Introduction
ACL injuries are significant due to their potential to cause substantial long-term consequences if not properly managed. These injuries are not only common but also have a profound impact on an individual’s mobility, quality of life, and overall knee function. When an ACL injury occurs, it often leads to knee instability, which can cause recurrent episodes of giving way, pain, and swelling. This instability can significantly impair daily activities and athletic performance, and if left untreated, it can result in progressive joint damage, including meniscal tears and the early onset of osteoarthritis.1–3
Reconstruction surgery, typically involving the replacement of the torn ACL with a graft, aims to restore knee stability and function. The primary goal of this surgical intervention is to re-establish the mechanical properties of the knee, allowing patients to return to their pre-injury levels of activity and reduce the risk of further joint degeneration.4,5 The success of this procedure, however, is heavily dependent on the healing process of the graft within the bone tunnel. This healing is a complex, multi-phase process that includes the initial inflammatory response, the proliferation of cells and extracellular matrix, and the long-term remodeling of the graft into a functional ligament.6,7
Understanding the molecular biology of graft healing is crucial for optimizing rehabilitation protocols and improving clinical results.8,9 The biological processes involved in graft healing are governed by various molecular and cellular mechanisms, including the release of cytokines and growth factors, cellular proliferation, matrix synthesis, and the remodeling of collagen fibers.10,11 By gaining insights into these molecular events, clinicians can develop targeted interventions to enhance the healing process. For instance, identifying key molecular targets can lead to the development of pharmacological agents that accelerate healing or improve graft integration.12,13
Moreover, an in-depth understanding of the molecular biology of ACL graft healing can inform the design of rehabilitation protocols. Early mechanical loading, when appropriately timed and controlled, has been shown to stimulate cellular activities that promote graft maturation and strength.14,15 Therefore, a thorough knowledge of the molecular mechanisms can help in determining the optimal timing and intensity of rehabilitation exercises, thereby improving patient outcomes and reducing the risk of graft failure.16,17
In conclusion, ACL injuries necessitate effective management strategies to prevent long-term complications. Reconstruction surgery is a cornerstone treatment, and the healing of the graft is pivotal to its success. By delving into the molecular biology of graft healing, we can refine rehabilitation protocols and enhance clinical outcomes, ultimately improving the quality of life for patients undergoing ACL reconstruction.18,19
Healing Phases of ACL Graft and Molecular Mechanisms
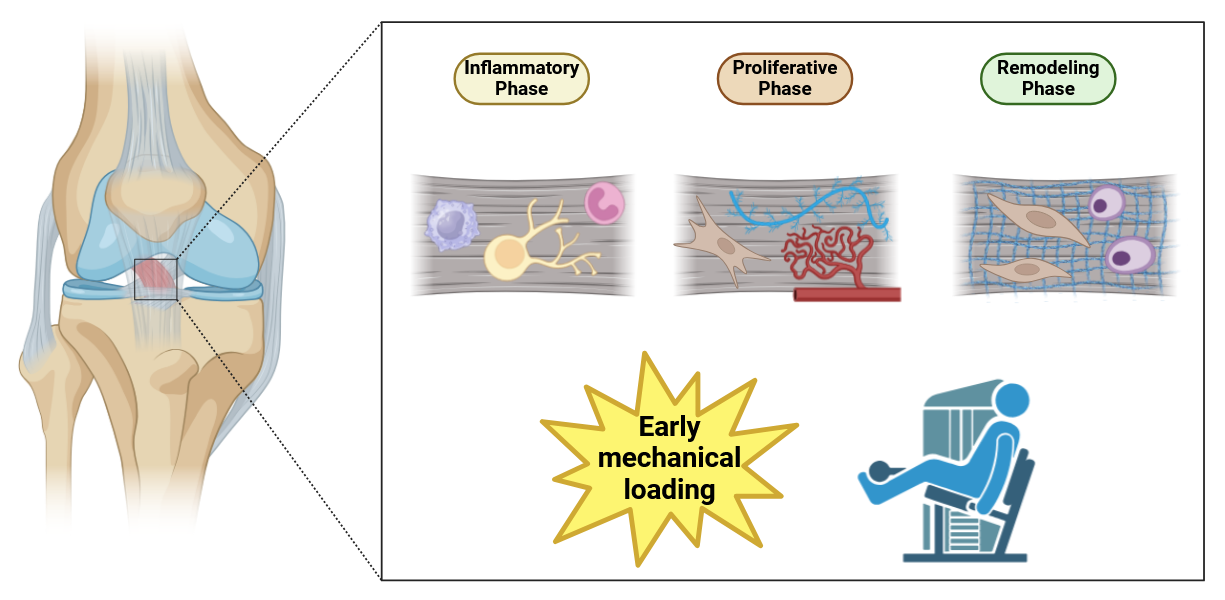
The healing process of an ACL graft is a complex and dynamic sequence of events that can be broadly divided into three main phases: inflammatory, proliferative, and remodeling.20 Each of these phases encompasses distinct molecular and cellular activities that are crucial for the successful integration and function of the graft (Figure 1).21
In the inflammatory phase, which begins immediately after the graft is implanted, the body’s initial response involves the recruitment of inflammatory cells, such as macrophages, neutrophils, and lymphocytes, to the site of injury.22 These cells release a variety of cytokines and growth factors that are vital for initiating the healing process.23 The inflammatory response serves to clear away necrotic tissue and debris, setting the stage for the subsequent phases of healing.24 The delicate balance of inflammation is crucial, as excessive inflammation can lead to further tissue damage and fibrosis, hindering graft integration.25
Following the inflammatory phase, the proliferative phase begins.26 This phase is marked by the proliferation of fibroblasts, which are essential for the synthesis of the extracellular matrix (ECM).27 The ECM provides a scaffold for new tissue formation, promoting structural integrity and support for the graft.28 During this phase, growth factors such as transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF) play significant roles.29 These factors regulate fibroblast activity, collagen production, and angiogenesis, ensuring that the graft is well-nourished and supported by a network of new blood vessels.30 The molecular mechanisms during this phase involve the activation of various signaling pathways, such as the TGF-β/Smad pathway and the hypoxia-inducible factor-1 alpha (HIF-1α) pathway, which are crucial for cell proliferation and ECM synthesis.31
The final phase, remodeling, extends over several months to years and involves the maturation and reorganization of the initially formed tissue into a structure that closely resembles a native ligament.32 This phase is characterized by the alignment of collagen fibers along the lines of mechanical stress, enhancing the biomechanical properties of the graft.33 Cellular activities are regulated by mechanical signals and molecular factors that promote tissue maturation and functional integration.34 The remodeling phase involves the downregulation of pro-inflammatory cytokines and the upregulation of anabolic factors, such as the Wnt/β-catenin signaling pathway, which regulates fibroblast differentiation and collagen synthesis.35 Additionally, matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs) play a critical role in balancing collagen degradation and synthesis, ensuring the formation of a durable and functional ligament.36
Understanding these phases is essential for optimizing surgical techniques and rehabilitation protocols, ultimately leading to improved clinical outcomes for patients undergoing ACL reconstruction (Table 1).37 By gaining insights into the molecular and cellular mechanisms underlying each phase, clinicians and researchers can develop targeted therapies and interventions that enhance graft healing, reduce complications, and accelerate recovery.38 This comprehensive understanding is key to advancing patient care and achieving successful long-term outcomes in ACL reconstruction surgery.39

1. Inflammatory Phase
The inflammatory phase is the initial response following anterior cruciate ligament (ACL) graft implantation and is crucial for setting the stage for subsequent healing processes.40 Beginning immediately after surgery and typically lasting several days to a week, this phase is characterized by an influx of inflammatory cells—including macrophages, neutrophils, and lymphocytes—to the site of injury.41 These cells are recruited through chemotactic signals released by damaged tissue and the surgical site, such as chemokines like CCL2 (monocyte chemoattractant protein-1) and CXCL8 (interleukin-8), creating a robust inflammatory environment essential for initiating the healing cascade.42
Macrophages and neutrophils play pivotal roles by releasing a plethora of cytokines and growth factors, including interleukins (IL-1, IL-6), tumor necrosis factor-alpha (TNF-α), and transforming growth factor-beta (TGF-β).43 These signaling molecules orchestrate the removal of necrotic tissue and debris through phagocytosis, as macrophages and neutrophils recognize damage-associated molecular patterns (DAMPs) via pattern recognition receptors (PRRs) like toll-like receptors (TLRs) on their surfaces.44 The engagement of these receptors triggers intracellular signaling pathways, such as the nuclear factor-kappa B (NF-κB) and mitogen-activated protein kinase (MAPK) pathways, leading to the production of additional pro-inflammatory mediators.45 Additionally, cytokines like TNF-α and IL-1β enhance vascular permeability by inducing the expression of adhesion molecules (e.g., selectins and integrins) on endothelial cells, facilitating leukocyte extravasation and a greater influx of immune cells to the site.46
Early mechanical loading during this phase can significantly impact graft healing.47 Controlled loading—such as passive motion or low-intensity weight-bearing exercises—promotes vascularization and modulates inflammation.48 Mechanical stimuli are sensed by mechanosensitive ion channels and integrins on the surfaces of cells like fibroblasts and endothelial cells, initiating intracellular signaling cascades such as the focal adhesion kinase (FAK), extracellular signal-regulated kinase (ERK), and phosphoinositide 3-kinase/Akt (PI3K/Akt) pathways.49 Activation of FAK leads to the assembly of focal adhesions and influences cytoskeletal reorganization, while the ERK pathway regulates gene expression involved in cell proliferation and survival.50 These pathways modulate the production of cytokines and growth factors, like vascular endothelial growth factor (VEGF), enhancing angiogenesis and facilitating a smoother transition to the proliferative phase.51 However, excessive or inappropriate mechanical loading can lead to overactivation of inflammatory pathways and increased production of reactive oxygen species (ROS), exacerbating tissue damage and must be carefully managed.52
