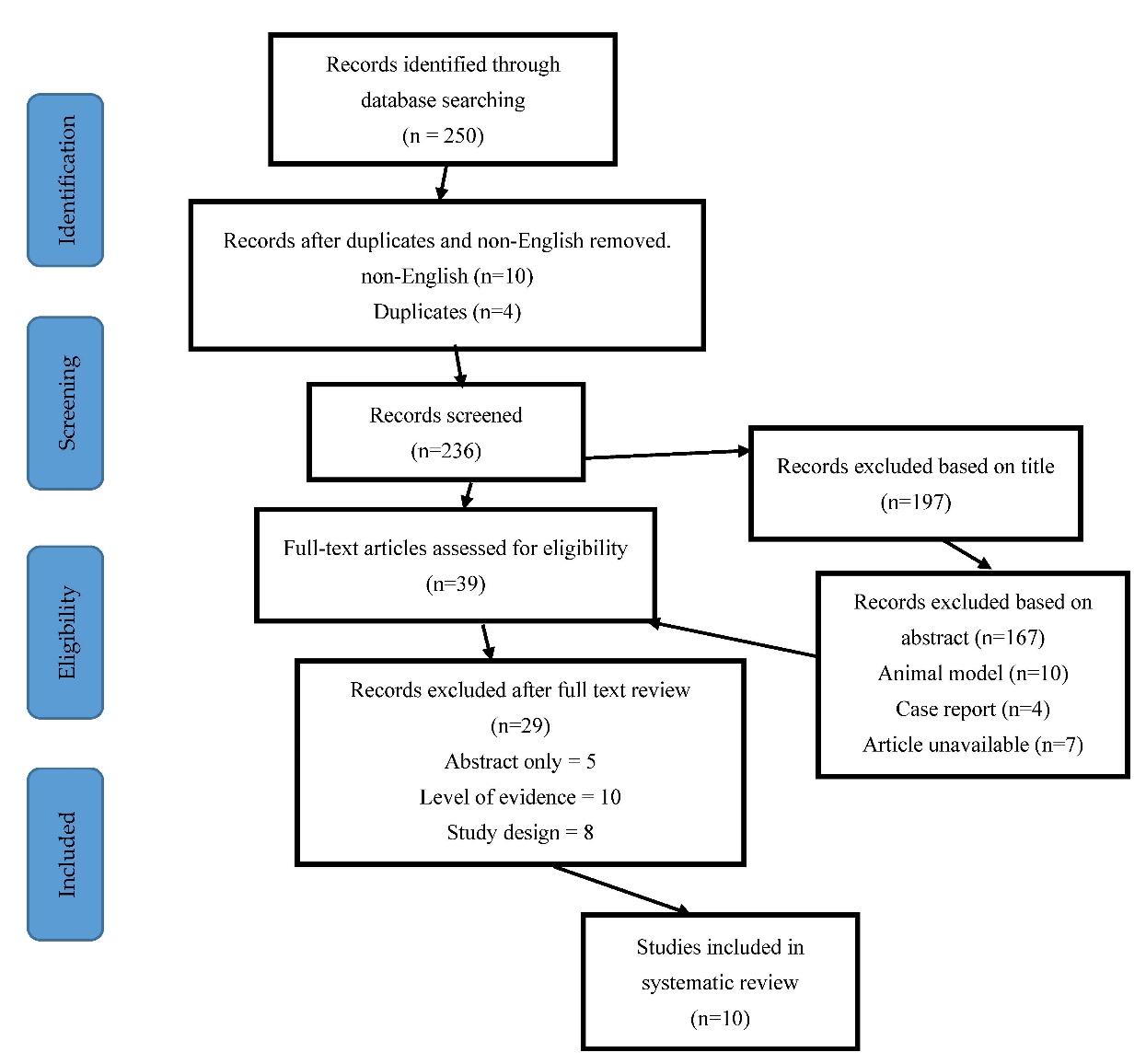
The full detail of database query and literature inclusion process and selection can be seen on Figure 1. The total of processed literature reached a total of 250 studies and after undergoing screening assessment using the inclusion criteria, the total viable studies that will be utilized within the systematic review amounts to around 18 studies.

