


Introduction
Distal femur fractures account for a relatively small proportion of all fractures, representing approximately 3–6% of femoral fractures and less than 1% of all skeletal injuries.1 These injuries typically occur in two distinct populations: elderly individuals with osteoporosis following low-energy trauma, and younger adults exposed to high-energy mechanisms such as traffic accidents or falls from height.2
The surgical treatment of these fractures is often technically demanding due to several factors, including anatomical location, intra-articular extension, metaphyseal comminution, and compromised bone quality.1,3 In elderly osteoporotic patients, maintaining fracture stability is particularly difficult, while in young trauma patients, the complexity of the fracture pattern increases the surgical challenge.4
Retrograde intramedullary nailing (RIMN) and lateral locking plate (LP) fixation are the two most commonly applied surgical techniques for stabilizing distal femoral fractures. RIMN involves the insertion of a nail into the medullary canal to align and fix the fractured bone segments. This method offers benefits such as indirect fracture reduction, minimal soft tissue disruption, shorter operative time, and reduced perioperative blood loss.5,6 However, it may fail to provide adequate stability in osteoporotic bones or highly comminuted metaphyseal fractures.2,7
On the other hand, LP fixation ensures rigid stabilization and is often preferred in multifragmentary fractures involving the metaphysis.8,9 Advantages of this method include enhanced biomechanical stability and more controlled anatomical reduction.10 Nevertheless, increased risk of complications such as soft tissue damage, infection, and nonunion has been reported due to the more extensive surgical dissection required.11,12
Despite numerous studies comparing the two methods, there is still no clear consensus regarding their relative effectiveness. Many reports have shown that RIMN and LP yield comparable outcomes in terms of fracture union, complication rates, implant failure, and postoperative rehabilitation.13,14 Some studies have indicated that LP may offer better postoperative knee mobility but is associated with a higher risk of infection and nonunion,15 whereas others suggest that RIMN results in fewer complications in this regard.16
Overall, each technique has its own strengths and limitations, and the question of superiority remains debated. The present study aims to compare retrograde intramedullary nailing and lateral locking plate fixation in the treatment of distal femur fractures among adult and osteoporotic populations. The analysis focuses on union rate and time, complication rates, implant failure, rehabilitation outcomes, and other clinical parameters.
Methods
This retrospective comparative cohort study was carried out at a single institution between 2018 and 2023, with the aim of comparing the clinical outcomes of retrograde intramedullary nailing (RIMN) and lateral locking plate (LP) fixation in the surgical treatment of distal femur fractures. The study population included both adult trauma patients and elderly individuals with osteoporotic fractures.
Inclusion Criteria
Patients aged 18 years and above who were diagnosed with distal femur fractures—confirmed radiologically and classified under the AO/OTA system as types 33A, 33B, or 33C—were considered eligible for inclusion in this study. Only individuals who had undergone surgical treatment using either retrograde intramedullary nailing (RIMN) or lateral locking plate (LP) fixation techniques were evaluated. Furthermore, a minimum of six months of clinical and radiological follow-up after surgery was required for all participants to be included in the analysis.
Exclusion Criteria
Patients were excluded from the study if they presented with pathological fractures, such as those involving tumor-bearing bone regions. Additional exclusion criteria included periprosthetic fractures located adjacent to total knee arthroplasty implants, any history of prior surgical intervention in the same anatomical area, and individuals younger than 18 years of age.
Patient Groups
Participants in the study were categorized into two groups based on the surgical technique applied. The first group included patients who underwent retrograde intramedullary nailing (RIMN), while the second group consisted of individuals treated with lateral locking plate (LP) fixation. The patient selection process is summarized in Figure 1.