While the inflammatory response is essential for kickstarting healing, excessive or prolonged inflammation can lead to tissue damage and fibrosis, negatively impacting graft healing.53 Therefore, a balanced inflammatory response is critical.54 Optimal inflammation involves timely resolution, where anti-inflammatory signals and cytokines prevail, signaling the transition to the proliferative phase.55 Modulating the inflammatory response through pharmacological agents or controlled mechanical loading can enhance graft healing by reducing excessive inflammation and promoting a conducive environment for repair.56 Anti-inflammatory treatments or therapies that target specific cytokines and immune cells, such as monoclonal antibodies against TNF-α or IL-1β, can be strategically employed to improve healing outcomes.57
The inflammatory phase also involves the activation of molecular pathways like NF-κB, which regulates the expression of pro-inflammatory genes.58 Activation of NF-κB occurs when inflammatory signals such as TNF-α and IL-1β bind to their respective receptors—TNF receptor (TNFR) and IL-1 receptor (IL-1R)—on immune and resident cells, triggering adaptor proteins like MyD88 and leading to the activation of the IκB kinase (IKK) complex.59 The IKK complex phosphorylates the inhibitor IκBα, targeting it for ubiquitination and degradation by the proteasome.60 This degradation releases NF-κB dimers (typically p65/p50), allowing them to translocate into the nucleus.61 In the nucleus, NF-κB binds to specific κB sites on DNA, promoting the transcription of genes encoding pro-inflammatory cytokines, chemokines, adhesion molecules, and enzymes such as cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) involved in the inflammatory response.62 Negative feedback mechanisms, including the synthesis of IκBα itself and other inhibitory proteins like A20, limit NF-κB activity, ensuring that the inflammatory response is robust yet transient.63
Moreover, the resolution of inflammation is mediated by anti-inflammatory cytokines like interleukin-10 (IL-10) and TGF-β, which help dampen the inflammatory response and promote tissue repair.64 IL-10 signals through the Janus kinase 1 (JAK1) and tyrosine kinase 2 (Tyk2), activating the signal transducer and activator of transcription 3 (STAT3) transcription factor, which suppresses the expression of pro-inflammatory genes and promotes the expression of anti-inflammatory genes.65 TGF-β signals through Smad-dependent pathways, where receptor-regulated Smads (R-Smads) are phosphorylated and form complexes with Smad4, translocating to the nucleus to regulate gene expression involved in extracellular matrix production and cell differentiation.66 Other molecular pathways, including the MAPK pathways (e.g., p38 MAPK, JNK) and the JAK/STAT pathways, contribute to regulating immune responses and tissue repair by influencing cell proliferation, apoptosis, differentiation, and cytokine signaling.67 For instance, activation of the p38 MAPK pathway can lead to the production of pro-inflammatory cytokines but also plays a role in cell differentiation and apoptosis, highlighting the complexity of these signaling networks.68
In summary, the inflammatory phase involves a complex interplay of immune cells, cytokines, chemokines, and molecular signaling pathways that work together to clear debris, prevent infection, and set the stage for tissue repair.69 Properly controlled early mechanical loading can enhance this phase by activating key mechanotransduction pathways, promoting vascularization through the upregulation of angiogenic factors, and modulating inflammation by influencing cytokine profiles.70 Understanding and manipulating these molecular mechanisms and signaling pathways can lead to improved strategies for enhancing graft healing and ultimately better clinical outcomes for patients undergoing ACL reconstruction.71
2. Proliferative Phase
Following the inflammatory phase, the proliferative phase commences, characterized by fibroblast proliferation and extracellular matrix (ECM) production, typically spanning from a few days to several weeks post-surgery.72 During this period, the primary goal is to rebuild and strengthen the tissue at the graft site, providing structural support for long-term healing and integration.73
Fibroblasts migrate to the graft site in response to chemotactic signals released during the inflammatory phase, such as platelet-derived growth factor (PDGF) and transforming growth factor-beta (TGF-β).74 Once they reach the site, fibroblasts become activated and begin synthesizing collagen and other ECM components like glycosaminoglycans, elastin, and proteoglycans.75 The ECM serves as a scaffold that provides structural support and facilitates new cell attachment and growth, essential for restoring the mechanical strength and stability of the graft.76
The production of ECM is tightly regulated by various growth factors and signaling pathways. TGF-β plays a crucial role by binding to its receptors (TGF-β type I and type II receptors) on fibroblasts, activating the Smad-dependent signaling pathway.77 Upon ligand binding, TGF-β receptor type II phosphorylates and activates receptor type I, which then phosphorylates receptor-regulated Smads (R-Smads), specifically Smad2 and Smad3.78 The phosphorylated Smads form complexes with Smad4 and translocate into the nucleus to regulate gene expression.79 This process promotes the synthesis of type I and III collagen and other ECM components, enhancing fibroblast proliferation and differentiation.80
In addition to the Smad pathway, TGF-β can activate Smad-independent pathways such as the mitogen-activated protein kinase (MAPK) pathways, including extracellular signal-regulated kinase (ERK), c-Jun N-terminal kinase (JNK), and p38 MAPK.81 These pathways further influence gene expression related to ECM production, cell proliferation, and differentiation.82
Platelet-derived growth factor (PDGF) stimulates cell migration, proliferation, and ECM production by binding to its tyrosine kinase receptors (PDGFR-α and PDGFR-β) on fibroblasts.83 This interaction leads to receptor dimerization and autophosphorylation, activating downstream signaling cascades such as the phosphatidylinositol 3-kinase (PI3K)/Akt pathway and the Ras/Raf/MEK/ERK pathway.84 The PI3K/Akt pathway promotes cell survival and growth, while the ERK pathway regulates gene expression involved in cell proliferation and ECM synthesis, supporting robust scaffold formation.85
Vascular endothelial growth factor (VEGF) is critical for angiogenesis, promoting new blood vessel formation that supplies the graft with nutrients and oxygen.86 VEGF expression is upregulated in response to hypoxic conditions within the healing graft, mediated by hypoxia-inducible factor-1 alpha (HIF-1α).87 Under low oxygen levels, HIF-1α stabilizes and translocates to the nucleus, where it dimerizes with HIF-1β and binds to hypoxia-responsive elements (HREs) in the promoter regions of target genes, including VEGF.88 The increased VEGF expression enhances angiogenesis, improving nutrient and oxygen delivery to the healing tissue.89
Other cytokines like fibroblast growth factors (FGFs) and insulin-like growth factors (IGFs) contribute by stimulating fibroblast proliferation and enhancing collagen synthesis.90 FGFs bind to fibroblast growth factor receptors (FGFRs), activating signaling pathways such as MAPK and PI3K/Akt, which promote cell proliferation and ECM production.91 IGFs signal through the IGF-1 receptor (IGF-1R), also activating downstream pathways that support cell growth and survival.92
Early mechanical loading during this phase enhances healing by stimulating fibroblast activity and promoting collagen alignment within the ECM.93 Controlled exercises activate integrin-mediated signaling pathways in fibroblasts. Integrins are transmembrane receptors that connect the ECM to the cell’s cytoskeleton and sense mechanical cues.94 Mechanical stimulation leads to integrin clustering and activation of focal adhesion kinase (FAK).95 Activated FAK triggers downstream signaling cascades, including the Ras/MAPK and PI3K/Akt pathways, enhancing fibroblast proliferation, ECM production, and structural organization.96
Mechanical signals also influence the expression of ECM-remodeling enzymes like matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs), ensuring a balance between ECM synthesis and degradation.97 For example, mechanical loading can upregulate MMP expression to facilitate ECM remodeling while promoting TIMP expression to prevent excessive ECM degradation.98 This balanced remodeling is essential for proper tissue repair and integration of the graft.
Excessive mechanical loading can disrupt ECM formation and should be carefully calibrated.99 Overloading may lead to increased MMP activity without adequate TIMP regulation, resulting in excessive ECM degradation and weakening of the graft.100 Therefore, controlled mechanical stimuli are crucial for optimal healing outcomes.