3.2. Description of included studies
Detailed description of the provided studies, as well as its characteristics are de-scribed in Table 1 below according to each cell therapy descriptions. As it is with the systematic review title, all patients treated with MSCs is currently undergoing or has a history with knee OA. The patients are injected with MSCs, mostly through intra-articular injection to the knee, and was monitored improved behaviour or functionality within the injured site. This was done through a series of pre-set value measurement for pain, functionality, or radiological measures to observe the potential effects of the MSC treatment or combined treatment with arthroscopy, on the injury site overtime. The indexes or guidelines used for the value measurements include the “Western Ontario and McMaster Universities Osteoarthritis Index” (WOMAC), “Visual Analogue Scale” (VAS), “Knee Injury and Osteoarthritis Score” (KOOS), and “International Cartilage Repair Society Score” (ICRS). Additionally, results of treatments on OA can also be further visualized through radiological measures such as “Magnetic Resonance Imaging” (MRI) or surgery. Available real-time images of the treatment site of the injury are a real advantage, since it can notify changes in cartilage thickness, cartilage repair or regeneration, joint-space width, cartilage size and depth defects. Kellgren-Lawrence grade scale of OA conditions was also used to define any possible major changes in the knee structure. Six studies even under-gone a follow-up measure of the treatment in order secure a better definitive data available for long-term treatment and application using MSCs.
OA, osteoarthritis; AD-MSC, adipose-derived mesenchymal stem cells; BM-MSC, bone-marrow derived mesenchymal stem cells; hUCB-MSC, human umbilical cord blood derived mesenchymal stem cell; Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC); Visual Analogue Scale (VAS); Knee Injury and Osteoarthritis Score (KOOS), and International Cartilage Repair Society Score (ICRS). Identified CD-Markers; (+) CD73, CD49d, CD29, CD90, and CD105. dGEMRIC, delayed gadolinium-enhanced MRI of cartilage; IKDC, International Knee Documentation Committee.
3.3. Interventions
Mesenchymal stem cells used in the various studies within the systematic review was derived from many sources such as Bone-Marrow-derived mesenchymal stem cell (BM-MSC), adipose-derived mesenchymal stem cell (AD-MSC), and umbilical cord-blood (UC-MSC). Most of the MSCs used in the studies are autologous as opposed to allogenic method, meaning that most of the MSCs transplantation within the patients are gathered from themselves and only a few of MSCs are from other donors. Specifically, two studies utilized BM-MSC,31,33 each of which uses different sources that of one autologous and the other is allogenic. Six studies utilized AD-MSC,30,36 in which five are autologous and one is allogenic sourced. Finally, one study utilized hUCB-MSC25 and was allogenic sourced. The method of extraction of these MSCs all differ according to the source where each are isolated. AD-MSC are usually commonly isolated through tumescent liposuction or through lipoaspiration.17,18,30,32,34,36 As for BM-MSC, the bone marrow aspiration method (BMA) method is often used,33 and as for UCB-MSC28, the stem cells are isolated during neonatal delivery. Successful isolation of MSCs through these methods enables the possibility of undergoing the treatment.
CD markers and immunophenotypic typing was also done in some studies; with six studies reporting CD markers,30,31,37 three studies not reporting,33,35 and one study created conformed cultures profile to ISCT criteria on MSCs.25 In detail, the six reporting studies reported positive marker of CD34, CD90, CD105, CD73, CD94d, CD29, CD31, CD45, and HLA-DR. Three of the studies also include the negatively expressed actions, although some that is included conflicts with positive markers in other studies such as HLA-DR, CD34, CD45, and only one new marker CD14. The stem cells are all mostly injected through intra-articular injection within the studies,17,33–35 however, there are also studies that are unclear in the method of injection.25 Specifically, these studies only reported direct injection towards the knee site of injury. Furthermore, there are also one study that uses US-guided injection and NR method of injection. Arthroscopic procedure was mostly done prior to MSCs treatment injection, with seven studies performing the procedure to clean and repair the damaged cartilage site,9,17,31,32 and the other three studies reporting that future utilization of ar-throscopic microfractures may help improve the study’s results.35
3.4. Risk of Bias Assessments
The risk of bias across the ten studies were low to moderate at best. According to the score value determined by the Down-and-Black scale, eight of the ten studies have low risk of bias and one of each studies left has moderate and high-risk of bias, respectively. The participants and study population are clearly stated in Table 1 of the systematic review and is well defined. Although there are missing or unreported data within two-three studies that can be well used during the systematic review and may cause unclear risks.