Data Collection
Patient data were retrieved retrospectively from hospital records, outpatient follow-up notes, and radiographic evaluations. The following variables were recorded:
-
Demographics: Age, sex, body mass index (BMI), and comorbid conditions (e.g., diabetes, osteoporosis, hypertension)
-
Fracture-related details: Fracture classification based on the AO/OTA system, side of injury (right/left), and mechanism of trauma (e.g., low-energy fall, high-energy accident)
-
Surgical parameters: Type of fixation (RIMN or LP), surgical duration (minutes), intraoperative blood loss (mL), and postoperative immobilization approach
-
Functional outcomes: Knee range of motion, early or delayed weight-bearing status, and time required to return to daily activities
-
Radiographic outcomes: Union status categorized as complete union, malunion, or nonunion; time to radiographic union (in weeks); final implant positioning
-
Complications: Occurrence of superficial or deep infection, implant-related failure, need for revision surgery, and thromboembolic complications
Power Analysis
To determine the appropriate sample size, a power calculation was conducted prior to data analysis. Drawing upon previously published union rates—86.7% for retrograde intramedullary nailing and 70% for lateral locking plate fixation—the study was designed with a significance threshold of 0.05 and a statistical power of 70%. Based on these parameters, a total of 72 patients (36 in each group) was deemed sufficient to detect meaningful differences between the two treatment modalities.17
Statistical Analysis
Continuous variables were expressed as either mean ± standard deviation (SD) or median with corresponding minimum and maximum values, depending on distribution characteristics. Categorical data were summarized using counts and percentages. To compare differences between groups, the Student’s t-test was used for normally distributed variables, whereas the Mann–Whitney U test was applied for data without normal distribution. Categorical