Understanding the complex interactions and regulatory mechanisms during the proliferative phase provides valuable insights into optimizing graft healing.101 Therapeutic strategies that target specific signaling pathways—such as administering growth factors or using pharmacological agents to modulate TGF-β, PDGF, or VEGF signaling—can enhance ECM production and tissue integration.102 Additionally, designing rehabilitation protocols that incorporate controlled mechanical loading can activate beneficial mechanotransduction pathways, promoting efficient healing and better clinical outcomes for patients undergoing ACL reconstruction [103].
3. Remodeling Phase
The remodeling phase is the final and longest phase of anterior cruciate ligament (ACL) graft healing, extending from several months to years [103]. During this period, the initially disorganized collagen fibers and extracellular matrix (ECM) undergo extensive maturation and reorganization to form a structure that closely resembles a native ligament.103 This transformation is crucial for the graft to acquire the mechanical properties necessary for proper knee function.104
At the molecular level, the remodeling process involves a delicate balance between the degradation of immature collagen and the synthesis of mature collagen types, primarily collagen type I, which confer tensile strength and durability to the graft.105 Matrix metalloproteinases (MMPs), particularly MMP-1 and MMP-13, play pivotal roles in degrading disorganized and immature collagen fibers.106 The activity of MMPs is tightly regulated by tissue inhibitors of metalloproteinases (TIMPs), ensuring that collagen degradation does not exceed synthesis.107 This balance is essential for proper ECM remodeling and is influenced by various signaling pathways.
Mechanical loading plays a crucial role in aligning collagen fibers in the direction of tensile forces, enhancing the biomechanical properties of the graft.108 Mechanotransduction pathways, such as the integrin-mediated focal adhesion kinase (FAK) pathway, are activated by mechanical stimuli.109 When mechanical stress is applied, integrins on the cell surface interact with ECM proteins, leading to the activation of FAK and downstream signaling molecules like extracellular signal-regulated kinases (ERK) and RhoA/ROCK pathways.110 These signaling cascades promote cytoskeletal reorganization and the expression of genes involved in collagen synthesis and alignment, ensuring that the collagen fibers can bear the stresses and strains placed on the knee during movement.111
Throughout the remodeling phase, the graft undergoes “ligamentization,” progressively acquiring the histological and biomechanical characteristics of a natural ligament.112 This involves reorganization of collagen fibers and differentiation of fibroblasts into ligament-like cells known as ligamentocytes.113 The differentiation process is regulated by signaling pathways such as the Wnt/β-catenin pathway and the transforming growth factor-beta (TGF-β) pathway.114 The Wnt/β-catenin signaling pathway is activated when Wnt proteins bind to Frizzled receptors on the cell surface, preventing the degradation of β-catenin.115 Accumulated β-catenin translocates into the nucleus and regulates the expression of target genes that promote fibroblast differentiation and mature collagen synthesis.116
Similarly, the TGF-β pathway plays a significant role in tissue maturation during the remodeling phase.117 TGF-β binds to its receptors on fibroblasts, activating Smad-dependent signaling pathways.118 Phosphorylated Smad2 and Smad3 form complexes with Smad4 and translocate to the nucleus, where they regulate gene expression promoting ECM production and inhibiting MMP expression.119 This leads to increased synthesis of collagen type I and decreased degradation of ECM components, contributing to tissue strengthening.120
The balance between MMPs and TIMPs is also regulated by the Wnt/β-catenin and TGF-β pathways, ensuring proper ECM remodeling.121 Additionally, mechanical loading influences these signaling pathways, as mechanotransduction can modulate the expression of Wnt ligands and TGF-β, integrating mechanical and biochemical signals to optimize graft maturation.122
The graft gradually integrates with the surrounding bone and ligament tissue, achieving structural and functional stability.123 This integration is supported by new blood vessel formation mediated by angiogenic factors like vascular endothelial growth factor (VEGF).124 Hypoxia-inducible factor-1 alpha (HIF-1α) accumulates under low oxygen conditions within the graft, promoting VEGF expression and angiogenesis.125 A continuous supply of nutrients and oxygen is vital for ongoing cellular activities within the graft, supporting the metabolic demands of remodeling cells.126
Additionally, the remodeling phase involves forming a robust bone-ligament interface, critical for the graft’s long-term stability and functionality.127 Osteoblasts and osteoclasts remodel the bone around the graft, ensuring a strong and durable attachment.128 Signaling pathways such as the receptor activator of nuclear factor kappa-B ligand (RANKL)/osteoprotegerin (OPG) system regulate osteoclast differentiation and activity, balancing bone resorption and formation.129 Bone morphogenetic proteins (BMPs), particularly BMP-2 and BMP-7, are involved in osteogenesis by promoting osteoblast differentiation through the Smad signaling pathway.130
The molecular biology of the remodeling phase involves downregulation of pro-inflammatory cytokines and upregulation of anabolic factors that promote tissue maturation.131 The downregulation of inflammatory signals reduces the activity of catabolic pathways that could otherwise degrade ECM components.132 Growth factors such as insulin-like growth factor-1 (IGF-1) and fibroblast growth factors (FGFs) promote anabolic activities, enhancing collagen synthesis and fibroblast proliferation.133
Moreover, signaling pathways like the mechanistic target of rapamycin (mTOR) pathway play a role in regulating protein synthesis and cell growth during the remodeling phase.134 Activation of the mTOR pathway stimulates ribosomal biogenesis and translation of proteins necessary for ECM production.135 Additionally, the Notch signaling pathway contributes to cell differentiation and tissue remodeling by regulating gene expression involved in cell fate determination.136
In conclusion, the healing process of an ACL graft during the remodeling phase is characterized by intricate molecular and cellular events that lead to the maturation and strengthening of the graft.137 Signaling pathways such as Wnt/β-catenin, TGF-β/Smad, integrin-mediated mechanotransduction, and others coordinate the activities of fibroblasts, osteoblasts, and other cells involved in tissue remodeling.138 Early and controlled mechanical loading is essential, as it activates mechanotransduction pathways that enhance collagen alignment and graft maturation while preventing excessive degradation.139 Understanding these molecular mechanisms provides valuable insights into optimizing rehabilitation protocols and developing therapeutic strategies to improve graft healing and clinical outcomes for patients undergoing ACL reconstruction.140
Impact of Early Mechanical Loading
Mechanical loading plays a crucial role in the functional recovery of the anterior cruciate ligament (ACL) graft post-surgery.141 Introducing mechanical load early in the rehabilitation process has been shown to significantly enhance graft healing.142 This enhancement is achieved by stimulating cellular activities that lead to better collagen fiber alignment, which is essential for the strength and durability of the graft.143
Research has consistently demonstrated that early mechanical loading can result in improved outcomes for patients recovering from ACL reconstruction.144 For instance, allowing partial weight-bearing within the first 1–2 weeks (e.g., 20–30% of body weight on the operative leg) and initiating gentle range-of-motion (ROM) exercises have been associated with faster revascularization of the graft and improved joint proprioception.145 Mechanical stimuli activate mechanoreceptors on cells within the graft and surrounding tissues, leading to the activation of intracellular signaling pathways such as the integrin-mediated focal adhesion kinase (FAK) pathway and the mitogen-activated protein kinase/extracellular signal-regulated kinase (MAPK/ERK) pathway.146 These pathways promote cell proliferation, differentiation, and extracellular matrix (ECM) remodeling, which are critical for graft maturation and integration.147
To illustrate, early resistance exercises (e.g., isometric quadriceps sets or straight-leg raises) can often be introduced by weeks 2–4—provided the patient has adequate pain control and can maintain near-full knee extension without undue strain on the graft. Sessions might be performed 2–3 times per day, using 1–2 sets of 10 repetitions for each exercise. This carefully controlled loading not only maintains muscle activation but also aligns with molecular cues that direct collagen deposition and graft remodeling.147
Mechanical loading also increases the expression of growth factors like transforming growth factor-beta (TGF-β) and vascular endothelial growth factor (VEGF).148 TGF-β stimulates collagen synthesis and extracellular matrix production via the Smad signaling pathway, enhancing tissue strength and integrity.149 VEGF promotes angiogenesis, improving blood flow and nutrient delivery to the healing graft.150
However, the success of this approach hinges on carefully considering the timing and intensity of the loading regimen.151 Progressively increasing the load from partial to full weight-bearing over 4–6 weeks, for example, ensures that the graft is not overloaded in its early, more vulnerable stages.152 Excessive or inappropriate mechanical loading can lead to graft damage or failure by overloading the healing tissues before they have acquired sufficient strength. Therefore, rehabilitation protocols must be meticulously designed to gradually increase mechanical stress in a controlled manner, allowing the graft to adapt and strengthen over time.153
Studies have shown that specific types of mechanical loading, such as cyclic tensile strain, positively influence cell behavior and extracellular matrix production.154 For example, applying cyclic mechanical strain to ligament fibroblasts increases the expression of collagen type I and decreases the expression of collagen type III, resulting in a stronger and more resilient tissue.155 Clinically, this may translate into low-intensity, high-frequency motion exercises (e.g., stationary cycling with minimal resistance for 10–15 minutes, 2–3 times a day), starting around 3–4 weeks postoperatively, to provide consistent, cyclic stimulus without excessive load.