3.5. Effect of MSCs on Structural Outcomes of OA
All the ten studies have reported and assessed the effect of MSCs application on all outcome measures such as osteoarthritis pre-set value by WOMAC, VAS, KOOS and ICRS, as well as through radiological imaging using MRI, which can identify potential regeneration activity occurring in the articular cartilage during MSC treatment. Nine of the studies reported their findings using MRI technology9,17,31,32 and among those, seven studies have recognized a potential regenerative property regarding cartilage thickness, increase in PCI value relating towards cartilage repair or regeneration, knee cartilage, femur, tibia, and patella, as well as the reduction in T1 relaxation time.9,12,31,33 The other two studies however have conflicting or unclear results. Pers et al.36 have noted that only three of six patients under the given doses seems to have a slight significant improvement in cartilage repair or regeneration, with other patients showing little or no changes at all using MRI technology. Similar can be said for Song et al (2019), in which during the research, only the high doses seem to produce apparent desired results compared to those in lower doses. Although, the study done by Song et al37 does not completely deny the effect of MSC treatment on OA, for the low-mid dosages still produces minor changes. As for the studies without the MRI imaging results, the patients were assessed through VAS, ICRS, and TAS, TT, and TLS angles changes which was observed through surgery.32
The other outcome measure done across the studies was the qualitative assessment through OA pre-sets measurements using WOMAC, ICRS, KOOS, and VAS. Each of these measurements are not used all-together in the studies, however, only two or three are included. Four studies utilize VAS in assessing MSCs treatment on knee OA9,25,33 and most of the results reported a significant improvement of the resulting value on their experiment. VAS values were shown to be reduced and thereby, increasing functionality within the injured site. Four of the studies has all reported a good significant improvement using MSC treatment on OA, with many presets assessment value being much more optimal compared to pre-treatment of the patients. VAS was also combined with IKDC evaluation score to measure the pain and functionality of the injured site of the patient. Aside from VAS, WOMAC is the next assessment quality pre-test that is used frequently and is utilized by four of the studies in the review.30,33 WOMAC functionality is to re-port the pain, function, and mobility of the patient. Overall, WOMAC has provided report for each of its assessment quality regarding OA, with Vega et al. reporting reduced pain,33 Pers et al., reporting significant improvement in pain, functional, and mobility,36 as well as with Song et al., research, in which the mean standard across the pain and function value are all reduced; suggesting a significant improvement of the injured site.30
KOOS and ICRS are used less frequently and is only utilized by two of ten studies in the literature review.31,32 Despite its non-frequent usage, both has reported significant effect of MSC treatment in which MSC was shown to have increased higher knee functionality. Furthermore, ICRS shows promising results in Kim et al, in which MSC injection combined with marrow stimulation and potential arthroscopy promotes cartilage regeneration.32 Lastly is both surgery and x-ray, which is utilized by two of the systematic review study.17 Assessment methods are generally available, so dire requirement in OA is directed towards radiological measures such as MRI. Surgery and X-Ray allows similar identification usage as MRI. Results of surgery in one of the studies identifies positive outcome after 12-24 months; showing the beneficial outcome of stem cells. As for x-ray, the method is currently in a joint-tandem with the Kellgren-Lawrence grade assessment method, which is like the previous qualitative assessments.