comparisons were conducted using either the Chi-square test or Fisher’s exact test, as appropriate. Kaplan–Meier survival analysis was utilized to assess group differences in time to union and complication rates.18,19 A p-value of less than 0.05 was considered statistically significant. All analyses were performed using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA).
Results
Patient Demographics
A total of 72 patients met the inclusion criteria for this study, with an even distribution across the treatment arms: 36 patients received retrograde intramedullary nailing (RIMN), while the remaining 36 underwent lateral locking plate (LP) fixation. The demographic features of the two cohorts were statistically comparable. Demographic characteristics of the patient groups are presented in Table 1.
No significant intergroup differences were observed with respect to operative parameters, including surgery duration, intraoperative blood loss, or postoperative immobilization strategy. The average surgical time was 75.4 ± 12.3 minutes in the RIMN group and 82.7 ± 14.6 minutes in the LP group (p = 0.07). Estimated intraoperative blood loss was 220 ± 65 mL for RIMN and 240 ± 70 mL for LP (p = 0.22).
Functional Evaluation
In terms of functional outcomes, the average postoperative knee range of motion was found to be 115.2° ± 8.7° in the RIMN group and 110.4° ± 10.1° in the LP group, demonstrating a statistically significant difference in favor of the RIMN group (p = 0.03). An early weight-bearing protocol was feasible in 61.1% of patients treated with RIMN, compared to 44.4% of those in the LP group; however, this difference did not reach statistical significance (p = 0.11). The duration until full resumption of daily living activities was shorter in the RIMN group, averaging 12.3 ± 2.8 weeks, as opposed to 14.1 ± 3.2 weeks in the LP group (p = 0.04). A comprehensive summary of surgical and functional outcome parameters is provided in Table 2.
Radiological Evaluation
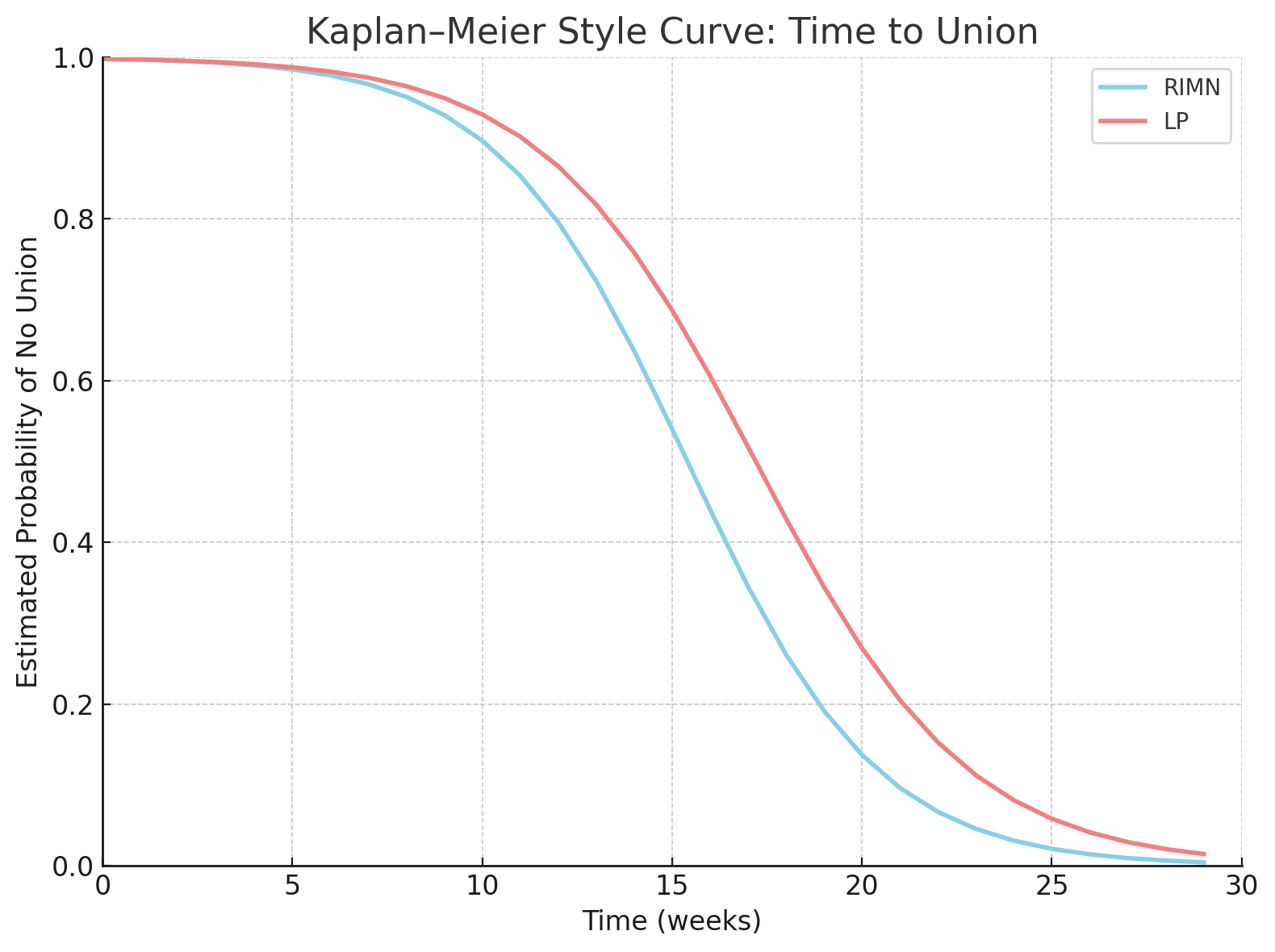
