

Introduction
Total hip arthroplasty (THA) is one of the most successful and cost-effective orthopaedic interventions, with more than one million procedures performed annually worldwide.1,2 It is even acclaimed as the ‘operation of the century’ for its ability to provide pain relief, restore mobility and improve overall quality of life.2 THA’s have an implant survivorship of 95% at 10-years, and significantly a survivorship of 58% at 25-years- indicating prolonged longevity of implants.1,3–6
Currently, the annual number of THAs performed is predicted to increase approximately 176% by the year 2040 and by as much as 659% by the year 2060 in the United States of America (USA) alone.7–9 In keeping with these increases, the number of revision THA’s is also increasing, with an overall revision rate of 6.8% at 13-years according to the National Joint Registry of the United Kingdom.10 Unfortunately, despite advances in both surgical techniques and implant designs, periprosthetic joint infection (PJI) remains one of the commonest and most devastating causes of failure following THA; accounting for 13-17% of all primary THA revisions.5,10–12
PJIs are associated with significant morbidity and mortality (Figure 1).13 They place a significant multifactorial burden on patients, relating to loss of mobility secondary to diminished limb function and prolonged hospital stays, which eventually leads to severe physical, emotional and psychological distress.14,15 Sadly, its burden isn’t isolated to the patient alone but rather extends to the caregivers, surgeons, hospitals, health systems and economies.15 Currently, the annual rate of PJIs is anticipated to rise concurrently with the increase in the number of THA performed. PJIs must be addressed due to their substantial clinical and economic implications, with anticipated direct costs estimated to be in excess of $46,000 in developed countries.14

This review will explore and highlight the dramatic and devastating consequences of this post-operative complication. These constitute the disconcerting and profound consequences of PJI including the deleterious impact on implant survivorship, functional and clinical outcomes, financial burden, mortality rate and psychological effects. These will be emphasised as they are important concepts for all surgeons performing THA. By placing the spotlight on PJI the authors aspire to reinvigorate better prevention strategies, promote better multi-disciplinary co-operation, inspire improved theatre etiquette, enhanced patient pre-operative
Methods
This review provides an evaluation of the published literature regarding PJI and its impact on patients, treating orthopaedic surgeons and economies. Publications relating to this subject were identified using different electronic resources, including PubMed, Scopus, and Google Scholar. The keywords used included ‘‘periprosthetic joint infection’’, ''total joint arthroplasty" “cost”, “burden” and ‘‘litigation’’. This identified 277 published papers. Additionally, studies written in languages other than English, reports not dealing with total hip or total knee arthroplasties, papers with the wrong subject matter, and duplications were excluded.
Incidence of PJI
PJI remains a major concern following THA with the present incidence ranging from 0.5% - 2.3% based on existing literature and joint registries.11,16–20 Overall, PJI is the 3rd leading cause of primary implant failure following THA and is the principal cause of early primary THA failure, i.e. within 2 years following surgery.10,20–23 Additionally, when comparing all major joint registries infection still ranks as one of the five commonest indications for revision surgery.24 In revision THA, PJI is the most common cause of failure accounting for 30.2% of all revisions.25 This rate is projected to rise over the next 15 years and predicted to account for up to 60% of all revision failures.16,18
Over the next few decades, the incidence of PJI is anticipated to increase secondary to ageing populations and changing characteristics of patients requiring THA, such as rates of obesity.14 The changing physiological characteristics and presence of concomitant comorbidities is further supported by data from the National Joint Registry for England and Wales. They reported that between 2010 and 2018, the number of patients reported as American Society of Anaesthesiologists (ASA) Class 1 (i.e. healthy) decreased from 16% to 12%. Reciprocally, during that same period, the number of patients classified as ASA Class 3 (i.e. incapacitating systemic disease) increased from 15% to 20%.24,26