Moreover, mechanical loading influences collagen fiber alignment through mechanotransduction mechanisms involving cytoskeletal reorganization.156 This process is mediated by the RhoA/ROCK pathway, which regulates actin stress fiber formation and focal adhesion assembly, contributing to the structural organization of the healing tissue.157 Functional exercises like mini-squats (0–45° knee flexion, 2–3 sets of 10 repetitions, 3 times per week) introduced around weeks 6–8 can further leverage these pathways, promoting optimal fiber alignment.
Early mechanical loading also affects the expression of matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs), which are crucial for extracellular matrix remodeling.158 Controlled loading can balance MMP and TIMP expression, promoting appropriate matrix turnover and preventing excessive degradation or scar formation.159 For instance, combining mild-to-moderate resistance exercises (e.g., 30–50% 1RM, 2–3 sets of 8–10 reps) with balance training helps maintain ECM homeostasis throughout the proliferative phase of healing.
Understanding these molecular mechanisms allows clinicians to optimize rehabilitation strategies, tailoring mechanical loading to enhance graft healing while minimizing risks.160 Progressing to functional and sport-specific drills (e.g., lateral shuffles or controlled agility drills) by months 3–4—once muscle strength and neuromuscular control are sufficiently restored—further enhances collagen alignment and tensile strength of the graft. By integrating controlled mechanical stimuli into rehabilitation programs, patients can achieve better functional outcomes, reduced recovery times, and a successful return to activity after ACL reconstruction [162].
1. Biomechanical Stimuli and Molecular Mechanisms in Graft Healing
Mechanical stimuli play a fundamental role in regulating cellular behavior within a healing graft by activating mechanotransduction pathways [162]. These pathways enable cells to convert mechanical signals—such as tension, compression, and shear stress—into biochemical responses that influence cellular functions essential for tissue repair and regeneration.161 Mechanical forces initiate a cascade of signaling events that affect gene expression, protein synthesis, and cellular behavior.162
Integrins are central components in these pathways.163 As transmembrane receptors, they facilitate adhesion between the cell and the extracellular matrix (ECM), bridging the intracellular cytoskeleton with the ECM to transmit mechanical signals.164 Upon binding to ECM components, integrins cluster and recruit intracellular proteins to form focal adhesions—complex assemblies that act as signaling hubs, relaying mechanical information into the cell.165 Focal adhesion kinase (FAK) is crucial in the signaling processes initiated at focal adhesions.166 Activated integrins recruit FAK, which becomes phosphorylated and sets off downstream signaling cascades involving molecules like Src family kinases and mitogen-activated protein kinases (MAPKs).167 These cascades influence gene expression, cytoskeletal dynamics, and key cellular functions such as proliferation, migration, and differentiation.168
Other mechanosensitive molecules also contribute to the transmission of mechanical signals.169 Mechanosensitive ion channels respond to mechanical stress by altering ion fluxes across the cell membrane, affecting cell signaling pathways like the calcium-dependent pathways that modulate cellular activities.170 The cytoskeleton, composed of actin and microtubules, senses and responds to mechanical stimuli through dynamic remodeling, essential for transmitting forces and maintaining cellular integrity.171 Mechanotransduction involves signaling molecules and transcription factors that regulate gene expression in response to mechanical cues.172 Transcriptional regulators like Yes-associated protein (YAP) and transcriptional co-activator with PDZ-binding motif (TAZ) translocate to the nucleus under mechanical stress, interacting with transcription factors like TEAD to regulate genes involved in cell proliferation, survival, and differentiation.173
Cellular responses to mechanical signals include increased collagen production and tissue remodeling, vital for the stability and functionality of the healing graft.174 Upregulated collagen synthesis enhances the structural integrity of the graft, while coordinated ECM degradation and synthesis ensure proper organization and integration with surrounding tissue.175 Small GTPases such as RhoA, Rac1, and Cdc42 regulate cytoskeletal dynamics and cell motility in mechanotransduction pathways.176 Acting as molecular switches, they control processes like stress fiber formation, cell contractility, adhesion, migration, and spreading, which are crucial for tissue repair and ECM organization.177
Understanding these molecular mechanisms is crucial for developing therapeutic strategies to enhance graft integration and healing.178 One practical application is the design of specific rehabilitation protocols that incorporate controlled mechanical loading to stimulate beneficial cellular responses. In the earliest postoperative stage (first 2 weeks), for instance, passive range of motion exercises—such as gentle knee flexion and extension—are introduced to promote synovial fluid movement and prevent joint stiffness without overstressing the graft.179 This gentle movement activates mechanosensitive pathways, encouraging vascularization and modulating inflammation through the production of growth factors like VEGF.180
As healing progresses, rehabilitation protocols can introduce active range of motion exercises and low-intensity resistance training. Exercises like stationary cycling with minimal resistance (10–15 minutes, 1–2 times daily) or aquatic therapy provide a safe environment for increasing joint mobility and muscle strength while minimizing impact forces.181 These activities stimulate mechanotransduction pathways involving integrins and FAK, promoting fibroblast proliferation and collagen synthesis.182 The gradual increase in mechanical load encourages the alignment of collagen fibers along the lines of stress, enhancing the tensile strength of the graft through the reorganization of the ECM mediated by molecules like MMPs and TIMPs.183
Advanced stages of rehabilitation might incorporate functional exercises that mimic daily activities or sport-specific movements. Incorporating motor control training and neurocognitive training, such as using perturbation drills or performing single-leg stands with closed eyes (3 sets of 30-second holds, 3–4 times weekly), can enhance neuromuscular control and joint stability.184 These exercises engage mechanosensitive ion channels and cytoskeletal components, improving the coordination of muscle activation patterns and joint proprioception through the modulation of signaling pathways like the PI3K/Akt pathway.185
Throughout the rehabilitation process, careful monitoring of mechanical loading is essential to prevent overstimulation of mechanotransduction pathways that could lead to adverse effects like fibrosis or graft failure.186 Excessive mechanical stress may cause an overproduction of collagen and ECM components, leading to stiffening of the tissue and reduced functionality.187 By tailoring the intensity and duration of exercises, clinicians can modulate molecular responses to optimize healing outcomes.188
Pharmacological interventions may also complement mechanical rehabilitation strategies. For example, agents that modulate specific signaling pathways involved in mechanotransduction could enhance the healing process. Inhibitors of RhoA/ROCK pathway may reduce excessive fibrotic responses, while agonists of YAP/TAZ pathways could promote regenerative processes.189 However, such interventions require careful consideration and further research to understand their effects fully and avoid unintended consequences.190
Biomaterials engineered to mimic the mechanical properties of native tissue present another practical application. Scaffolds with specific stiffness and elasticity can influence cell behavior by providing appropriate mechanical cues, promoting desired cellular responses through mechanotransduction pathways.191 These materials can be used in grafts to enhance integration and healing by aligning cellular responses with the mechanical environment.192
In summary, mechanical stimuli guide cellular behavior during graft healing through complex mechanotransduction pathways involving integrins, FAK, mechanosensitive ion channels, and cytoskeletal components.193 Rehabilitation protocols that incorporate controlled mechanical loading play a crucial role in activating these molecular mechanisms, promoting beneficial cellular responses like increased collagen production, fibroblast proliferation, and ECM remodeling.194 Practical applications include carefully designed exercise programs that progress in intensity and complexity, biomaterials that provide optimal mechanical environments, and potential pharmacological agents targeting specific pathways.195 The regulation of these processes is crucial for successful graft healing and functional integration, and continued research into these mechanisms holds significant potential for improving clinical outcomes in tissue engineering and regenerative medicine.196
2. Optimal Loading Regimens and Molecular Mechanisms in Graft Healing
Determining the optimal loading regimen maximizes the benefits of early mechanical loading while minimizing the risk of graft damage.116 Controlled, gradual introduction of mechanical load enhances the graft’s biomechanical properties by stimulating cellular activities essential for integration and maturation, such as fibroblast proliferation, collagen synthesis, and extracellular matrix (ECM) organization.117