Radiological assessment revealed that the fracture union rate was 86.1% in the RIMN group and 75.0% in the LP group, though the difference was not statistically significant (p = 0.27). The average time to radiographic union was measured as 15.4 ± 4.1 weeks in the RIMN group, compared to 17.2 ± 4.6 weeks in the LP group, with a borderline p-value of 0.05. Kaplan–Meier survival analysis did not demonstrate a significant difference between the two fixation methods regarding time to union (log-rank p = 0.09). The Kaplan–Meier style curve showing estimated union probability over time is presented in Figure 2.

Complications
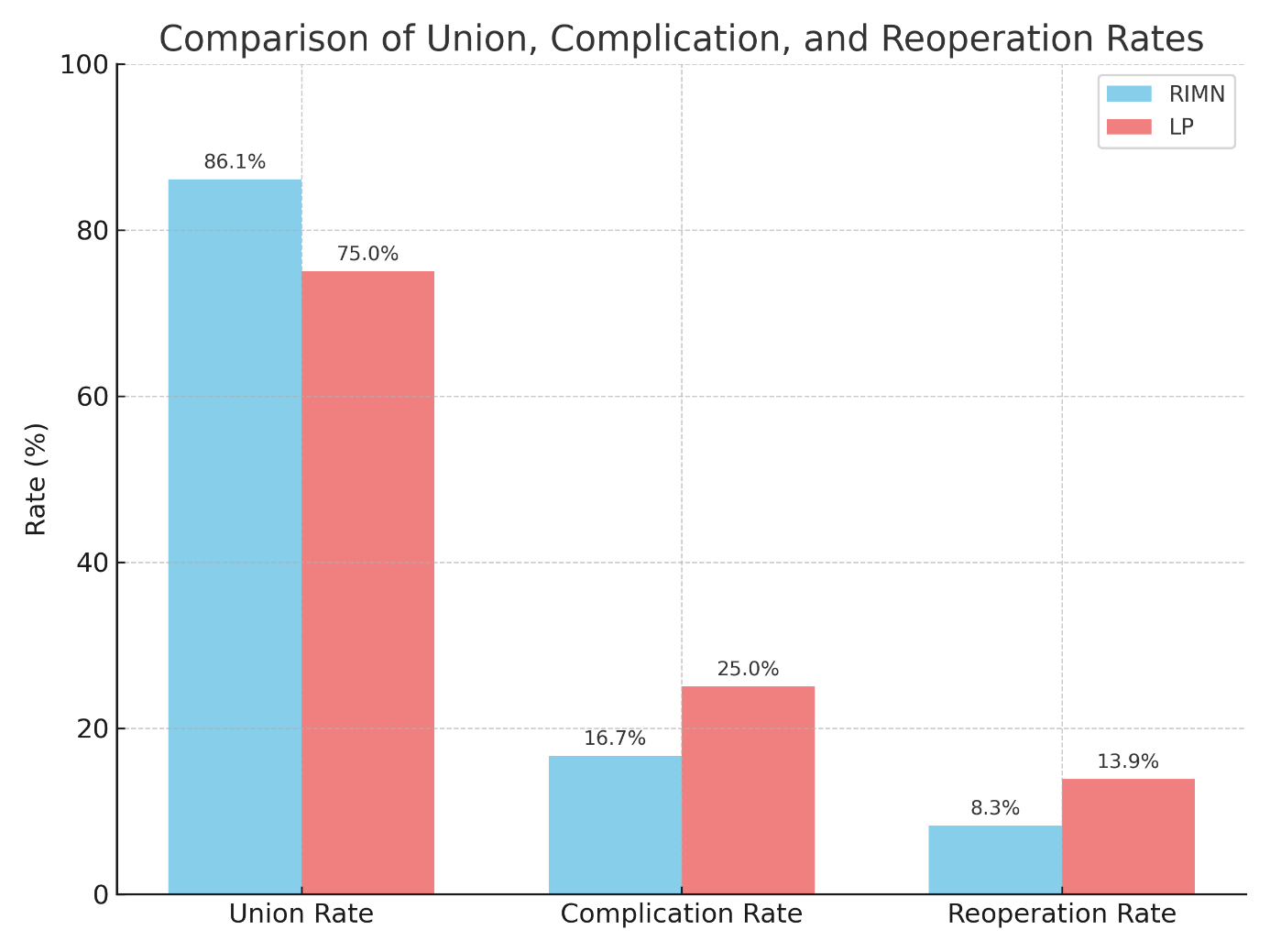
A total of 6 patients (16.7%) in the RIMN group and 9 patients (25.0%) in the LP group experienced postoperative complications; this difference did not reach statistical significance (p = 0.41).
Among the reported complications, nonunion occurred in 2 patients (5.6%) following RIMN and in 4 patients (11.1%) treated with LP (p = 0.32). Postoperative infections were identified in 2 patients (5.6%) from the RIMN group and 3 patients (8.3%) from the LP group (p = 0.64). Implant failure was observed in 2 individuals (5.6%) in both groups (p = 1.00).
Additionally, secondary surgical intervention was required in 3 patients (8.3%) in the RIMN group and in 5 patients (13.9%) from the LP group (p = 0.46). A detailed summary of complication types and reoperation rates is presented in Table 3. A visual comparison of union, complication, and reoperation rates between the two groups is provided in Figure 3.

.png)

Discussion
In this retrospective cohort study, we aimed to evaluate and compare the effectiveness of retrograde intramedullary nailing (RIMN) and lateral locking plate (LP) fixation in managing distal femur fractures among adult and osteoporotic patients. The results indicated that while both treatment modalities yielded clinically satisfactory outcomes, certain variables revealed notable differences between the two approaches.
