INTRODUCTION
Shoulder pain has been and remains one of the most frequently reported musculoskeletal issues, ranking third among complaints in orthopedic clinics.1 Shoulder impingement syndrome (SIS), defined as pathologies related to narrowing of the subacromial space, comprise a majority of shoulder pain clinic visits.2,3 Causes of SIS can be subdivided into intrinsic and extrinsic causes, with intrinsic causes being due to chronic usage and tendon degeneration, while extrinsic causes being due to anatomical variations and subacromial bursa inflammation.4 Physicians typically interchange SIS with other terms such as subacromial impingement syndrome and rotator cuff impingement. SIS are more commonly found in individuals whose profession involves strenuous overhead physical activity or those involved in athletics with heavy swinging motions.5
Non-surgical intervention for less severe cases of shoulder impingement includes anti-inflammatory medication and specialized physical therapy aimed towards improving strength of the rotator cuff.6–8 However, in situations where SIS does not improve through non-operative means, an acromioplasty can be performed, which, as originally described by Neer in 1972, is the removal of the anterior end and undersurface of the acromion, along with the associated coracoacromial ligament.9 Since the introduction of the technique, there have been many surgical modifications and alterations to the technique, though the main objective remains to alter the acromion to relieve impingement due to compression.10 The procedure was initially performed as an open procedure, but after the introduction of the arthroscopic approach by Ellman in 1987, it has overwhelmingly shifted to an arthroscopic technique.11,12
This systematic review provides a summary of the literature over time to show how continued research, surgical innovation, and patient reported outcomes can drive a shift in the standard of a surgical technique. The study aims to synthesize the literature on patients who underwent either arthroscopic or open acromioplasty and evaluate whether one approach demonstrates superior outcomes, validating the current preferences for arthroscopic procedures in modern surgical practice. Several patient orientated parameters will be analyzed, including return-to-activity, surgical parameters, patient satisfaction rating, and UCLA shoulder score. It is hypothesized that the evidence will show that the arthroscopic technique is superior to the open with regard to patient outcomes and thus is the reason that arthroscopic acromioplasty is most commonly performed today.
MATERIALS AND METHODS
Database Query For Relevant Literature
Peer-reviewed literature was searched up until October 7th, 2024, using the databases Pubmed/Medline, Embase (Ovid), Web of Science, and Cochrane. Relevant search terms were selectively chosen and combined to retrieve articles pertinent to the study of interest. The search terms related to the procedure (e.g. open acromioplasty, arthroscopic acromioplasty, open subacromial decompression, arthroscopic subacromial decompression) were combined with the injury mechanism (e.g. shoulder impingement, rotator cuff impingement, subacromial syndrome, shoulder blade impingement) to identify studies that analyzed certain measures related to patient outcome (e.g. outcomes, range of motion, recurrence, complications, satisfaction, effectiveness, follow-up). The specific searches used for each database can be found in Tables A.1, A.2, A.3, and A.4 of the appendix. Relevant studies were subsequently gathered in Covidence for screening and data extraction. This systematic review was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting standards.
Literature Screening and Eligibility Criteria
All studies exported to Covidence were screened for certain eligibility criteria along with relevance to the study of interest. In terms of study relevance, we selectively screened for articles comparing arthroscopic or open acromioplasty. The study designs included case series, prospective and retrospective cohorts, and randomized controlled trials, focusing on outcomes like patient recovery, range of motion, and complication rates. Papers identified as case reports, systematic reviews, technique papers, editorials, or conference presentations, as well as studies on cadavers, animals, biomechanics, non-English papers, and unavailable studies were excluded. Our studies underwent two rounds of screening, an initial title and abstract screening, followed by full-text review, both following the same eligibility criteria. Screening was conducted by A.K.C. and S.S., with conflicts resolved by a third reviewer, S.R.V.
Risk of Bias Assessment
To evaluate the methodological and evidential strength of the research articles, JBI’s Critical Appraisal Tool for cohort studies was used to determine the risk of bias. The assessment was conducted by A.K.C. and S.S., with discrepancies resolved by a third reviewer, S.R.V.
Data Extraction From Literature
All articles that passed screening underwent thorough data extraction focusing on key measurements such as study type, level of evidence, surgical technique, indications, patient count, sex, average age, functional outcomes, and patient-reported outcomes. Only patients who were available for follow-up were included. Data extraction was independently conducted by A.K.C. and S.S., with a second round of verification to ensure accuracy.