Mechanical stimuli are sensed by mechanoreceptors like integrins, which, upon mechanical loading, undergo conformational changes leading to focal adhesion formation.118 These sites initiate mechanotransduction signals involving proteins like focal adhesion kinase (FAK) and paxillin.119 Phosphorylated FAK triggers downstream signaling cascades, including the MAPK/ERK and PI3K/Akt pathways.120 The MAPK/ERK pathway promotes cell proliferation and differentiation, vital during early mechanical loading for graft integration.121 The PI3K/Akt pathway enhances cell survival and metabolism, ensuring cells remain viable and responsive to mechanical cues.122
Mechanical loading influences ECM production and organization by inducing collagen gene expression and protein secretion.123 Mechanosensitive molecules like transforming growth factor-beta (TGF-β) regulate collagen synthesis and ECM remodeling, contributing to the tissue’s mechanical strength.124 Transcriptional co-activators YAP and TAZ adapt cellular responses to mechanical environments by modulating gene expression related to proliferation, differentiation, and ECM production.125 Epigenetic modifications, influenced by mechanical stimuli, regulate gene accessibility involved in mechanotransduction and tissue repair.126 Small GTPases like RhoA, Rac1, and Cdc42 regulate cytoskeletal dynamics and cell motility, essential for maintaining tissue tension and integrity, cell migration, and ECM reorganization.127
Implementing optimal loading regimens requires a multidisciplinary approach that considers molecular and cellular healing mechanisms.128 Tailored rehabilitation programs incorporating controlled mechanical loading stimulate beneficial responses without causing re-injury.129 Monitoring the graft’s response allows for regimen adjustments based on healing progress.130
Specific rehabilitation protocols involve gradually increasing the intensity and complexity of exercises to align with the graft’s healing stages. In the immediate postoperative period (Weeks 0–2), passive range of motion (PROM) exercises are initiated to maintain joint mobility without stressing the graft excessively.134 Gentle knee flexion and extension movements (5–10 minutes, 3–5 times daily) promote synovial fluid distribution, reducing inflammation and supplying nutrients to the healing tissues.135 These movements activate mechanotransduction pathways at a low intensity, stimulating initial cellular responses necessary for healing.136
As healing progresses, active-assisted range of motion (AAROM) exercises and isometric strengthening are introduced.137 Patients engage muscles with assistance, further stimulating mechanosensitive pathways while protecting the graft.138 Low-resistance exercises like quadriceps sets and straight-leg raises (1–2 sets of 10 repetitions, 2–3 times per day) promote muscle activation, enhance blood flow and stress relaxation.139 These activities stimulate fibroblast proliferation and collagen synthesis through activation of MAPK/ERK and PI3K/Akt pathways, contributing to ECM production and organization.140
In the proliferative phase (Weeks 4–8), weight-bearing exercises are progressively incorporated.141 Closed kinetic chain activities like mini-squats (within a comfortable knee flexion range) and heel raises (2–3 sets of 10–12 reps, 2–3 times per week) apply controlled compressive forces across the joint.142 These exercises enhance joint stability and promote alignment of collagen fibers along lines of stress, improving the graft’s tensile strength.143 Mechanical loading at this stage further activates integrin-mediated signaling pathways, reinforcing cytoskeletal organization and ECM remodeling.144
Proprioceptive and motor control exercises, such as single-leg stands on stable or unstable surfaces, are essential components of rehabilitation.145 They enhance neuromuscular control and coordination by engaging mechanosensitive ion channels and small GTPases that regulate cytoskeletal dynamics.146 These exercises facilitate re-establishment of normal joint kinematics and reduce the risk of future injuries.147
Advanced rehabilitation includes functional and sport-specific exercises to prepare the patient for return to full activity.148 Activities like agility drills, plyometric exercises, and controlled running impose higher mechanical loads, stimulating robust activation of mechanotransduction pathways.149 This promotes further maturation of the graft through enhanced collagen cross-linking and ECM consolidation.150 For instance, light plyometrics (e.g., box jumps or gentle hop drills at low volume) may be introduced around 3–4 months postoperatively, after adequate strength and neuromuscular stability have been achieved.
Throughout rehabilitation, it is crucial to monitor the patient’s response to loading and adjust the regimen accordingly.151 Overloading can lead to excessive activation of signaling pathways, potentially causing graft failure or adverse tissue responses like fibrosis.152 Conversely, insufficient loading may result in inadequate stimulation of cellular processes necessary for optimal healing.153 Individualized rehabilitation plans that consider the patient’s progress and specific needs are essential.154
Understanding these mechanisms opens avenues for developing therapies to enhance graft healing, such as combining mechanical loading with growth factors or cytokines and targeting specific signaling pathways through gene therapy.155 Supplementing rehabilitation with platelet-rich plasma (PRP) injections may provide additional growth factors like TGF-β and PDGF, enhancing fibroblast activity and collagen synthesis.156 Gene therapy approaches could involve delivering genes encoding beneficial proteins like VEGF to promote angiogenesis and improve graft integration.157
In summary, optimal loading regimens enhance graft healing by leveraging mechanotransduction pathways.132 Controlled mechanical stimulation activates molecular signals promoting cell proliferation, survival, differentiation, and ECM organization, improving the success of graft-based treatments.133 Structured rehabilitation protocols, tailored to the healing stages and individual patient needs, apply practical applications of these molecular principles—from gentle PROM in the early weeks to progressive resistance and balance training—thus facilitating efficient and effective recovery.158
3. Molecular Responses to Loading
Mechanical loading elicits molecular responses integral to graft healing.196 Mechanical forces initiate signal transduction pathways that modulate gene expression, protein synthesis, and cellular behaviors essential for tissue repair.197 Mechanical stimuli upregulate genes associated with collagen synthesis and extracellular matrix (ECM) remodeling, notably COL1A1 and COL3A1, enhancing tissue mechanical properties by increasing the production of type I and type III collagen fibers.198
Simultaneously, mechanical loading stimulates matrix metalloproteinases (MMPs) such as MMP-1, MMP-2, and MMP-9, facilitating ECM degradation and remodeling by breaking down denatured collagen and other ECM components.199 The balance between MMPs and tissue inhibitors of metalloproteinases (TIMPs) ensures proper tissue remodeling by regulating ECM turnover and preventing excessive degradation.200 This equilibrium is crucial for maintaining the structural integrity of the healing tissue while allowing for necessary remodeling processes.
Mechanical loading promotes the release of growth factors like transforming growth factor-beta (TGF-β), which enhances collagen synthesis and modulates ECM components and MMPs, orchestrating balanced remodeling.201 TGF-β binds to its receptors on fibroblasts, activating the Smad signaling pathway that translocates to the nucleus to regulate gene expression related to ECM production and cell differentiation.202 Vascular endothelial growth factor (VEGF) is also upregulated, promoting angiogenesis and ensuring adequate nutrient and oxygen supply to the healing graft by stimulating the formation of new blood vessels.203 VEGF expression can be induced by mechanical stress through the activation of hypoxia-inducible factor-1 alpha (HIF-1α) under hypoxic conditions within the graft.
Controlled mechanical loading modulates inflammation by promoting anti-inflammatory cytokines like interleukin-10 (IL-10) and suppressing excessive pro-inflammatory responses, creating a conducive environment for tissue repair.204 Mechanical forces influence immune cell function and cytokine production, shifting the inflammatory balance towards resolution and promoting the transition to the proliferative phase of healing.205
At the cellular level, mechanical loading activates mechanosensitive ion channels, such as transient receptor potential (TRP) channels and stretch-activated ion channels, leading to calcium influx and activation of intracellular signaling pathways like calmodulin-dependent kinases (CaMKs).206 The increase in intracellular calcium serves as a secondary messenger, activating enzymes and transcription factors that regulate proliferation, differentiation, and apoptosis.207 This calcium signaling is essential for coordinating cellular activities during tissue repair.
Key signaling pathways like the mitogen-activated protein kinase/extracellular signal-regulated kinase (MAPK/ERK) and phosphoinositide 3-kinase/Akt (PI3K/Akt) promote cell proliferation, survival, and differentiation in response to mechanical stimuli.208 Activation of the MAPK/ERK pathway leads to the phosphorylation of transcription factors such as Elk-1 and c-Fos, enhancing the expression of genes involved in cell cycle progression.209 The PI3K/Akt pathway facilitates cell survival by inhibiting apoptotic processes and promoting protein synthesis through downstream effectors like the mammalian target of rapamycin (mTOR).210
Mechanical loading can induce epigenetic modifications, such as changes in DNA methylation and histone acetylation, regulating gene expression patterns associated with repair.211 Mechanical forces can influence the activity of histone acetyltransferases (HATs) and histone deacetylases (HDACs), altering chromatin structure and accessibility of transcriptional machinery to DNA.212 These epigenetic changes can upregulate or downregulate genes critical for tissue repair and regeneration.
