Introduction
Total Hip Arthroplasty (THA) is a key advancement in orthopaedic surgery, offering a lifeline to those suffering from debilitating hip pain across many clinical conditions.1 By alleviating pain, restoring mobility, and enhancing quality of life, THA marked its significance among treatments for hip disorders.1,2 Today, with over 500,000 procedures conducted annually in the United States, the impact of THA is profound and far-reaching.1
THA emerges as the treatment of choice for patients who failed conservative treatments or previous surgical interventions for hip pathologies.3 This procedure is indicated for persistent pain, significant reduction in daily activities, or considerable disability due to deformity and painless limitation in range of motion.3 The hip functions as a “ball-and-socket” joint, where the femoral head and acetabulum enable fluid motion. Disruptive conditions such as osteoarthritis, inflammatory diseases, and others, can precipitate joint deterioration, causing pain and functional loss.4 Since its advent, THA has revolutionized the management of these conditions with success rates that emphasize its efficacy and reliability.5
The rise in life expectancy predicts an increased prevalence of osteoarthritis, projecting a doubling in THA demand by 2030.6 This emphasizes THA’s role in maintaining mobility and independence in aging populations. However, outcomes of THA can be influenced by patient demographics such as gender, age, and socio-economic status.7,8 While THA carries inherent risks, the careful application of surgical approaches can significantly mitigate complications, maximizing patient satisfaction.9 There are more than six approaches to THA and of these, DAA and PA are the most used approaches worldwide.10,11
Amidst this backdrop, the selection of surgical approach for THA has been a focal point of debate.12 The 2020 guidelines from the American Academy of Orthopaedic Surgeons (AAOS) highlight that evidence found no clinically significant differences in patient-reported outcomes (PROMs) between THA approaches in osteoarthritis patients.12 Similarly, the National Institute for Health and Care Excellence (NICE) in 2020, and data from the National Joint Registry, stress the variability in approach preference, attributing the choice to the surgeon’s training, experience, and the patient’s unique clinical circumstances.13
Considering the ongoing debate regarding the most appropriate surgical approach for THA, our manuscript undertook an umbrella review of systematic reviews and meta-analyses (SRs/MAs) of randomized controlled trials (RCTs) comparing DAA to PA. Our goal was to assess the quality of these reviews, discern similarities and differences, explore the reasons for discrepancies, and articulate a well-founded conclusion regarding the optimal surgical approach.
Methods
Study design, criteria for inclusion and exclusion
We registered our protocol on PROSPERO (CRD42023450069). We included SRs/MAs of RCTs focusing on patients undergoing primary THA regardless of its indication, with DAA compared to PA, evaluating operation duration (OD), blood loss (BL), length of hospital stay (LOS), pain levels using the Visual Analogue Scale (VAS), hip function using the Harris Hip Score (HHS), incidences of complications including dislocations, fractures, groin pain, heterotopic ossification, infection, and prosthesis alignment, specifically the abduction and adduction angles. We excluded SRs/MAs that assessed VAS and HHS based on intervals rather than at specific time points to minimize heterogeneity and ensure the comparability of MAs.
Literature search
We searched MEDLINE, Embase, and Cochrane databases, from inception until August 23, 2023, without language restriction, with the help of a medical librarian (O.Z.). We used Medical Subject Headings (MeSH) terms and keywords relevant to “total hip arthroplasty”, “direct anterior approach”, “posterior approach”, “meta-analysis”, “systematic review”, and “randomized controlled trials” (Appendix 1). We manually reviewed the citations within the included SRs/MAs, narrative reviews and contacted experts in the field to ensure no relevant study was overlooked.
Quality Assessment
Title/abstracts and full-text screening, data abstraction, and the quality assessment of the included SRs/MAs using A Measurement Tool to Assess systematic Reviews 2 (AMSTAR-2) were completed in duplicate and independently by pair of reviewers (J.E.N., L.A.A., M.Madi., M.Mzeihem. and M.H.). Disagreements were resolved through discussion with a content expert (M.N.).
Data synthesis and statistical analysis
We gathered information on study population, intervention, comparator, and outcomes, as well as the methodology of each SR/MAs. For each outcome included, we constructed figures displaying the effect size estimates and 95% confidence intervals (CI) derived from each direct meta-analysis (DMA). Additionally, we developed matrices to evaluate discrepancies between the results of SRs/MAs that assessed the same outcome, detailing the included RCTs in each DMA, their corresponding data, and the quality assessments.