Analysis of Data From Extracted Articles
The articles analyzed were methodologically and clinically variable, with heterogeneous outcome measurements. Therefore, a meta-analysis was not performed and instead, measurements were concisely summarized into two tables: clinical and functional outcomes (Table 2) and patient-reported outcomes (Table 3). Table 2 includes return-to-activity/return-to-sports (RTA/RTS), surgical outcomes, range of motion, and muscle strength, while Table 3 covers patient satisfaction rating, UCLA shoulder score, Constant score, and others.
RESULTS
Database Filtering and Screening Information
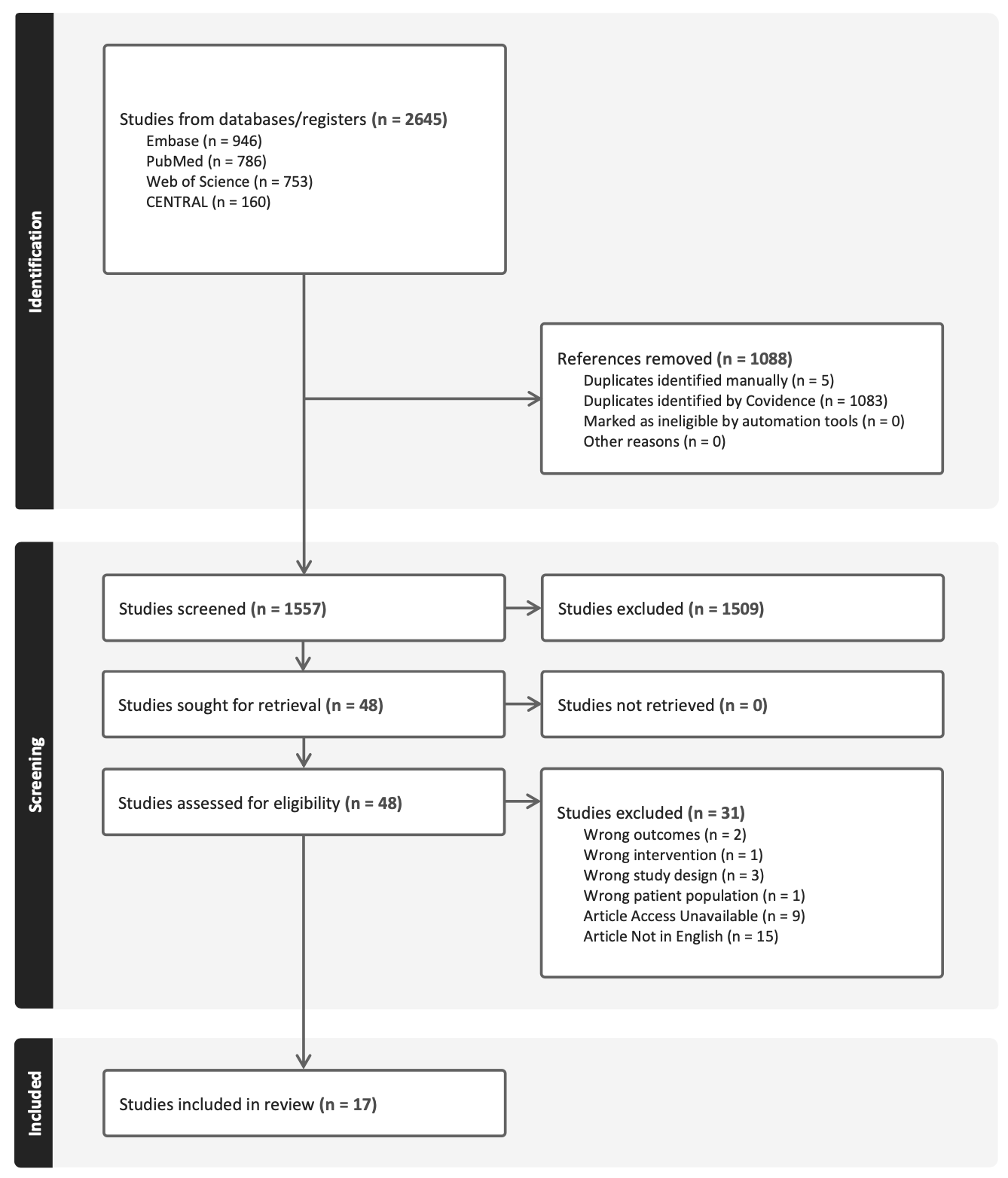
An initial search of multiple databases utilizing key search terms yielded a combined total of 2,645 articles, which after being filtered for duplicates, resulted in 1,557 articles progressing towards title and abstract screening. Based on inclusion and exclusion criteria, 48 articles were subsequently screened for full-text evaluation. Thirty-one articles were then excluded due to incorrect outcomes (n=2), interventions (n=1), study design (n=3), patient population (n=1), if unavailable (n=9), or not in English (n=15). Final data extraction was conducted on 17 articles for this systematic review.