In our study, the observed union rate was 86.1% in patients treated with RIMN and 75.0% in those managed with LP fixation. These outcomes are consistent with existing literature, which highlights the favorable healing potential of retrograde nailing in distal femur fractures. For instance, Papadokostakis et al. conducted a meta-analysis demonstrating that RIMN was associated with both high union rates and a relatively low incidence of complications in such injuries.20 Similarly, Van Rysselberghe et al., in a multicenter cohort study, reported union rates of 86.7% for RIMN and 78% for LP, aligning closely with our results.21
Our findings demonstrated that retrograde intramedullary nailing resulted in more favorable radiographic outcomes compared to lateral plating, particularly in terms of faster union and higher healing success. These results align with the literature, where several studies have reported shorter union times and lower nonunion rates associated with RIMN, especially in osteoporotic bone.22,23 However, some evidence suggests that fracture morphology and fixation strategy also influence healing dynamics, which may explain variations in outcomes across studies.24 These results are consistent with the systematic review by Shah et al., which reported equivalent union rates between RIMN and LP in periprosthetic distal femur fractures, emphasizing that the choice of implant may depend on fracture configuration and bone quality.25
Functional Outcomes
In terms of postoperative knee mobility, the average range of motion was calculated as 115.2° in the RIMN group and 110.4° in the LP group, indicating a statistically significant advantage in favor of RIMN (p = 0.03). This result is consistent with several prior studies suggesting superior knee joint function following retrograde intramedullary nailing. For example, DeKeyser et al. reported more favorable range of motion outcomes in patients who underwent RIMN in a biomechanical investigation.10
Conversely, Vallier et al. found differing results, reporting a mean range of motion of 115° in patients treated with percutaneous plate osteosynthesis, compared to 100° in those who underwent retrograde nailing.3 These conflicting findings underscore the influence of implant type and surgical technique on functional recovery. These results are also supported by Kim et al., who in a meta-analysis of over 2,000 patients reported superior outcomes for RIMN in terms of union time and range of motion.26
Additionally, early weight-bearing was achievable in 61.1% of patients in the RIMN group, compared to 44.4% in the LP group, although this difference did not reach statistical significance (p = 0.11). Nevertheless, various sources in the literature support the view that RIMN may facilitate earlier mobilization in the postoperative period.2,4,10–12,16
Complications and Reoperation Requirement
In the current study, the overall complication rate was recorded as 16.7% in the RIMN group and 25.0% in the LP group. Although this intergroup difference was not statistically significant (p = 0.41), a higher incidence of nonunion was observed among patients treated with LP (11.1% versus 5.6%). Despite a higher complication rate observed in the LP group, the difference did not reach statistical significance. The limited sample size might have affected the power to detect a meaningful difference. A similar trend was reported by Jain et al., who noted a greater nonunion rate in patients undergoing plate fixation.27 Similarly, Neradi et al. found no significant difference in complication rates, but reported that RIMN was more favorable in terms of early weight-bearing.28
The infection rate was found to be 5.6% for RIMN and 8.3% for LP. Notably, Kontakis et al. reported that no postoperative wound complications or infections occurred in patients treated with RIMN.29 Moreover, Markmiller et al. and Liporace et al. emphasized that while LP fixation provides robust mechanical stability, it may be associated with an increased risk of infection due to soft tissue dissection.5
Implant failure was observed in 5.6% of cases in both groups (p = 1.00). However, several studies have suggested that RIMN may be associated with a lower rate of hardware failure.2,8,13,22,30 The need for secondary surgical intervention was 8.3% in the RIMN group and 13.9% in the LP group. These rates are in line with previously published data.31,32 Kale et al. emphasized the importance of tailoring fixation techniques to patient characteristics, highlighting the acceptability of both methods when appropriately indicated.33
A key strength of this study lies in its adequate sample size, which allowed for a reliable comparison of the two fixation methods. In addition, the comprehensive analysis of specific complications contributed to a more nuanced understanding of the clinical outcomes associated with each technique. Nonetheless, several limitations must be acknowledged. These include the retrospective nature of the design, lack of randomization in group assignment, variations in surgical protocols between centers, and incomplete follow-up in a subset of patients.
In summary, both RIMN and LP were found to be clinically viable options for the surgical treatment of distal femur fractures. However, retrograde nailing demonstrated advantages in terms of union rate, healing time, and functional recovery, particularly in osteoporotic patients. Therefore, the choice of surgical technique should be individualized based on fracture characteristics and patient-specific factors.
Conclusion
This study compared retrograde intramedullary nailing (RIMN) and lateral locking plate (LP) fixation in the management of distal femur fractures. Both techniques were found to be clinically effective, with acceptable complication rates. However, RIMN demonstrated superior outcomes in terms of radiographic union, healing time, and knee joint function, particularly in patients with osteoporotic bone. LP fixation remains a viable option, especially in complex fracture patterns and metaphyseal zones requiring angular stability. These findings suggest that surgical strategy should be individualized according to patient-specific and fracture-related factors. Further prospective, randomized studies are necessary to confirm these results and guide treatment algorithms.