

Introduction
Due to its anatomical structure, multidirectional mobility, and excessive exposure to trauma, the glenohumeral joint represents the most frequently encountered major joint dislocation in emergency departments.1 Currently, shoulder dislocation cases constitute approximately half of all dislocation cases presenting to the emergency department. The most common mechanism of injury involves a fall onto an outstretched hand while the forearm is in extension, abduction, and external rotation.1,2 These dislocations are predominantly anterior, comprising 95% of cases. Shoulder dislocation is a pathology requiring urgent intervention. The primary goal of treatment is to restore a painless, fully functional, and stable joint.3 Two crucial considerations must be observed: first, avoiding excessive force during reduction to prevent fractures, and second, ensuring that no nerve damage occurs. The initial step in the reduction of a dislocated shoulder is to calm the patient, either through reassurance or pharmacological sedation.3,4 Acute shoulder dislocation should be reduced using one of the standard methods, with the most commonly employed being the Kocher and Hippocratic techniques.4 However, most of these classical techniques are partially painful and are associated with iatrogenic injuries, with the most frequently encountered being fractures of the proximal humerus and injuries to the brachial plexus, axillary nerve, and/or axillary artery.4,5
In this case series, we aimed to demonstrate that in four anterior shoulder dislocation cases where reduction attempts under emergency conditions were unsuccessful, the application of intramuscular analgesics and low-dose intramuscular sedatives, leading to the patient’s transition into natural sleep, allowed for spontaneous reduction of the shoulder joint within the first two hours without requiring anesthetic intervention or reduction maneuvers.
Case 1
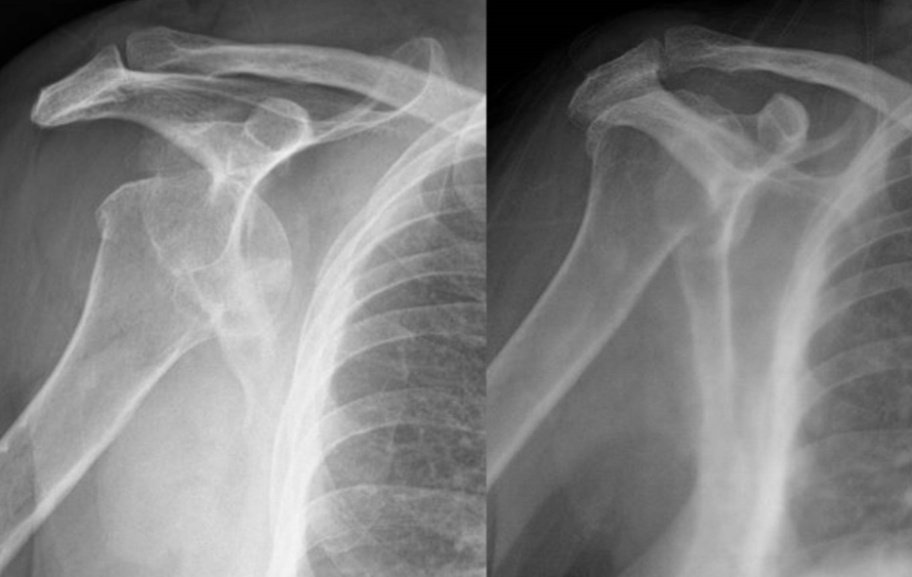
A 48-year-old male patient was brought to the emergency department following a fall. Shoulder radiography and computed tomography (CT) revealed a left anterior shoulder dislocation. Apart from the shoulder dislocation, no additional pathology or fracture was observed (Figure 1). The patient had no comorbidities and received only intramuscular analgesic (diclofenac sodium) under emergency conditions. Subsequently, reduction was attempted using the Hippocratic maneuver in the emergency unit, but this was unsuccessful. The patient was scheduled for reduction under anesthesia. The dislocated shoulder was immobilized with a Velpeau bandage, and the patient was admitted for emergency observation. During observation, in addition to analgesics, 5 mg of intramuscular diazepam was administered. The patient transitioned into natural sleep due to the medication, and upon waking one hour later, his pain had resolved. Control radiographs were requested, revealing that the shoulder joint had spontaneously reduced during natural sleep, negating the need for anesthetic intervention or reduction maneuvers. The patient was discharged with a Velpeau bandage.