We calculated the weighted mean for continuous variables using the formula if a relevant mean was not reported in the SR/MA for extraction, where “x” represents the variable and “w” the weight.
Results
Our search strategy yielded a total of 5,252 citations, from which we reviewed the full texts of 213 papers. Among these, 11 SRs/MAs of RCTs addressed our research question11,14–23 and were included in our umbrella review [Figure 1].
Characteristics of the included SRs/MAs
Population characteristics
Within the 11 SRs/MAs11,14–23 included, the number of RCTs examining the direct comparison between DAA and PA ranged from 4 to 11 per SR/MAs, resulting in sample sizes ranging from 310 to 932 participants, respectively. The inclusion of the network meta-analyses (NMA)16,23 extended this range, varying from 8 to 63 RCTs per NMA and yielding sample sizes from 822 to 4859 participants, respectively. The participants were predominantly older adults, as reported by 10 SRs/MAs.11,14,16–23 Baseline Body Mass Index (BMI) was reported across eight SRs/MAs.11,14,17,19–23 Follow-up duration was reported in seven SRs/MAs,11,14,17,18,20,22,23 providing a comprehensive overview of the demographic and clinical characteristics of the study populations [Table 1].
Meta-Analysis Methods
Software and Type of Analysis
Among the 11 SRs/MAs11,14–23 included, the most used software was RevMan. Of these, nine SRs/MAs conducted a DMA, two performed an NMA, and one conducted both types of analyses. Most of these SRs/MAs accounted for confounders by utilizing sensitivity analysis [Table 2].
Effect measures
In all 11 SRs/MAs, mean difference (MD) or standard MD (SMD) was reported, while odds ratio (OR) and relative risk (RR) were each reported in four SRs/MAs [Table 2].
Definition of approaches “Direct Anterior Approach” and “Posterior Approach”
Only two SRs/MAs11,23 explicitly defined both “DAA” and “PA”. The remaining nine SRs/MAs14–22 did not provide definitions for any THA approach [Table 2].
Quality assessment of the included SRs/MAs using the AMSTAR-2 tool24:
Among the 11 SR/MAs11,14–23 included in our umbrella review, only two19,23 were assessed as low quality, while the quality of the remaining nine SRs/MAs11,14–18,20–22 was rated critically low. This low quality can primarily be attributed to deficiencies in one or more critical domains (Items 2, 4, 7, 9, 11, 13, and 15) as outlined by the AMSTAR-2 tool24 [Table 3].