The Burden and Impact on patients
Mortality in THA PJI
Mortality rates in PJI subsequent to a primary THA range from 4 – 8% after one year.27–29 Natsuhara et al.29 in their systematic review of 23 studies which included over 19,000 patients that underwent a two-stage revision for PJI reported a mortality rate of 4.22% and 21.12% at 1-year and 5-years respectively. Furthermore, Badarudeen et al.30 showed that 1-year mortality rate differed with different types of revision surgery. Patients who underwent a two-stage revision demonstrated a 1-year mortality of 5.8%, whilst a one-stage revision showed a higher mortality of 7%. Interestingly, after a debridement, antibiotics, irrigation and retention of implants (DAIR) procedure the 1-year mortality was highest at 10.4% in their series.30
When considering long-term outcomes, data from the Swedish hip arthroplasty registry indicated a 10-year all-cause mortality rate of 45% for patients with a PJI following THA, compared to the 29% in the non-PJI THA group.14,31 Additionally, Xu et al.14 conducted a systematic review in which they compared nine studies evaluating mortality rates between patients with PJI managed either surgically or medically. It demonstrated that PJI had a mortality risk at 1-year of 2.18 compared to primary arthroplasty.14
As previously established, the ASA Class may be used to indicate presence of comorbidities.31 Interestingly, ASA Class 1 and 2 are the only ASA Classes whose mortality risk is affected by PJI. This is explained Murray and colleagues32 who report that a new chronic disease has a greater influence on mortality in a previously healthy individual than those with preexisting comorbidities i.e. ASA Class 3 and 4. In patients with PJI, hip function and mobility is compromised; this precipitously increases chronic diseases due to decreased physical activity in previously healthy individuals and therefore influences mortality risk.31
Kurtz et al.33 in their retrospective cohort review, contextualised the significant mortality risk these patients face by comparing the overall survival at 5-years of Medicare patients with PJI to patients diagnosed with breast or prostate cancer (the 2 commonest cancers globally). The 5-year survival was reported to be 73% and 79% for female breast and male prostate cancer respectively. While the 5-year survival of for PJI after THA was found to be lower, at 67% in their cohort. Additionally, Zmistowski et al.34 compared survival rates at five years for PJI versus common cancers. They found that PJI had the lowest survival rate (87.3%) compared to prostate cancer (99%), breast cancer (89%), and melanoma (91%).34
Complications of revision THA for PJI
Following a primary THA, the rate of major complications occurring within 90 days is 1 – 3%, these include venous thromboembolism (VTE), wound infection, hospital readmission, dislocation and death.35 In revision THA, Koenig et al.35 reported the risk of major complications within 90 days in patients over 80 years to be 34% and for in patients aged 65-79 years to be 19%. In revision THA for PJI, patients are faced with a 10% higher rate of developing any complication compared to aseptic revision.36
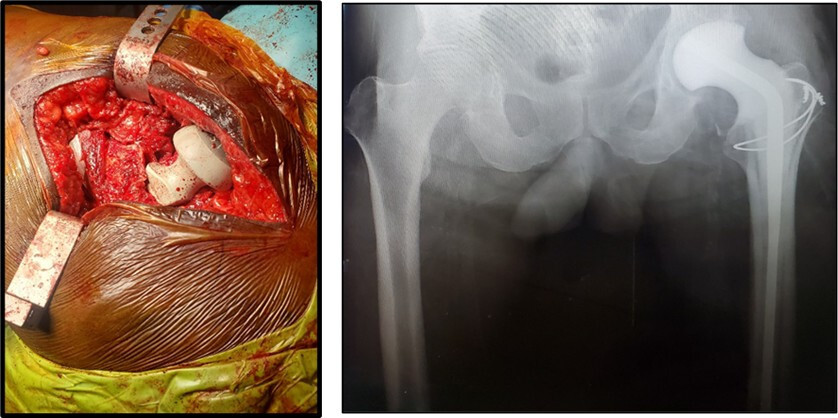
The commonest treatment for chronic PJI following THA remains a two-stage revision arthroplasty (Figure 2 and 3).37 Li et al.37 found 38% of patients undergoing two-stage revision treatment for PJIs will suffer at least one major complication during the period between the first and second stage surgery. Moreover, the median time to the first complication was noted to be 2.3 months. Twenty five percent of these complications are attributed to medical deterioration including VTE. Whereas approximately 60% are wound related complications or an ongoing infection requiring reoperation.37 Considering all these factors, it is therefore unsurprising that only 60 - 77% of patients are even able to undergo the second stage of a planned two-stage reimplantation.38

._post-opera.jpeg)
Health, Functional and Psychological impact
Patients with PJI after THA will experience inferior hip function and lower median Oxford hip scores compared to control groups.31 A systematic review by Rietbergen et al.39 revealed a 12 – 25% lower health related quality of life (HRQoL) questionnaire scores in patients undergoing 2-stage revision treatment for PJI in THA when compared to the general population. Different HRQoL also influence the patient-reported outcomes, further complicating comparison between studies.14 A registry review of the Swedish Hip Arthroplasty Registry demonstrated that the greatest difference between PJI patients relative to the control group was the decrease in mobility.31 Stating as many as 50% of PJI patients reported major functional deficit.31