The Hippo signaling pathway is also influenced by mechanical loading, with transcriptional co-activators Yes-associated protein (YAP) and transcriptional co-activator with PDZ-binding motif (TAZ) promoting genes involved in proliferation and ECM production.213 Under mechanical stress, YAP and TAZ translocate to the nucleus and interact with transcription factors like TEAD, regulating gene expression that drives cell growth, inhibits apoptosis, and enhances ECM synthesis.214
Mechanical loading enhances integrin production and activity, strengthening cell-ECM adhesion and signal transduction.215 This activation initiates cascades involving Rho family GTPases, such as RhoA, Rac1, and Cdc42, which regulate cytoskeletal dynamics and cell motility.216 RhoA promotes the formation of stress fibers and focal adhesions, Rac1 controls lamellipodia formation for cell spreading, and Cdc42 is involved in filopodia formation, aiding in cell migration and ECM organization crucial for tissue repair.217
The molecular events triggered by mechanical loading collectively enhance graft healing by promoting collagen synthesis, ECM remodeling, angiogenesis, and modulating inflammation.218 This integration of mechanical and biochemical signals optimizes the healing process by ensuring that cells respond appropriately to their mechanical environment, leading to improved structural and functional outcomes of the graft.219
In conclusion, early mechanical loading is vital in rehabilitation following ACL reconstruction. Managing mechanical stimuli allows clinicians to improve graft healing and recovery outcomes.220 Understanding these molecular mechanisms facilitates the development of targeted therapies and protocols that enhance tissue repair and integration, ensuring successful and durable graft healing.221
Clinical Implications from Molecular Biology
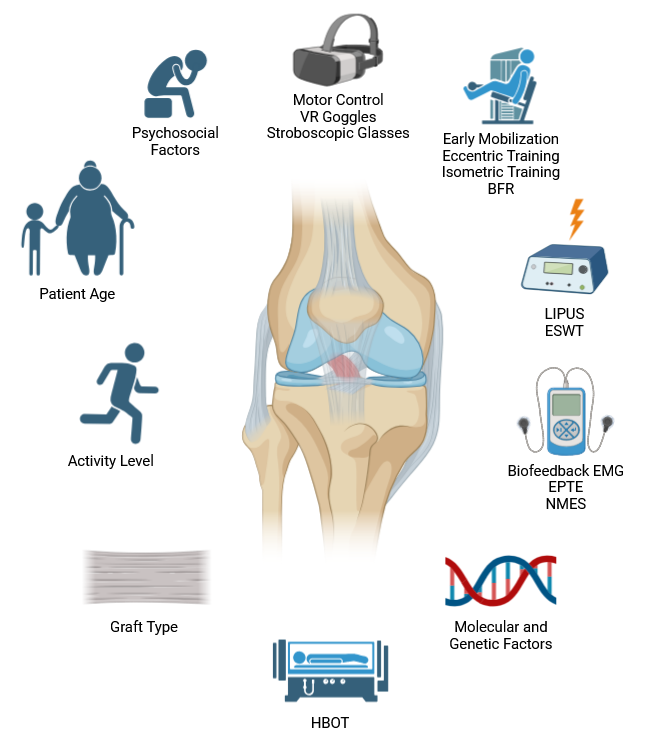
Understanding the molecular responses to early mechanical loading can significantly impact the development of optimized rehabilitation protocols (Figure 2).222 When rehabilitation specialists comprehend how the body’s cells and tissues react to mechanical stress, they can design targeted strategies that facilitate better healing and functional recovery.223 Integrating early low-intensity exercises into rehabilitation regimens can activate specific biological pathways that accelerate graft maturation and integration.224 This early intervention is essential as it can bolster the graft’s structural integrity, enhancing its strength and resilience.225 Consequently, patients experience improved clinical outcomes, including quicker restoration of mobility and strength, compared to conventional rehabilitation approaches that might delay movement initiation.226 These optimized protocols not only support faster recovery but also reduce the likelihood of complications, ensuring that patients can resume their daily activities and sports with greater confidence and a lower risk of re-injury.227
1. Optimizing Rehabilitation Protocols through Molecular Understanding
Understanding the molecular responses to early mechanical loading can significantly impact the development of optimized rehabilitation protocols (Figure 2).228 When rehabilitation specialists comprehend how the body’s cells and tissues react to mechanical stress, they can design targeted strategies that facilitate better healing and functional recovery.229 Integrating early low-intensity exercises into rehabilitation regimens can activate specific biological pathways that accelerate graft maturation and integration.230 This early intervention is essential as it can bolster the graft’s structural integrity, enhancing its strength and resilience.231 Consequently, patients experience improved clinical outcomes, including quicker restoration of mobility and strength, compared to conventional rehabilitation approaches that might delay movement initiation.232 These optimized protocols not only support faster recovery but also reduce the likelihood of complications, ensuring that patients can resume their daily activities and sports with greater confidence and a lower risk of re-injury.233
Early mobilization protocols yield better knee function and graft integration than immobilization (Table 2).234 Traditional rehabilitation relied on extended immobilization for graft protection and healing,235 but recent studies show it causes joint stiffness, muscle atrophy, and delayed recovery.236 In contrast, early mobilization creates a dynamic healing environment by triggering mechanical and molecular responses that enhance tissue repair.237
Molecularly, early mobilization activates integrins, initiating FAK and MAPK/ERK pathways that upregulate genes for cell proliferation and survival.238–241 It increases growth factors like TGF-β and VEGF, promoting collagen synthesis and angiogenesis.242–244
Eccentric training enhances tendon stiffness and collagen synthesis by upregulating collagen genes COL1A1 and COL3A1 and activating the phosphoinositide 3-kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) pathway via insulin-like growth factor 1 (IGF-1).245 Mechanical loading during eccentric contractions increases IGF-1 expression, which binds to IGF-1 receptors on muscle and tendon cells, activating PI3K/Akt signaling.246 This pathway promotes protein synthesis and cell growth by activating mTOR, leading to increased collagen production and improved tendon properties.247
Isometric training boosts muscle strength and reduces pain by increasing nitric oxide (NO) production.248 NO promotes vasodilation, enhancing blood flow to muscles and tendons, and activates the MAPK/ERK pathway, leading to muscle relaxation and repair.249 NO production is mediated by endothelial nitric oxide synthase (eNOS) and neuronal nitric oxide synthase (nNOS), which are upregulated during isometric contractions.250 The MAPK/ERK pathway enhances the expression of genes involved in muscle repair and regeneration, such as MyoD and myogenin.251 Additionally, NO has anti-inflammatory effects by inhibiting pro-inflammatory cytokines like TNF-α and IL-1β.252
Blood flow restriction (BFR) training induces a hypoxic environment in muscles by applying external pressure to limbs during low-intensity exercise.253 Hypoxia elevates hypoxia-inducible factor 1-alpha (HIF-1α), which upregulates VEGF expression, enhancing angiogenesis.254 BFR also stimulates the release of growth hormone (GH) and IGF-1, activating the PI3K/Akt/mTOR pathway, promoting muscle protein synthesis and hypertrophy.255 Increased GH levels stimulate hepatic production of IGF-1, which binds to IGF-1 receptors, activating anabolic signaling pathways.256
Neuromuscular electrical stimulation (NMES) prevents muscle atrophy and improves strength by electrically activating motor neurons, inducing muscle contractions.257 NMES activates the PI3K/Akt pathway, which inhibits protein degradation by downregulating ubiquitin-proteasome pathways and autophagy-related genes.258 It enhances the expression of myogenic regulatory factors like MyoD and myogenin, promoting muscle fiber regeneration and hypertrophy.259
Biofeedback electromyography enhances motor learning by providing real-time feedback on muscle activation patterns.260 This increases brain-derived neurotrophic factor (BDNF) levels, activating cAMP response element-binding protein (CREB) pathways.261 CREB regulates genes involved in synaptic plasticity and neuronal survival, improving neural connections and muscle recruitment efficiency.262
Stroboscopic glasses train proprioception and visual-motor coordination by intermittently obstructing vision, forcing reliance on proprioceptive input.263 This enhances neural plasticity by upregulating synaptic proteins like synapsin I and neurotrophic factors such as BDNF and nerve growth factor (NGF).264 These changes strengthen synaptic connections and improve sensory integration.265 Stroboscopic training enhances cortical excitability and neuroplasticity through modulation of neurotransmitter systems, including glutamate and GABA.266
Motor control exercises with an external focus improve movement efficiency and coordination by directing attention to the effect of movement rather than the movement itself.267 This approach optimizes neural pathways by reducing co-contractions and promoting automaticity in motor patterns.268 It enhances synaptic plasticity and strengthens neural circuits involved in motor control through long-term potentiation mechanisms mediated by NMDA receptor activation.269 These exercises also modulate dopamine release, associated with motivation and motor learning.270
Percutaneous electrical stimulation delivers electrical currents directly to the healing tissue via needles inserted into the skin, enhancing ACL graft healing through specific molecular mechanisms.271 The electrical currents activate voltage-gated ion channels, leading to cell membrane depolarization and increased intracellular calcium levels.272 This rise in calcium activates calcium-dependent signaling pathways like calmodulin-dependent kinases (CaMKs) and protein kinase C (PKC), which regulate gene expression and protein synthesis crucial for tissue repair.273 Additionally, electrical stimulation modulates heat shock proteins (HSPs), which protect cells from stress and aid in protein folding and repair.274 It also influences fibroblast and tenocyte activity, increasing collagen production and aligning collagen fibers along the lines of electrical current, thereby improving the mechanical properties of the graft.275 Electrical stimulation reduces inflammation by decreasing pro-inflammatory cytokines like TNF-α and IL-1β and increasing anti-inflammatory cytokines such as IL-10, creating a favorable environment for tissue healing.276
Extracorporeal Shockwave Therapy (ESWT) promotes healing by delivering high-energy acoustic waves to tissues.277 It upregulates VEGF and endothelial nitric oxide synthase (eNOS), enhancing angiogenesis.278 ESWT increases the expression of neuropeptides like substance P and calcitonin gene-related peptide (CGRP), modulating pain and inflammation.279 It activates the Wnt/β-catenin signaling pathway, stimulating cell proliferation and differentiation necessary for tissue regeneration.280
Hyperbaric oxygen therapy (HBOT) increases oxygen delivery to tissues by having patients breathe pure oxygen in a pressurized chamber.281 It supports angiogenesis through upregulation of VEGF and fibroblast growth factor 2 (FGF-2).282 HBOT enhances collagen synthesis by stimulating fibroblast activity and increasing pro-collagen mRNA expression.283 It reduces oxidative stress by upregulating antioxidant enzymes like superoxide dismutase (SOD) and catalase, protecting cells from damage.284 HBOT also modulates inflammatory responses by decreasing pro-inflammatory cytokines and increasing anti-inflammatory cytokines.285