3.6. Arthroscopy Procedure
Five studies perform MSC injection following Arthroscopy procedure under spinal anaesthesia. Arthroscopy examination was initially conducted to assess cartilage defect. The cartilage lesion was measured with a calibrated arthroscopic probe and graded according to the international cartilage repair society (ICRS) cartilage injury classification. Multiple drill holes with approximately 3-5 mm in diameter and 2-5 mm deep were subsequently created to implant the MSC intra-articularly at the surface of the cartilage lesions. Kim et al extracted the synovial fluid prior to injection.32 After the procedure was done, the wound was then closed and compressed with bandages completed with knee splint.5,32
4. Discussion
The evidence provided in the literature above was systematically reviewed for the effectiveness of mesenchymal stem cells (MSCs) in improving OA treatment process. The data evidence was comprised of controlled trials, randomized and unrandomized, ten studies that was regarding MSC treatment on OA. There are a total of 290 patients in the included studies; eight of which are high quality; the other two is moderate and low quality, respectively. Based on consistent evidence; MSC was shown to have a beneficial effect on the regeneration of articular cartilage when supplied enough dosage.30,36 Further-more, application of MSC treatment on knee OA seems to also be reducing sense of pain and increase knee functionality. These results were shown through the many pre-sets quality assessment results and radiological measurements. Although there are still some incomplete details such as the proper amount of dosage needed to yield maximum effect, or in cases during Pers et al.,36 in which only three of the high dosage patients have any impactful effect on their OA conditions during MSC treatment. Furthermore, many of the literature used all have a degree of varying variables used within the study. So, significant traces of heterogeneity might have impacted the results study through its modest sample size, methodological limitations, or publication bias potential, much like previous systematic reviews regarding MSCs as well as in this current review.12,19
As for determinative consistent evidence provided by the studies used; up to six studies have shown that MSC treatment/therapy on knee osteoarthritis have borne beneficial effects such as basic stages of regeneration, reducing pain through its immunomodulatory effect, and potentially further increasing knee functionality.9,31,33 Additionally, follow-up injections of MSCs by the studies, have shown to have also aided in increasing the regeneration effects of articular cartilage, as well as increased knee functionality. Other increased factors such as a balanced joint-space width and subchondral bone structure can also be strengthened/repaired as seen in the informative results by Song et al., & Lee et al., of MRI on OA treatment with MSC and arthroscopy.17,37 Furthermore, several quality assessments such as WOMAC, ICRS, KOOS, and VAS have shown even more evidence regarding the potentiality of MSC as a treatment method when combined with arthroscopy.17,25,31–34
In terms of specific MSC’s efficacy, the studies provided in the systematic review utilizes mostly BM-MSCs or AD-MSCs combined with a treatment method of arthroscopy.17,25,32–34,36 Arthroscopic treatment was done to clean the injury site and perform surface-level repair of the cartilage damage prior to MSCs treatment.26–28 Based on the study results, both BM-MSCs and AD-MSCs showed improvement in all the expected outcome measures of OA through improved VAS, KOOS, WOMAC, and ICRS scores, as well as good radiographic results from X-Ray and MRI-T2 scans.17,18,32,34,35,37 This suggests that both BM-MSCs and AD-MSCs are viable choices for OA treatment utilizing MSCs. One thing to note regarding MSCs usage is through its dosage as well.36,37 While both BM-MSCs and AD-MSCs reported improvements of cartilage repair and regeneration of OA, the included study of Pers et al.,, reported that AD-MSCs produced significantly higher functional improvement in OA outcome measures when administered in high dosages.36 This can be attributed to AD-MSCs treatment being able to increase its effectiveness through increasing the dosage. Additionally, AD-MSCs are easily harvestable compared to BM-MSCs so the amount yield will be higher and have less risk involved during harvest compared to BM-MSCs. Based on that, utilizing AD-MSCs as a treatment method for OA is superior in terms of yield amount, safety, and efficacy compared to BM-MSCs when administered in high dosages.7,13,17,21 This also aligns with previous systematic reviews regarding effect of MSCs sources on treating and managing OA, in which their studies shows that AD-MSCs are superior in terms of efficacy and safety compared to BM-MSCs,12,38 although it is mentioned that in some OA cases, AD-MSCs are only effective for pain relief, which means that the usage of BM-MSCs is not all void of its uses.12