Quality Assessment According to Risk of Bias
Risk of Bias assessment for quality control was conducted by A.K.C. and S.S. according to the JBI Critical Appraisal Tools for cohort studies, leading to an average score of 10.2/11.13–29 After appraisal, all 17 studies were considered eligible for further data extraction and analysis.
Patient Demographics Throughout Literature
Throughout the 17 studies analyzed, a total of 1,293 patients underwent open or arthroscopic acromioplasty, with postoperative follow-up data collected (Table 1). The patient population consisted of 763 males and 530 females, with a weighted age of 45.4 years. The patients had various shoulder impingement syndromes, such as rotator-cuff impingement. These chronic conditions were typically unresponsive to nonoperative treatment.
Functional Outcomes Following Acromioplasty
Across the studies, a number of functional outcomes, including return-to-activity/sport, surgical outcomes, range of motion, and muscle strength, were recorded for patients after undergoing arthroscopic or open acromioplasty and summarized in Table 2.
Return-to-activity/Return-to-sports
Post-operative recovery from arthroscopic and open acromioplasty demonstrated slight differences in timing for return-to-activity and return-to-sports timing. VanHolsbeeck et al. reported a 9-week recovery for arthroscopic procedures compared to 11.6-weeks for open procedures.18 Another study found the arthroscopic group averaged 5.7 weeks compared to 10 weeks of open procedures.29 Further analysis of arthroscopic acromioplasty patients revealed a 67% RTS, with 33% unable to maintain the preoperative strength for throwing activities.23
Surgical Outcomes
In a study by Spangehl et al., postoperative surgical outcomes were measured for patients undergoing either arthroscopic or open acromioplasty.17 A similar number of patients experienced postoperative stiffness, four from the arthroscopic group and three from the open group. Five patients from the arthroscopic group eventually underwent open acromioplasty due to the persistent symptoms. Another study reported keloid scar formation in 2% of shoulders at portal sites.20
Operative times varied between studies. Odenbring et al. found a significant difference between procedures, with arthroscopic acromioplasty averaging 45 minutes and open acromioplasty averaging 57 minutes.24 Conversely, another study showed arthroscopic procedures averaged 82 minutes while open procedures averaged 52 minutes.29 Schröder et al. compared arthroscopic operation time based on surgeon expertise, categorizing surgeons as beginner, some experience, or experienced, with open acromioplasty as the comparator group.26 Average operative time was 53 minutes, 50 minutes, 38 minutes, and 55 minutes respectively. Experienced arthroscopic acromioplasty surgeons had significantly shorter operative times compared to those performing open acromioplasty. Hospital stay was 2.3, 1.9, 1.3, and 5.5 days, respectively, with all arthroscopic patients having significantly shorter hospital stays than the open group.
Range of Motion
In one study, active forward flexion was assessed and showed that arthroscopic and open procedures improved flexion ability post-operatively.18 Preoperative active forward flexion score for the arthroscopic group improved from 3.7 to 4.8, while the open group improved from 3.2 to 4.6. A similar study studied active elevation, with the open group changing from 150° to 157°, and the arthroscopic group changing from 140° to 157° at follow up.22 Complications related to range of motion included two patients who developed frozen shoulders after arthroscopic acromioplasty. In the open acromioplasty group, two patients developed superficial wound infections, one developed a hematoma, and three developed frozen shoulders.26
Muscle Strength
For the arthroscopic group, the mean strength score of the anterior deltoid improved from 13.7 to 16.9 post-operatively, comparable to the open group, which showed an improvement of 13.4 to 15.6.17 Additionally, the average strength score for forward flexion was improved similarly in both groups, with the arthroscopic group improving from 3.8 to 4.7 and the open group improving from 3.5 to 4.5. Another study monitoring elevation strength showed a significant improvement in the open group from 9.0 to 14.4, whereas the arthroscopic group had a nonsignificant improvement from 11.6 to 14.0. However, there was no significant difference in final strength between the two groups.21 Isokinetic muscle testing for external rotation at 96 months postoperatively revealed that the arthroscopic group had a score of 149, compared to 128 for the open group.29
Patient Reported Statistics
After undergoing treatment for their shoulder impingement syndromes, studies recorded several patient-reported outcomes to evaluate treatment effectiveness (Table 3). Primary measurements included: patient satisfaction rating, UCLA shoulder score, constant score, DASH score, OSS score, and pain score.