Virtual Reality (VR) glasses improve motor learning and neural plasticity by providing immersive environments that stimulate multiple sensory modalities.286 VR training increases BDNF levels and activates CREB pathways, promoting synaptic plasticity and cortical reorganization.287 It reorganizes cortical maps by enhancing neurogenesis and dendritic branching in motor and sensory cortices.288 VR modulates neurotransmitters like dopamine and serotonin, enhancing motivation, mood, and cognitive function, contributing to better rehabilitation outcomes.289 The engaging nature of VR increases adherence to rehabilitation programs, improving recovery.290 Studies show VR-based rehabilitation improves functional outcomes after ACL reconstruction by enhancing proprioception, balance, and coordination.291
Understanding these molecular mechanisms allows clinicians to design rehabilitation protocols that maximize healing, graft integration, muscle strength, and joint stability, ensuring better long-term outcomes after ACL reconstruction.292
2. Patient-Specific Approaches
Tailoring rehabilitation protocols to individual patient characteristics, such as age, activity level, and graft type, can significantly enhance recovery outcomes.293 Personalized rehabilitation acknowledges each patient’s uniqueness, moving away from a one-size-fits-all approach. By considering specific factors, specialists can create customized protocols that address distinct needs, optimizing healing and improving overall recovery.294
For instance, patients with higher activity levels or professional athletes may require a more aggressive rehabilitation program to facilitate an earlier return to sport while minimizing the risk of re-injury.295 Conversely, older patients or those with lower physical demands might benefit from a more conservative approach that focuses on gradual strength and mobility improvements.296 The type of graft used in ACL reconstruction also influences rehabilitation strategies; for example, patellar tendon grafts may require different considerations compared to hamstring tendon grafts due to variations in donor site morbidity and healing times.297
Research has demonstrated that individualized rehabilitation programs lead to better functional outcomes and higher satisfaction rates.298 By tailoring exercises to address specific deficits in strength, flexibility, and proprioception, therapists can enhance the efficacy of rehabilitation.299 Additionally, accounting for psychological factors such as fear of movement or re-injury can improve patient adherence and engagement.300
Advancements in technology, such as biomechanical assessment tools and wearable devices, enable clinicians to monitor patient progress and adjust rehabilitation protocols in real-time.301 Furthermore, incorporating patient preferences and goals into the rehabilitation plan promotes a patient-centered approach that can improve motivation and outcomes.302
In summary, customizing rehabilitation protocols based on individual patient characteristics is crucial for optimizing recovery after ACL reconstruction. This personalized approach can enhance graft healing, restore function more effectively, and facilitate a safer return to activity.303
Age
Age is a crucial factor in designing rehabilitation protocols. Younger patients typically have higher metabolic rates and more robust healing responses, allowing for more aggressive rehabilitation. Molecularly, they exhibit greater cellular proliferation, differentiation, and efficient DNA repair.304–307 Higher levels of growth factors like insulin-like growth factor 1 (IGF-1) and fibroblast growth factor (FGF) enhance protein synthesis, muscle cell proliferation, angiogenesis, and fibroblast activation.308,309 Additionally, a favorable extracellular matrix (ECM) composition and effective immune responses facilitate quicker inflammation resolution and tissue repair.310–312 Active satellite cells in younger individuals further promote muscle regeneration.313 Consequently, aggressive rehabilitation with higher-intensity exercises and faster progression can rapidly restore strength, flexibility, and function.
Older patients, however, may experience slower tissue healing due to decreased cellular activity and reduced protein synthesis capacity.314–319 Aging is associated with shorter telomeres, increased cellular senescence, and diminished regenerative capacity, leading to a pro-inflammatory environment that impairs healing.320,321 The ECM becomes stiffer and more fibrotic, and there is a decline in critical growth factors and anabolic responses.322,323 Mitochondrial dysfunction and increased reactive oxygen species (ROS) production further hinder the healing process.324,325 For older individuals, a gradual rehabilitation approach with low-intensity exercises and slower progression is necessary to avoid graft overload and complications. This method minimizes inflammation and excessive scar tissue formation, supported by targeted interventions like antioxidant supplementation or anti-inflammatory treatments using compounds such as curcumin and resveratrol.326–331 Adequate nutritional support, including essential amino acids, vitamins C and D, and minerals like zinc and magnesium, is also crucial for collagen synthesis and tissue repair.332–334
By understanding these molecular and physiological differences, clinicians can design rehabilitation protocols that maximize healing, graft integration, muscle strength, and joint stability, ensuring better long-term outcomes after ACL reconstruction.
Activity Level
Activity level prior to injury or surgery is crucial for effective rehabilitation protocols.335 Highly active individuals and athletes require programs that quickly restore high function and performance. Molecularly, exercises that enhance mitochondrial biogenesis and muscle hypertrophy through PGC-1α and mTOR pathways are essential.336,337 PGC-1α promotes mitochondrial gene expression and oxidative capacity, while mTOR stimulates protein synthesis and muscle growth.338,339 Rehabilitation for these patients may include sport-specific exercises, agility training, high-intensity interval training (HIIT), and resistance training to increase muscle mass and mitochondrial function.340,341 Additionally, these activities boost the release of myokines like irisin and IL-6, which aid in muscle repair and metabolism.342,343
Sedentary individuals or those with lower physical demands benefit from less intensive programs focused on restoring basic functionality and promoting overall health.344 Emphasizing aerobic capacity and cardiovascular health activates AMP-activated protein kinase (AMPK) and VEGF pathways, enhancing metabolic health and angiogenesis.345,346 Low-impact activities such as walking, cycling, and swimming improve endurance and flexibility without excessive stress.347 Moreover, balance and coordination exercises like tai chi and yoga enhance functional ability and reduce injury risk by upregulating brain-derived neurotrophic factor (BDNF), which supports neural plasticity and proprioception.348,349
By customizing rehabilitation based on a patient’s pre-injury activity level, clinicians can optimize recovery outcomes.350 For highly active individuals, the goal is to swiftly restore peak performance, while for more sedentary individuals, the focus is on improving general health and functional capacity.351 This individualized approach ensures that each patient receives appropriate care tailored to their specific needs and lifestyle, enhancing overall recovery and long-term success.352
Graft Type
The type of graft used in surgery significantly influences the rehabilitation strategy.353 Autografts, taken from the patient’s own body, typically integrate faster, allowing for accelerated rehabilitation.354 They benefit from immediate vascularization and viable cells like fibroblasts, endothelial cells, and mesenchymal stem cells (MSCs), which express matrix metalloproteinases (MMP-1, MMP-2, and MMP-9) to efficiently remodel the extracellular matrix (ECM).355,356 Autografts contain intact ECM components such as collagen types I and III, elastin, and glycosaminoglycans (GAGs), providing scaffolds for cell attachment and migration.357 Growth factors like transforming growth factor-beta (TGF-β) and vascular endothelial growth factor (VEGF) are more active in autografts, promoting angiogenesis and collagen synthesis.358,359 However, autografts involve donor site morbidity, requiring careful management to balance healing at both graft and donor sites.360 Effective pain management and monitoring inflammatory cytokines like interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) are crucial.361,362
Allografts, sourced from donors, avoid donor site complications but require a more conservative rehab approach due to slower integration from delayed neovascularization and immune responses.363,364 Allografts lack viable cells and contain donor antigens (human leukocyte antigen (HLA) molecules) that can trigger immune responses, necessitating immunosuppressive strategies.365,366 Their integration relies on creeping substitution, where host cells gradually replace donor tissues, influenced by graft preparation methods.367,368
Optimizing rehabilitation for both graft types involves incorporating biomaterials or growth factors like platelet-rich plasma (PRP) to enhance cellular adhesion and matrix production.369,370 Mechanical loading through controlled physical therapy stimulates mechanotransduction pathways, enhancing cellular responses.371–373 Biodegradable scaffolds seeded with MSCs can further promote graft integration by providing environments for cell growth and controlled release of growth factors.374,375 For allografts, immunomodulatory strategies such as decellularization and MSC application help reduce antigenicity and promote tolerance.376,377
By tailoring rehabilitation to the specific graft type, clinicians can optimize healing and integration, reduce complications, and promote successful long-term outcomes.378 Understanding the molecular biology of graft healing informs the timing, intensity, and type of interventions, leading to more personalized and effective rehabilitation strategies.379
Molecular and Genetic Factors
Advances in molecular biology and genetics are crucial for patient-specific rehabilitation, allowing protocols to be tailored based on individual genetic variations that influence injury response and healing.380–408 Genetic variations can affect collagen synthesis, inflammation, and tissue repair. Single nucleotide polymorphisms (SNPs) in genes like COL1A1, COL5A1, IL-6, and TNF-α provide insights into tissue healing and inflammatory responses.381–386 For example, the COL1A1 Sp1 binding site polymorphism affects collagen production and injury risk, while SNPs in IL-6 and TNF-α genes modulate inflammation and muscle regeneration.383–386 Genotyping these polymorphisms helps clinicians predict healing challenges and customize rehabilitation protocols, such as focusing on strengthening exercises for those with weaker collagen structures.