Medical and surgical complications and financial implications following PJI often receive significant attention in literature.40 Unfortunately, the psychological sequelae following PJI remains a topic inadequately investigated. The psychological anguish these patients face is related to a multitude of stressors including physical and financial distress and losses. For instance, patients with PJI have persistent pain; this chronic pain may manifest psychologically as either depression or anxiety.40 Wilson et al.40 demonstrated this showing that patients with PJI have higher odds of developing new onset depression (NOD) compared to primary THA (odds ratio = 1.82).40,41 Additionally, they demonstrated that presence of pre-operative anxiety is the strongest predictor of post-operative NOD.40
Approximately 58% of patients report depressive symptoms throughout treatment and 21.9% continue to have symptoms at 5 years following PJI eradication.42,43 PJI patients are twice as likely to identify as disabled with 20% being unable to climb stairs. While 40% will report having a worse physical health and up to 80% of patients expressing a need for additional psychological support.43,44 Sadly, 1 in every 5 patients who develop PJI will regret undergoing their initial THA.43
The survivorship & success of treatment
In a retrospective review of 369 hips treated for PJI with revision THA, at a single high-volume Centre, Liukonnen et al.45 showed that 1 in 5 patients required re-operation within 1 year of revision THA. The rate of failure of early PJI treated surgically was noted to be 37% whilst surgical intervention for chronic PJI was approximately 26.8% at 1-year follow-up. Also, they found that performing one-stage revision over a DAIR for early infections halved the incidence of further surgical interventions while having the same 1-year mortality rate.45
The reported success of two-stage revision for PJI after THA varies from 52%–78%.37 Van Dijk et al.46 showed an 83% infection control rate after a 2-stage revision procedure at 4 years following treatment. In a long-term registry review, reviewing the Swedish hip arthroplasty registry, Svensson et al.47 reported a survivorship of 72-75% after single or two stage revision for PJI at the 15-year mark, with no significant difference between either treatment.
A recent systematic review showed the reinfection rate after either single or two stage revision for PJI ranges from 5.7- 8.2%.48 Treatment for re-infection with a repeat two-stage revision THA has a further reduced implant survivorship of 74% after 2 years and only 45% after 5 years.49 Along with a reduced survivorship, repeat two stage revision for re-infection results in a further increase in mortality risk where one third of patients will be deceased within 2 years following treatment.50
The economic burden of PJI after THA
Economic considerations
Economic costs related to treatment of PJI remain high. This is related to a multitude of factors including prolonged hospitalizations, requirement for revision of the implant and poor RTW.51 In the USA, the annual number of PJIs in THA during 2002 was 5,075 which increased to 8,635 and 11,985 in 2012 and 2017 respectively. Total annual cost increased from $166.6 million to $384.7 million over the same 15-year period.52 The current estimated lifetime economic cost of treatment for a 65-year-old patient with a PJU is approximately $390,806.53,54 The total annual hospital costs are estimated to rise to $753.4 million by the year 2030.52
Patel et al.55 compared the relationship between case difficulty and relative value units (RVU) compensation in primary and revision arthroplasty. When compared to the primary THA, every revision type, except for modular component head/liner exchange, reimbursed less per minute and less per RVU.55 Emphasising the importance and value of ensuring that primary THA never reaches PJI. Furthermore, Quan et al.56 showed when comparing RVU per minute between aseptic and septic revision THA, septic revision THA cases were valued less at $7.65 per minute compared to aseptic revision THA at $9.28. Moreover, Feng et al.57 demonstrated that in the current financial model in the USA, revision hip surgeons can potentially lose 26-55% RVU per day when compared to surgeons only performing primary THA.