Patient Satisfaction Rating
In comparing patient satisfaction levels postoperatively, Spangehl et al. categorized their data in three groups: satisfied, somewhat satisfied, and not satisfied.17 The arthroscopic group had 16, 12, and 4 patients respectively, while the open group had 16, 10, and 4 patients respectively. Similar satisfaction rates were observed in other studies, with one study reporting that 88.3% of arthroscopic group patients were satisfied with their procedures compared to 94.3% in the open group.18 In an eight-year follow-up, patients that underwent arthroscopic acromioplasty reported a satisfaction rate of 95/100 compared to 93/100 for those who had open acromioplasty.29 However, Schröder et al. found a distinct difference between the two groups, with the arthroscopic group having 82% patients reporting excellent or good outcomes, compared to 68% in the open group.26
UCLA Shoulder Score
To functionally quantify shoulder outcomes, several studies used the UCLA shoulder score clinical scale. Nutton et al. evaluated patients who developed a UCLA shoulder score above 27 before arthroscopic subacromial decompression, 3 months postoperatively, 6 months postoperatively, and 1 year postoperatively, finding scores of 0%, 39%, 71%, and 85% respectively.14 Two studies compared UCLA shoulder scores and reportedly had similar score distributions between the arthroscopic and open acromioplasty groups.17,18 Additionally, Husby et al. showed that, eight years postoperatively, UCLA scores identical (32) for both groups.29 However, two other studies comparing the same procedures showed significantly higher mean UCLA scores for the arthroscopic group. Odenbring et al. reported an average score of 32.1 for the arthroscopic group and 27.8 for the open group, while T’Jonck et al. showed an average of 28.3 and 24.5 respectively.24,25
Constant Score
To measure shoulder function and pain levels, patients were evaluated using the clinical Constant score. When comparing pre- to postoperative scores, the arthroscopic group showed a significant improvement from 54.3 to 74.7, similar to the open group which significantly improved from 48.6 to 80.3.21 These results were consistent with another study, where the arthroscopic group improved from 56 to 66, and the open group improved from 48 to 73.22 However, T’Jonck et al. reported a constant score of 80.8 for the arthroscopic group compared to 73.8 for the open group, although the data was not statistically significant.25
Other Measurements
To quantify disability of patients before and after surgery, Bengtsson et al. showed a significant decrease in DASH score after arthroscopic acromioplasty from 42 preoperatively to 18 six-months postoperatively.13 Another study comparing arthroscopic to open acromioplasty found no significant difference in DASH scores between the groups, with scores of 24 and 29 respectively.24 Mean OSS scores were also measured in a study evaluating arthroscopic subacromial decompression, showing a significant improvement from 18 preoperatively to 38 three months postoperatively.15 Additionally, a study measuring mean pain score ADLs in patients who underwent open acromioplasty found a pain score of 10.5/15 for involved shoulders, compared to 15/15 for the unaffected shoulders.16
DISCUSSION
This review sought to synthesize the evidence comparing open versus arthroscopic acromioplasty while also incorporating the historical perspective to provide a comprehensive analysis of the evolution of the preferred surgical treatment for shoulder impingement syndrome. It is through the development of arthroscopy, research, patient data collection, and innovation that arthroscopic acromioplasty is most commonly performed today.
Postoperative return-to-activity and return-to-sports are key indicators of patient recovery time and ability to regain functionality. The included literature demonstrated that, on average, patients who underwent arthroscopic acromioplasty (average 5.7 weeks) had a multiple week quicker return-to-activity compared to those who underwent the open procedure (average 10 weeks). These findings may be attributed to the minimally invasive nature of arthroscopy, resulting in less tissue trauma, faster wound closure time, and reduced local inflammation.30 A shorter length of stay for the arthroscopic group, although based on limited data from a 2001 study, supports these findings.