Case 2
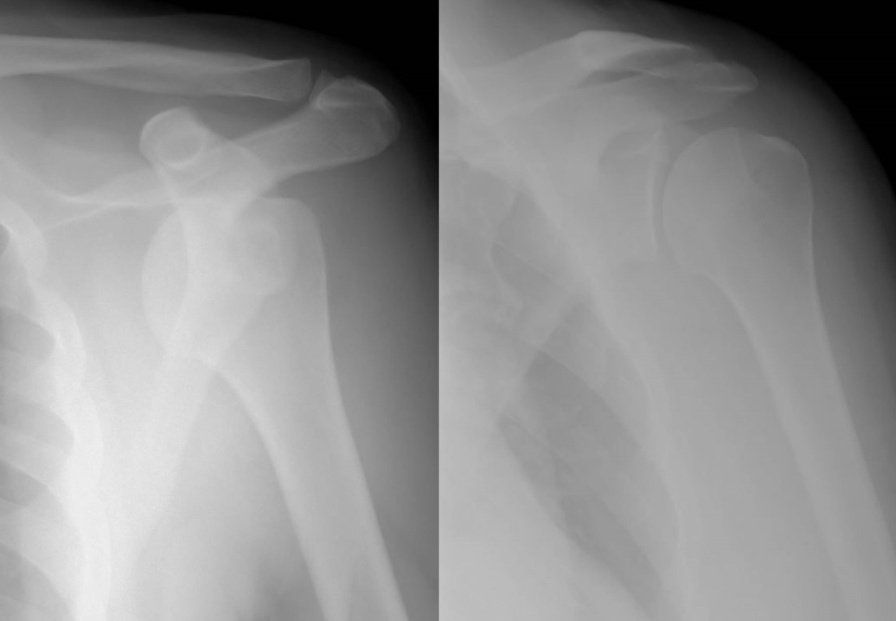
A 63-year-old female patient was brought to the emergency department following trauma. Shoulder radiography and CT imaging revealed a right anterior shoulder dislocation. No additional pathology or fractures were present aside from the shoulder dislocation (Figure 2). The patient had hypertension and diabetes and was administered only intramuscular analgesic (diclofenac sodium) under emergency conditions. Reduction was attempted using the Hippocratic maneuver in the emergency unit, but this was unsuccessful. The patient was scheduled for reduction under anesthesia. The shoulder was immobilized with a Velpeau bandage, and the patient was admitted for emergency observation. In addition to analgesics, 5 mg of intramuscular diazepam was administered. The patient transitioned into natural sleep due to the medication, and upon waking 45 minutes later, her pain had resolved. Control radiographs were requested, revealing that the shoulder joint had spontaneously reduced during natural sleep, making anesthetic intervention or reduction maneuvers unnecessary. The patient was discharged with a Velpeau bandage.

Case 3
A 60-year-old female patient was brought to the emergency department following an assault. Shoulder radiography and CT imaging revealed a right anterior shoulder dislocation (Figure 3). No additional pathology or fractures were present apart from the shoulder dislocation. The patient had hypertension and was administered only intramuscular analgesic (diclofenac sodium) under emergency conditions. Reduction was attempted using the Hippocratic maneuver in the emergency unit, but this was unsuccessful. The patient was scheduled for reduction under anesthesia. The shoulder was immobilized with a Velpeau bandage, and the patient was admitted for emergency observation. In addition to analgesics, 5 mg of intramuscular diazepam was administered. The patient transitioned into natural sleep due to the medication, and upon waking 90 minutes later, her pain had resolved. Control radiographs were requested, confirming that the shoulder joint had spontaneously reduced during natural sleep, eliminating the need for anesthetic intervention or reduction maneuvers. The patient was discharged with a Velpeau bandage.