@attachment
Outcomes assessed
Operation duration (OD)
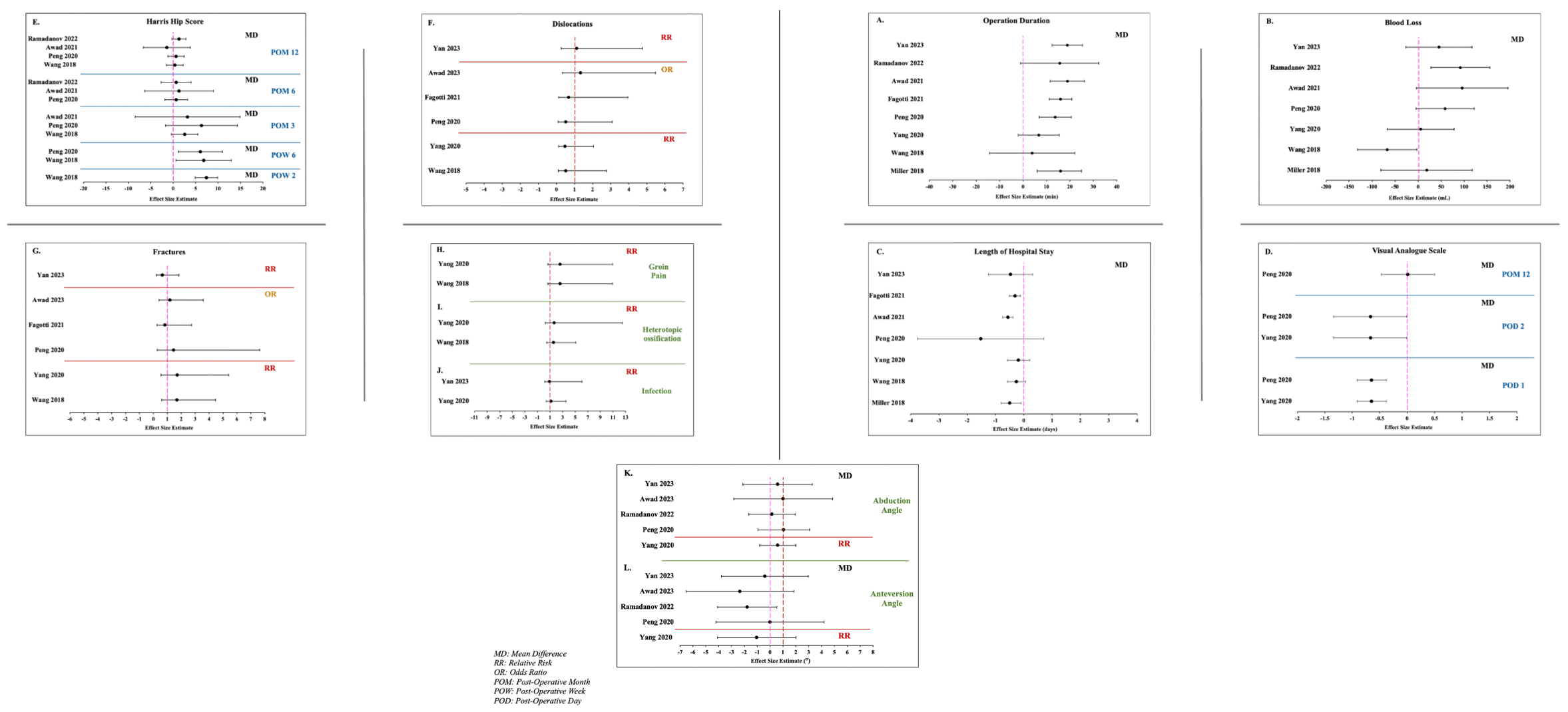
Of the eight DMAs11,15,17,19–23 assessing OD, five15,17,19,20,23 reported significant findings, indicating a longer OD when undergoing THA using DAA compared to PA (MD range 13.74 to 18.92). The remaining three DMAs11,21,22 did not demonstrate significant differences [Figure 2A]. These DMAs were compiled in a matrix to investigate the reasons behind this discrepancy [Appendix Table 1].

Blood loss (BL)
Among the seven DMAs11,15,19–23 assessing BL, one DMA21 reported significant findings, indicating increased BL when undergoing THA using DAA compared to PA, with a MD of 91.87 (27.99, 155.74). Conversely, another DMA22 reported that PA was associated with significantly higher BL than DAA with a MD of -67.02 (-131.46, -2.58). The remaining five DMAs11,15,19,20,23 did not report significant differences in BL between the approaches [Figure 2B]. These DMAs were compiled in a matrix to investigate the reasons behind this discrepancy [Appendix Table 2].
Length of Hospital Stay (LOS)
Of the seven DMAs11,15,17,19,20,22,23 assessing LOS, three15,17,19 reported significant findings, indicating a longer LOS when undergoing THA by PA compared to DAA (MD range -0.31 to -0.56). The remaining four DMAs11,20,22,23 did not demonstrate significant differences [Figure 2C]. These DMAs were compiled in a matrix to investigate the reasons behind this discrepancy [Appendix Table 3].
Discrepancies observed in DMAs for OD, BL, and LOS outcomes can be attributed to various factors related to the selection of studies. Exclusions due to non-randomization, language barriers, comparisons of different approaches (e.g., PL vs DAA), and the omission of studies published outside the search period all played a role. Additionally, inconsistencies in reporting effect sizes for the same trials contributed to the heterogeneity of results. Such inconsistencies can potentially justify the discrepancies encountered across DMAs.
Visual Analogue Scale (VAS)
At post-operative day (POD) 1, two DMAs11,20 found significantly less pain using DAA vs PA, with a MD of -0.65 [-0.91, -0.38], whereas one NMA18 found no significant difference. At POD2, similar findings were reported by two DMAs11,20 with a MD of -0.67 [-1.34, -0.01] with one NMA18 reporting no significant results.