Operative time, an indicator of cost efficiency and potential increased risk of complications, showed mixed results across the studies. The level of experience likely plays a role in these variations, as efficient arthroscopy requires a specialized skill set. When surgeons were separated out by experience, Schröder et al. found that experienced surgeons were on average able to complete arthroscopic acromioplasty 17 minutes faster than open acromioplasty. Furthermore, Spangehl et al. showed that several patients who underwent arthroscopic acromioplasty later required reoperation with an open approach due to persistent symptoms, which may influence surgeons to prefer the open procedure in more severe cases.
As arthroscopy continues to be widely adopted in orthopedics, increased exposure and training have significantly enhanced surgeon proficiency.31 As surgeons transition towards arthroscopy at a higher volume, they demonstrate improved efficiency, shorter operation times, and lower complication rates over time, indicating that the initial learning curve is eventually overcome through surgical mastery. Furthermore, as surgeons gain familiarity with arthroscopic techniques, the shift toward predominantly choosing arthroscopy for certain procedures, such as acromioplasty, becomes increasingly justified, offering benefits such as improved patient outcomes and the ability to manage more complex cases arthroscopically.
Range of motion and muscle strength were both outcomes used to evaluate the effectiveness of each procedure in addressing the predominant manifestations of shoulder impingement syndromes. Range of motion improved in both surgical approaches to the same degree, as measured through active forward flexion score and active elevation. These results suggest that both procedures are similarly successful in treating the intended issue. Muscle strength improvements were also comparable between the two procedures, with similar improvements to mean anterior deltoid strength, forward flexion strength, and elevation strength postoperatively. However, arthroscopic acromioplasty showed a slight improvement to external rotation at 96 months postoperatively, suggesting a potential long-term advantage for arthroscopic procedures. Regardless, patient strength improved at a similar degree for most measured strength examinations, indicating that both types of acromioplasty are effective in treating shoulder impingement syndromes.
Regarding patient satisfaction, several studies showed that the proportion of patients who were satisfied or unsatisfied with their respective interventions was similar between the arthroscopic and open acromioplasty groups. However, Schröder et al. showed 14% higher satisfaction in the arthroscopic group compared to the open group, which may be attributed to reduced postoperative scarring or the surgeon’s expertise within this specific cohort. UCLA shoulder scores were similar across multiple studies. These findings were also shown in an eight-year follow up study, implying similar long-term satisfaction between the two groups. However, two studies indicated higher UCLA shoulder scores in the arthroscopic group, suggesting that some cohorts experienced improved long term outcomes with arthroscopic acromioplasty. In terms of Constant score, both groups showed similar improvements pre- and postoperatively, except for one study, which found a non-significantly higher constant score in the arthroscopic group. These findings indicate that arthroscopy may result in marginally improved shoulder functionality, though the evidence is limited and minimal clinically important differences were not analyzed in this review.
Several limitations must be considered when evaluating our findings. The heterogeneity of study design and outcome measurements could introduce variability, leading to compromised generalizability and consistency. Differences in how outcomes such as strength, pain, or range of motion are measured may further complicate comparisons between the surgical procedures. Additionally, variability in patient age and injury mechanisms across studies could influence recovery times and functional outcomes, making it challenging to draw definitive conclusions. Another key limitation is the variability in surgical technique and expertise. Studies have shown that success of arthroscopic acromioplasty is heavily dependent on the surgeon’s experience, and differences in skill level may skew findings. Confounding variables, such as comorbidities, rehabilitation procedures, or pre-existing shoulder conditions, may have also impacted recovery outcomes, and their influence may not have been adequately controlled for in each study.
Overall, this systematic review provides all the evidence to show the transition and evolution of the acromioplasty and how what was commonly performed open now is mostly done arthroscopic.
CONCLUSION
This systematic review summarizes the literature and displays how evidence and patient reported outcomes can shift a surgical technique. Arthroscopic acromioplasty offers superior return to activity/sport times, shorter hospital stays, and better cosmetic outcomes due to its minimally invasive nature. Through evidence and continued research, surgeon preference has shifted towards the arthroscopic acromioplasty over time, as it offers better recovery times and improved cosmetic results, making them a favored approach for shoulder impingement syndromes in patients and surgeons alike.
To whom correspondence should be addressed
Andrew K. Chow
Department of Orthopedic Surgery
Virginia Commonwealth University Medical Center
1200 E Broad St.
Richmond, VA 23298, USA
Tel: 917-912-1131
Email: chowak@vcu.edu