Molecular markers like C-reactive protein (CRP), matrix metalloproteinases (MMPs), and growth factors (IGF-1, TGF-β, VEGF) enable real-time monitoring of healing progress.387–390 CRP levels indicate systemic inflammation, guiding exercise intensity to avoid exacerbating inflammation.388 Elevated MMPs signal active ECM remodeling, informing the timing of strength training.389 Growth factors reflect anabolic processes, allowing adjustments to enhance tissue regeneration.390
Epigenetics also enhances personalized treatment by influencing gene expression through DNA methylation and histone acetylation.391–396 For instance, hypomethylation of the IL-10 promoter increases its anti-inflammatory effects, promoting tissue repair.392,393 Exercise-induced histone acetylation of PGC-1α enhances muscle endurance and recovery.394 Assessing epigenetic markers enables clinicians to predict and modulate responses to rehabilitation, using interventions like nutraceuticals or pharmacological agents to optimize gene expression.395,396
Novel therapeutic approaches from molecular biology, such as gene therapy and CRISPR-Cas9, offer enhanced healing by introducing genes that promote tissue repair.397–400 Gene delivery of growth factors like bone morphogenetic proteins (BMPs) and fibroblast growth factors (FGFs) using viral or non-viral vectors can boost tissue regeneration.399,400 Additionally, advanced biomaterials and drug delivery systems, including biodegradable scaffolds and hydrogels infused with microRNAs (miRNAs) or small interfering RNAs (siRNAs), create optimal healing environments.401–404 These materials can release therapeutic agents that regulate gene expression and reduce fibrosis, improving tissue repair.402–404
Personalized rehabilitation protocols integrate genetic information, molecular markers, and advanced therapies to tailor interventions to each patient’s biological profile.405–407 For example, patients with genetic variants leading to heightened inflammation may benefit from anti-inflammatory treatments like non-steroidal anti-inflammatory drugs (NSAIDs) in the first two days post-surgery or omega-3 supplements.406 Those with impaired collagen synthesis might receive nutritional support with vitamin C, lysine, and proline.407 Pharmacogenomics further personalizes medication choices to enhance efficacy and reduce adverse effects during rehabilitation.408
By leveraging genetic variations, molecular markers, epigenetic modifications, and novel therapeutic techniques, rehabilitation protocols can be highly individualized. This personalized approach maximizes healing, minimizes complications, and accelerates recovery, leading to improved outcomes and faster return to normal activities.380–408
Psychosocial Factors
Psychological and social factors, including motivation, support systems, and mental health, significantly impact rehabilitation outcomes.409–438 Motivation and support are crucial, as highly motivated patients with strong support networks adhere better to rehabilitation programs and achieve superior results. Rehabilitation specialists can enhance recovery by incorporating motivational strategies, providing psychological support, and involving family members or caregivers.409–416
Molecular effects of stress involve the hypothalamic-pituitary-adrenal (HPA) axis, which influences systemic inflammation and healing.417–420 Chronic stress activates the HPA axis, increasing cortisol levels, which suppress pro-inflammatory cytokines like interleukin-1 (IL-1), IL-6, and tumor necrosis factor-alpha (TNF-α) essential for wound healing.421–423 Elevated cortisol also reduces fibroblast proliferation and collagen synthesis by downregulating collagen genes and transforming growth factor-beta (TGF-β) signaling, impairing tissue integrity.424,425
Stress reduction strategies can mitigate cortisol’s negative effects on healing. Techniques such as mindfulness, cognitive behavioral therapy (CBT), and stress management interventions support mental well-being.426–429 Mindfulness reduces cortisol levels and enhances immune function, while CBT helps manage pain and adherence by altering negative thought patterns.430–433 Stress management practices like deep breathing and muscle relaxation promote endorphin release and reduce anxiety, further lowering cortisol levels.434,435
Social support plays a vital role in rehabilitation by boosting morale, providing practical assistance, and encouraging adherence to exercises and appointments.436–439 Positive interactions release oxytocin, which attenuates stress responses by inhibiting HPA axis activity and promoting relaxation.440,441 Engaging caregivers ensures consistent support, enhancing motivation and recovery.436–439
Impact on molecular healing processes includes the downregulation of growth factors like VEGF and TGF-β due to chronic stress, which impairs angiogenesis and fibroblast activation.442–444 Oxidative stress from chronic psychological stress generates reactive oxygen species (ROS), damaging cellular components and hindering tissue repair by inhibiting fibroblasts and keratinocytes.445–447 Antioxidant therapies and stress reduction techniques can reduce ROS levels and protect cellular integrity, enhancing healing.448–450
Epigenetic influences involve DNA methylation and histone acetylation, which alter gene expression related to inflammation and tissue repair.451–453 Chronic stress can hypermethylate anti-inflammatory genes like IL-10, reducing their expression and prolonging inflammation, while hypomethylation of pro-inflammatory genes like NF-κB exacerbates the inflammatory response.454–456 Assessing epigenetic markers allows clinicians to predict and adjust rehabilitation interventions, using nutraceuticals or pharmacological agents to optimize gene expression for healing.457–459
By addressing psychological and social factors through targeted strategies and understanding their molecular impacts, rehabilitation protocols can be more effectively tailored to support both mental well-being and physical healing, leading to improved outcomes and faster recovery.460–462
Discussion
In summary, tailoring rehabilitation protocols to individual patient characteristics significantly enhances recovery outcomes by addressing each patient’s unique needs.463–469 Factors such as age, activity level, graft type, molecular and genetic factors, and psychosocial aspects enable rehabilitation specialists to develop personalized programs that optimize healing, reduce complications, and ensure efficient recovery.
Molecular Biology Integration provides a robust scientific foundation for personalized rehabilitation. By incorporating genetic and molecular insights, clinicians can anticipate and address challenges in healing, such as variations in inflammation or tissue regeneration. Monitoring biomarkers like cytokine profiles, growth factor levels, and gene expression patterns allows for real-time adjustments to rehabilitation strategies, enhancing tissue repair and minimizing adverse effects.470
Psychosocial Management ensures patients remain engaged and motivated, improving adherence to rehabilitation protocols and outcomes. Reducing stress-induced cortisol levels through psychological interventions enhances immune function and accelerates molecular-level healing.471 Techniques such as mindfulness and cognitive behavioral therapy (CBT) support mental well-being and mitigate the negative impacts of chronic stress on tissue repair.
Advanced Molecular Techniques, including gene expression profiling and proteomics, monitor patient progress during rehabilitation.472 For example, tracking the expression of myosin heavy chain (MyHC) isoforms helps assess the effectiveness of strength training exercises, indicating muscle function and endurance improvements.473,474 Proteomic analysis of blood or tissue samples reveals changes in protein levels related to inflammation, tissue repair, and stress responses, providing a comprehensive view of the patient’s physiological state.475,476 Proteins like heat shock proteins (HSPs) indicate cellular stress and the effectiveness of recovery strategies.
By leveraging these advanced molecular tools, rehabilitation specialists can create highly personalized and scientifically grounded rehabilitation programs. This approach not only enhances the effectiveness of the rehabilitation process but also reduces the risk of adverse outcomes, promoting faster and more complete recovery for each patient.477–479

Conclusion
This review article emphasizes the essential role of early mechanical loading in improving the healing of anterior cruciate ligament (ACL) grafts, leveraging insights from molecular biology. It explains how mechanical stimuli during early rehabilitation influence tissue repair and regeneration at both cellular and molecular levels, providing a foundation for optimizing rehabilitation strategies and enhancing clinical outcomes after ACL reconstruction.
Key findings highlight specific molecular pathways activated by mechanical loading, such as the upregulation of growth factors like TGF-β and VEGF, which regulate collagen synthesis and angiogenesis through the Smad and PI3K/Akt pathways, respectively. Mechanotransduction involves integrins and focal adhesion kinase (FAK), triggering signaling cascades like MAPK/ERK that promote cell survival, proliferation, and differentiation. Additionally, mechanical loading improves collagen fiber alignment and extracellular matrix (ECM) integrity, essential for graft strength and functionality.
The article advocates for personalized rehabilitation protocols tailored to individual patient characteristics and graft types, enhancing healing by targeting specific molecular mechanisms. It calls for future research to identify precise molecular targets, explore genetic and epigenetic factors, and combine mechanical loading with therapies such as biological scaffolds and stem cells. By integrating molecular biology insights with clinical practice, ACL rehabilitation can become more effective and personalized, leading to better recovery times and long-term joint function.