No significant differences were observed at post-operative week (POW) 2 by one NMA,18 nor at POW6 by either the DMA15 or NMA.18 At post-operative month (POM) 12, one DMA20 also found no significant differences [Figure 2D].
Harris Hip Score (HHS)
Wang et al.22 found significant improvement in hip function at POW2 for THA via DAA over PA, with a MD of 7.41 (4.91, 9.92). By POW6, both DMAs20,22 and a NMA18 reported better outcomes for DAA, with MDs of 6.05, 6.80, and 3.7, respectively. However, at POM3, three DMAs15,20,22 and one NMA18 showed no significant differences in HHS results. At POM6, three DMAs15,20,21 similarly showed no significant differences. By POM12, all four DMAs15,20–22 continued to show no significant variability in HHS [Figure 2E].
Complications
Assessing post-surgical complications, all six DMAs11,14,17,20,22,23 and one NMA23 showed no significant differences for dislocations [Figure 2F] and fractures [Figure 2G]. Groin pain and heterotopic ossification rates, evaluated in two DMAs11,22 also lacked significant differences [Figures 2H and 2I, respectively]. Similarly, infection rates in two DMAs11,23 and one NMA23 were not significantly different [Figure 2J].
Prosthesis Alignment
When evaluating abduction and anteversion angles, all five DMAs11,14,20,21,23 along with one NMA23 showed no significant differences [Figures 2K and 2L, respectively].
Discussion
Evidence regarding the safest and least complicated approach to THA still stirs controversies is controversial. Considering that, this umbrella review sought to investigate possible differences in DAA and PA to THA regarding functional and surgical outcomes. In this study, 11 SRs/MAs of RCTs were analysed to compare the efficacy and safety of THA using DAA vs PA. Many variables, intra-procedural and post-procedural, were assessed and SRs/MAs included were evaluated for the potential causes of the discrepancies among them.
DAA was associated with longer OD compared to PA. One notable feature of DAA is its distinct method of femoral preparation, which is not required in PA. DAA involves a comprehensive release of deep structures, such as the posterior capsule and the piriformis, especially crucial during the elevation of the femur.25 This process of gradually releasing the deep structures prolongs the preparation time of the femoral canal for DAA.25 While OD should be recorded as the time from skin incision to skin closure, the included SRs/MAs did not address their definition of OD including whether this timeframe encompassed anaesthesia administration or the application of dressings.26 Hence, the accuracy of the reported OD cannot be validated, rendering it challenging to derive definitive conclusions.
Yang et al.27 and Cha et al.,16 reported that BL was notably greater with DAA, whereas Wang et al.22 reported increased BL with PA. Wang et al.,22 aimed to conduct a SR/MA exclusively of RCTs; however, they included Zhang et al.,28 a retrospective study, in their analysis of BL. Since retrospective studies provide lower quality evidence compared to RCTs, this inclusion introduced a methodological inconsistency that may have skewed their findings. In fact, Zhang et al.28 reported a MD of -163.69 (-177.89, -149.49), the largest effect size among all studies included in Wang et al.,22 with a 27.22% contribution to the pooled estimate. The inclusion of Zhang et al.28 significantly influenced the overall results reported by Wang et al.22 raising concerns about the validity of their conclusions. Therefore, these inconsistencies prevent a definitive conclusion about the superiority of one approach over the other in terms of BL. Another contributing factor to BL is that most surgeons perform a large anterior capsulectomy over a capsulotomy to gain access to the femur.29 However, capsulectomy may result in bleeding and create a persistent space for hematoma formation.29 Moreover, bleeding originating from the femoral side can obscure the posterior capsule view and complicate the management of bleeding during the release of the posteriorly located soft tissues.29
Both the longer OD and the greater BL observed in DAA can potentially be attributed to the steep learning curve for DAA which is a relatively newer approach than PA.30
In our analysis, three SRs/MAs15,17,19 established that PA was associated with a longer LOS compared to DAA. The quicker recovery and earlier discharge from the hospital after surgery may be attributed to DAA technique, which inflicts minimal damage to muscles, thereby facilitating rapid progression in walking training.31
PROMs serve as a foundational element for both surgeons and patients when determining the preferred surgical approach. Our data indicates that DAA is associated with lower VAS compared to PA, however this superiority is short-term and was only observed at POD1 and POD2 after which, there were no significant differences in VAS at POW2, POW6 or POM12.