Hospital costs
The treatment of PJI in THA is estimated to be 3 – 5.6 times more costly than primary THA resulting in a substantial economic impact and burden.11,17,52,53,58 On average THA PJI costs $62,964 more than an uncomplicated primary THA, wherein 83% of this total cost results from the combined hospital bed, operating room and implant expenses.58–60 This results in a 2.3 times longer hospital stay and double the readmission rate compared to an uncomplicated primary THA.58,59 Additionally, outpatient follow-up visits increase from 3.8 visits in uncomplicated primary THA to 9.2 visits in patients with PJI’s.59
Kapadia et al.58 showed increased hospital costs were incurred across multiple areas during the treatment of PJIs. These included a 3.7 times higher admission cost, 4.5 times higher hospital bed, 2.5 times higher operating room and anaesthesia services cost, and 24 times increase in multidisciplinary speciality consultation costs compared to uncomplicated cases.58 PJI caused by methicillin-resistant Staphylococcus Aureus or Enterococcus species further leads to a 1.5 – 2 times higher total cost, mean length of stay and mortality rate when compared to patients with THA PJI caused by other organisms.27,58,61
Overall, the cost of revision THA for PJI is high and incurs a 3.6 times higher cost when compared to primary THA. This is more than double the cost of revision THA for non-infected cases, which itself is 1.4 times more costly than primary THA.62
Return to work after treatment
PJI’s negatively impacts on a patient’s capacity to work and conduct everyday activities.63 Unfortunately, there is a paucity of evidence regarding return to work (RTW) following PJI. Scott et al.64 noted that of their patient cohort that was < 65 years old and working previously, only 33% of patients returned to work following revision surgery. Factors that most profoundly impacted on RTW were age, early failure of the primary implant and the post-operative Oxford Hip Score.64 The factor that had the greatest impact on RTW was the patient’s age, where only 20% of patients >60 years of age returned to work. Additionally, no patients returned to moderate or heavy manual labour following revision surgery.64
Impact on Orthopaedic surgeons
A scarcity of quantitative data exists regarding the psychological impact of PJI on the treating Orthopaedic and Arthroplasty Surgeon. Svensson et al.65 identified various challenges surgeons face in the management of patients with PJI, that often lead to subjective psychological stress. These begin with difficulties in the diagnosis of PJI after THA, that result in the surgeons experiencing incompetence, insecurity and frustration. Over 90% of surgeons cited experiencing grief, along with the various stages including guilt and occasionally denial.65
Despite counselling about the possibility of complications prior to primary THA, patients do not expect that they’ll develop a PJI. And once a PJI develops patients and their relatives often lay the blame on the orthopaedic surgeon. Frequent requests for transfer or referral to other care facilities by patients amplify the feeling of fault, woe and disappointment experienced by orthopaedic surgeons.65 Suggestions to improve this involve establishing a multidisciplinary team including orthopaedic surgeons of different experience, allied health care services such as psychologists and infectious disease physicians. Standardising PJI management protocols, creating specialised units and having scheduled times for surgeon counselling is recommended.65,66
Litigation in PJI
It is estimated over 80% of adult arthroplasty surgeons are likely to be affected by medical malpractice lawsuits during their careers, one of the highest of the orthopaedic subspecialties.67,68 Overall, Kheir et al.67 found that 22 - 25% of allegations post total joint arthroplasty were related to PJI. THA accounts for 11% of all orthopaedic related claims and 10% of the overall cost of orthopaedic related claims against the United Kingdom’s National Health Services. Over a 15-year period, there were 1,004 litigation claims involving THA across the UK that totalled over £41.5 million. Of these 11.5% were related to PJI- a 3% higher number of claims compared to those related to a leg length discrepancy post-THA and just below the percentage of claims due to iatrogenic neurological injuries. The average claimant’s pay-out for each of these cases of PJI post THA amounted to approximately £138,600.69
In 2019, Senard and colleagues70 conducted retrospective review of PJI claims with a major French medical liability-specialized insurance company. They observed that a high proportion (51%) of the litigation involved early cases of infection i.e. < 1 month.70 Additionally, they determined the 3 commonest causes of poor management in PJI included a delay in diagnosis, inadequate antibiotic therapy and poor surgical treatment.70 Furthermore, the recommendation was made that an infectious disease (ID) specialist be consulted early in treatment, as they discovered that ID advice was sought very late, in as many as 24% of cases.70
Conclusion
Whilst, PJI remains an uncommon complication of THA, its increasing incidence will emulate the rising number of primary THAs being performed each year. The magnitude of the impact on patients, orthopaedic surgeons, hospitals, society and economies renders PJI in THA the most devastating complication. Establishing multi-disciplinary teams for holistic patient care together with continued research and innovation are essential to optimize THA outcomes and subsequently reduce the risk of PJIs. Therefore, it is quintessential that every orthopaedic and arthroplasty surgeon remains mindful of the burden caused by this complication and every effort be undertaken to reduce the risk of PJI in THA.
Authors’ contributions
Mohammad H.S. Aftab: literature review, writing original draft, editing manuscript
Troye Joseph: literature review, writing original draft
Richard Almeida: manuscript reviewing and editing, supervision
Nkhodiseni Sikhauli: manuscript reviewing and editing, supervision
Jurek R.T. Pietrzak: conceptualization, literature review, writing original draft, supervision
Conflict of interests
The authors declare that they have no conflict of interests
Funding
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.