Case 4
A 44-year-old male patient was brought to the emergency department following a motor vehicle accident. Shoulder radiography and CT imaging revealed a left anterior shoulder dislocation (Figure 4). No additional pathology or fractures were present apart from the shoulder dislocation. The patient had no comorbidities and received only intramuscular analgesic (diclofenac sodium) under emergency conditions. Reduction was attempted using the Hippocratic maneuver in the emergency unit, but this was unsuccessful. The patient was scheduled for reduction under anesthesia. The shoulder was immobilized with a Velpeau bandage, and the patient was admitted for emergency observation. In addition to analgesics, 5 mg of intramuscular diazepam was administered. The patient transitioned into natural sleep due to the medication, and upon waking 110 minutes later, his pain had resolved. Control radiographs were requested, revealing that the shoulder joint had spontaneously reduced during natural sleep, eliminating the need for anesthetic intervention or reduction maneuvers. The patient was discharged with a Velpeau bandage.

Discussion
Although anterior glenohumeral dislocations are frequently encountered in emergency departments, the reduction procedure can often be challenging. Standard practice involves an initial attempt at manual reduction with analgesia, followed by reduction under anesthesia and sedation if the initial attempt fails. The severe pain associated with shoulder dislocation increases muscle contractions in the shoulder region, which hinders reduction.5,6 Reduction methods represent different approaches to overcoming these identified obstacles. For shoulder joint reduction, the humeral head must move anteriorly and laterally or supralaterally. Normally, dynamic stabilizing forces keep the joint stable, but during dislocation, muscle spasms continue to pull on the humeral head and shaft. The spasms of the long head of the biceps and the subscapularis muscle are the primary dynamic forces preventing reduction of the humeral head. The long head of the biceps pulls the dislocated humeral head upward, anchoring it in the subcoracoid or glenoid region. During a spasm, this muscle resists anterior movement of the head and further restricts the repositioning of the humeral head by wrapping anterolaterally around its axis. The subscapularis muscle rotates the humerus inward and holds the head medially. The goal here is to reduce tension on the shoulder joint capsule, relieve the patient’s pain, and increase control over the joint as spasm subsides. In rare cases where shoulder reduction is not achieved, spontaneous reduction may occur within a few hours due to the muscle relaxation induced by intramuscularly administered analgesic and sedative medications, even before anesthetic intervention. In our series of four cases involving isolated anterior shoulder dislocations, we identified that spontaneous reduction could occur during natural sleep, without requiring further intervention.6,7
Although no studies specifically addressing the spontaneous reduction of anterior shoulder dislocations during natural sleep have been identified in the literature, several studies have examined the use of analgesic and sedative medications to facilitate shoulder reduction. Hayashi et al. compared intravenous sedation, intra-articular anesthetic application, and peripheral nerve block for anterior shoulder dislocation reduction, concluding that none of these methods had a clear advantage over the others, although respiratory complications were noted with intravenous sedation.7 Studies by Zitek et al., Sithamparapillai et al., and Fitch et al. demonstrated that intra-articular analgesic administration and intravenous sedation had nearly identical effects in assisting anterior shoulder dislocation reduction.8–10 Waterbrook et al. and Viktor et al. highlighted the analgesic effectiveness of intra-articular lidocaine, while Dunn et al. emphasized the sedative effect of intravenous propofol in facilitating anterior shoulder reduction.11–13 Frederics et al. reported that a combined suprascapular and axillary nerve block successfully enabled shoulder reduction without the need for sedation.14
Conclusion
In isolated anterior shoulder dislocation cases where reduction attempts in the emergency unit were unsuccessful, it was observed that the natural sleep state induced by pre-anesthetic administration of intramuscular analgesics and a low dose (5 mg) of intramuscular diazepam facilitated spontaneous reduction of the shoulder joint by relieving the spasm in the surrounding shoulder muscles that prevents reduction. Particularly in elderly patients or those with multiple comorbidities where anesthesia poses risks, the possibility of achieving reduction through the natural sleep process should not be overlooked. We hope that this study will shed light on future research aimed at the treatment of patients with shoulder dislocation and acknowledge that there is a need for studies involving more patients and additional parameters.
Ethics approval
The institutional ethics review board deemed that ethics review was not required.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data are available upon reasonable request from the corresponding author.