Most of the MSCs treatment was injected into the injury site through intra-articular injection and assisted with arthroscopic procedures.17,18,33,34,37 Intra-articular injection is the most preferred method of injection as it provides the nearest entry point for the MSCs to home in the damaged site.3,4,19,24 Results from the studies are good with no mention of any MSCs trapped in any organ sites or that there is less MSC activity within the damaged site. Thus, suggesting that intra-articular pathway is a very advantageous route of administration for MSCs as it eliminates common MSCs problem of entry and being trapped,20 which results in more MSCs to be concentrated on the damaged site.9,16 However, another common issue that prevents MSCs from expressing its therapeutic features might come from the harsh inflammatory conditions of the damaged cartilage site. These microenvironment conditions might be due to inflammation, hypoxic conditions, or even oxidative stress, which all are very detrimental to MSCs survival11[40-42]. The added treatment method of arthroscopy might potentially have aided in alleviating these microenvironment conditions based on the included studies result. In each outcome measures, all studies reported considerable increase in functional improvement and pain relief with no mention of reduced performance.17,18,32,34–37 While arthroscopy treatment procedure is commonly not ad-vised for OA treatment due to its short-term pain relief and repair,5,26,27,39 the effects of clearing inflamed tissue (synovium) in the damage site or performing surface-level repair in the damaged articular cartilage29 might be enough to assist in MSCs survivability by lowering the harsh microenvironment in the site, which can lead to an increase MSCs effectiveness in regenerating amount of lost chondrocytes.9
Aside from using arthroscopy and intra-articular route of administration, two of the included studies utilized scaffolds to support MSCs cell proliferation, adherence, differentiation, and spreading.31,32 Both Toan et al., and Kim et al., used a fi-brin-glue network scaffolds to increase the MSCs efficacy in treating OA.31,32 Results of the scaffold MSCs treatment reported a higher KOOS score, which is increased knee functionality, as well as evidence of cartilage repair through MRI radiographic imaging. Other qualitative measurements such as VAS also showed a reduction in pain measurement. Through this systematic review, the true benefits of scaffold to boosts MSCs efficacy is not explored since two of the ten included studies only utilizes MSCs scaffold method. How-ever, there is evidence from both studies and other publications regarding MSCs combined with scaffolds11[42], that it might also be a potential choice in boosting MSCs treatment effectiveness. This method coupled alongside injecting MSCs through the intra-articular route and with the added treatment of arthroscopy, can potentially produce a higher effectiveness in alleviating microenvironment inflammation of the damaged site.
The systematic review has limitations. Due to its small literature count with only ten provided studies, the result of the systematic review has a chance to still be supplied with new and additional information. Additionally, with such few studies, the chance of there being a heterogeneity factor of the experiment/research across the literature used is considerably high. The heterogeneity stems from different controlled variables or used variables such as study populations, MSC source and contents, doses, frequencies, and administration schedule. The same thing can be applied in this systematic review as it is difficult to pinpoint studies that uses similar dosages, MSCs, as well as using a prior arthroscopy treatment, therefore may cause certain results from this review to be different during different MSCs treatment on OA. Although heterogeneity causes potential comparison issues; the high consistent evidence of MSCs potential and effective role as a new media to be applied in OA still provides a solid foundation for future research, cases, or reviews regarding the true potential of MSCs in increasing/improving cartilage outcomes. Toan et al., one of the included studies, has also been shown the exact behaviour of MSCs and its MSCs.31 Furthermore, the research results of the study were assessed with a variety of both quality assessment materials and radiographic imaging. However, in the end MSCs still remind a mystery and there is still no definitive data, although its potential is clear and can be combined with existing methods of treatment; the process will accelerate quicker, and the issue of long treatment duration will diminish.
5. Conclusions
The systematic review, constructed upon ten phase I or phase II clinical trials, showed consistent evidence of information for a beneficial effect of intra-articular injections of MSCs on articular cartilage, including the subchondral bone. Issues regarding heterogeneity and injected MSCs, early stage of trails, methodological limitations, bias, modest sample sizes, and limited studies; more incentive into finding and researching other works to provide full comprehensive is required, before MSC therapy is recommended in the management of OA.
Author Contributions
Conceptualization, Y.Y; K.L.D; C.R.S.; methodology, Y.Y; K.L.D; C.R.S; A.W; D.M; I.R.D.; software, R.H; N.F.N; B.Y.C.P.; validation, K.L.D; C.R.S; A.W; D.M; I.R.D.; formal analysis, Y.Y; K.L.D; C.R.S.; investigation, A.W; D.M; I.R.D.; resources, Y.Y; K.L.D; C.R.S.; data curation, Y.Y; K.L.D; C.R.S; A.W; D.M; I.R.D.; writing—original draft preparation, Y.Y; R.H; N.F.N; B.Y.C.P.; writing—review and editing, Y.Y; R.H; N.F.N, K.K; B.Y.C.P.; visualization, Y.Y; R.H; N.F.N; K.K.; B.Y.C.P.; supervision, , K.L.D; C.R.S; A.W; D.M; I.R.D.; project administration, Y.Y; R.H; N.F.N; B.Y.C.P.; funding acquisition, C.R.S; A.W. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by PT. Prodia StemCell Indonesia.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
Not Applicable.
Conflicts of Interest
The authors declare no conflict of interest.