Observed trends in HHS for evaluating hip function indicated that patients who underwent THA via DAA exhibited significantly improved hip functionality at POW2 and POW6 compared to those who underwent THA via PA. However, like VAS, the advantage of DAA over PA was not maintained over time with HHS differences becoming statistically insignificant at POM3, POM6 and POM12.
Early favourable outcomes associated with DAA can be ascribed to its less invasive nature.11 DAA is performed through an intermuscular plane between the sartorius, rectus femoris, and tensor fasciae latae muscles, preserving muscular integrity, avoiding trauma to the posterior capsule, and maintaining external rotation.11 However, PA involves blunt dissection through the gluteus maximus and cutting the lateral rotator muscle group, which may result in tissue damage.11
Strengths and Limitations
Pollock et al.32 highlighted the methodological challenges in overviews of SRs/MAs, including the risk of “double counting” due to overlapping studies. To address this, a common approach is to select either the most recent SR/MAs or a Cochrane Group study when faced with multiple choices.32 In our review, we evaluated the overlap among SRs/MAs without merging their results to avoid potential bias.
Our findings are limited by the available literature, with only two SRs/MAs11,23 defining DAA and PA, complicating RCT selection. Of the 11 SR/MAs11,14–23 examined, two were “low”19,23 and nine “critically low” quality,11,14–18,20–22 affecting results interpretation. It is important to note that the rating was done according to AMSTAR-2 domains, which assess the methodological quality and reporting of systematic reviews and meta-analyses, rather than the quality of the conclusions they reached. Despite being related, a methodologically weak study does not necessarily falsify its conclusion but it does lower the level of evidence supporting the conclusion. Key methodological steps, such as stating the reason for including RCTs (domain 3), providing a list of excluded studies (domain 7), and reporting on sources of funding (domain 10) would have improved their quality in terms of the AMSTAR-2 but their absence will not affect the conclusion and validity of the results reported.
Moreover, discrepancies may arise from human error; however, verifying individual trial data or assessing the influence of learning curves and practitioner experience was outside the scope of our review.
This review is the first to compare DAA and PA through SRs/MAs of RCTs, addressing a highly debated topic. Through detailed quality assessments and the creation of matrices to analyse SRs/MAs, we have deepened our understanding of the available evidence and its variances, setting the stage for further studies.
Conclusion
This umbrella review showed that, although there are insignificant differences in complications and prosthetic alignment between DAA and PA, DAA is associated with significantly less early postoperative pain and better early hip functionality. The advantage of DAA lies in its muscle-and soft tissue-sparing technique, leading to positive patient-reported outcome measures and potential cost savings. Evidence comparing the superiority of surgical approaches is limited by the variability and inconsistencies in SRs/MAs. Decision-making regarding the choice of approach must account for the surgeon’s clinical training, expertise, and the patient’s clinical profile. Recognizing the inherent advantages and limitations of surgical approaches, we recommend that surgeons maintain adherence to the approach they have diligently trained and practiced over years while continually refining their techniques to optimize patient outcomes. To resolve this controversy, future research should focus on clearly defining the different surgical approaches in order to prevent misinterpretation and to accurately assess the impact of surgical expertise on THA outcomes
Correspondence
Mohamad Nassereddine (mn103@aub.edu.lb)
Division of Orthopaedic Surgery, Department of Surgery
American University of Beirut Medical Center
Medical Center, Beirut, Lebanon
Cairo Street, Hamra, Beirut 1107 2020, Lebanon
Telephone number: +961 1 350000 (ext 5444)
Fax: +961-1363291
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Author Contributions
JN and LA conceptualized the study design, developed the protocol, performed the search strategy, extracted and analyzed data, and prepared the manuscript draft. MiM and MaM contributed to the search strategy, extracted analyzed data, and prepared the manuscript draft. MH contributed to the search strategy, extracted data, and helped in revision of final manuscript.
MN supported study conceptualization provided methodological support and expertise, and study oversight. All authors read and approved the final manuscript.
Acknowledgements
We would like to thank Dr. Ola El-Zein, senior medical librarian at the American University of Beirut, who has provided advice for the search strategy.
Protocol Registration
PROSPERO (CRD42023450069)
Provenance and peer review
Not commissioned, externally peer-reviewed.