Introduction
With the continuous advancements in pre-operative medical optimization, pain management protocols, and post-operative clinical pathways for primary hip and knee arthroplasty, there has been a significant reduction in post-operative pain and hospital length of stay.1–3 These improvements have led to significant policy change, such as Center for Medicare Services (CMS) removing the total knee and total hip arthroplasty in 2018 and 2020, respectively, from the inpatient only list. As a result, many surgeons have increasingly offered their patients same day discharge, also known as outpatient total joint arthroplasty (TJA) procedures in the ambulatory surgical center. The shift to outpatient arthroplasty has been extensively studied and can lead to better patient outcomes, better patient and surgeon satisfaction, and lower overall healthcare costs. While these benefits have already largely been accepted, implementing such processes in an already functioning academic hospital has scarcely been studied and necessitates a review of challenges specific to this particular setting.
How Did We Get Here?
Traditionally, TJA required an inpatient admission as the patient had yet to be optimized medically. This included pain control, access to multidisciplinary physicians during rounds, physical therapists, nursing staff, social workers, and consultant services. However, contrary to what one would expect, Andrews et. al found that inpatient hospital stays increased the likelihood of experiencing an adverse event by as much as 6% for each additional day of hospital stay. Furthermore, of their cohort, 18% of patients experienced a serious event that led to longer hospital stays and increased cost of care for the patient.4 It was factors such as these that began the push towards accelerated protocols to allow same day discharge TJA.
As described in Richardson et al.'s review of outpatient trends in TJA, in 2018, once CMS removed total knee arthroplasty (TKA) from the inpatient only list, there was a sudden surge in outpatient TKA prevalence, followed by an unfortunate decline due to the decrease in cases from the Coronavirus-19 pandemic. After resolution of the pandemic, the upward trend continued, and after removal of total hip arthroplasty (THA) from the inpatient only list in 2020, there was another surge with almost twice as many outpatient TJAs performed compared to years prior.5 For many academic centers, this was their first experience with outpatient arthroplasty as the initial post-Covid period was complicated by limited inpatient admissions for non-urgent orthopaedic conditions. As such, significant efforts were required to create systems and protocols that permitted safe same day discharge for TJA.
Inpatient versus Outpatient TJA: Is it Safe?
Regarding the safety of outpatient TJA, Wang et. al published an NSQIP database study with over 177,000 propensity-matched patients between 2005 and 2014 which found no significant differences in overall post-operative complications or readmissions between same-day discharge and inpatient TJA.6 The same group later published a single surgeon retrospective study of 970 patients matched 1:1 based on demographics, finding no significant difference in readmission rates, complications, visits to the emergency department, or unplanned clinic visits between inpatient and outpatient TJA groups.7 Anderson Orthopedic Research Institute took this a step further and conducted a prospective study to compare THA’s performed in their surgery center versus THA’s performed in the hospital outpatient department and found no differences in complications, revisions, reoperations, readmissions, or ED visits.8 They repeated the same study comparing surgery center versus hospital outpatient TKA’s and came to the same conclusion.9
Similarly, Bemelmans et al. published a meta-analysis in 2022 including 41 studies in which they found no overall difference in complication or readmission rates between inpatient versus outpatient TJA, concluding that outpatient pathways are safe and effective in select patient populations.10 Regarding patient perceptions of safety, a study by Meneghini et al. surveyed a single-surgeon’s cohort of patients, finding that 52% of patients thought that TJA in the Ambulatory Surgical Center (ASC) or hospital was equally safe, and 63% would rather recover from a TJA at home.11
As a strong limitation, the literature regarding safety of outpatient arthroplasty is largely from private ambulatory surgery centers or orthopaedic specialty hospitals. These centers are incentivized to perform their cases there due to ownership, which allows increased autonomy and ancillary revenue. As such, academic centers may not experience these same incentives and therefore may not see the benefits of shifting to the outpatient arena. Additionally, safety data from these specific practice models are lacking in the literature.
Why Move to the Outpatient Arena?
Ultimately, bringing TJA to the outpatient arena allows for improved patient outcomes, better patient and surgeon satisfaction, and lower overall healthcare costs. Outpatient surgery allows for the benefit of cost savings for the patient and the healthcare system, which is an important factor in a healthcare system known for its exorbitant costs. Aynardi et al. published a case-control study that shows that each outpatient TJA saves $6,000.12 These cost-savings are especially important when it comes to performing outpatient TJA at ASCs optimized for efficiency and value-based care. Additional advantages of ASCs include efficient workflow with faster OR turnover times, increased surgeon satisfaction, and the opportunity for ancillary income in light of decreasing reimbursements for TJA. These advantages are imperative given that burnout is at an all-time high and reimbursements for TJA are decreasing. Further, the opportunity for surgeon buy-in and ASC ownership incentivizes surgeons to perform efficiently.13,14 Physician ownership has been studied by Cho et al. in a systematic review looking at physician-owned hospitals before 2008, showing that when physicians own the hospital they make better decisions in terms of cost and quality.15
These benefits of outpatient TJAs at ASCs have been well studied, however when transitioning to outpatient TJAs at a university or academic medical center, with employed or RVU based academic positions, there may not exist as much pressure to produce cost savings. This is especially the case with the increased administrative burden required for successful selection and scheduling of outpatient TJA.
Increased Burden to Make it Work
In order to make outpatient TJA successful, the healthcare system as a whole has to be involved in making the experience an efficient and streamlined process. It is well known that for successful outpatient TJA, there exists a larger burden of pre-operative work on administrative and ancillary staff. Berger et al. quantified this burden, describing that for 100 patients discharged within 5 hours of entry into the post-anesthesia care unit (PACU), there were 250 phone calls required.16 Our group has previously published data on Time Driven Activity-Based Costing, quantifying that each TJA patient had 8.5 hours of unaccounted for work.17 In the year 2020 alone, that was $1.5 million of preoperative work that was completed but not reimbursed.17 Thankfully, policymakers responded to this issue and there now exists potential for reimbursement through principal care management codes. They have acknowledged that this pre-operative administrative burden needs to be reimbursed for continued efficacy of outpatient TJA, and there is potential for both the provider as well as ancillary staff to bill appropriately for these services which are conducted outside of a direct patient encounter.18 If there exists no external incentive or pressure for surgeons to practice with this efficiency in mind, they may not choose to conduct this extra work to transition their patient practice to outpatient arthroplasty.
Pre-Operative Medical Optimization
One of the key factors to success in outpatient TJA is pre-operative optimization of each patient. For patients to be as ready for surgery as they can be, a strong relationship with medical consultants is required by the practice, as well as the shift of mindset to disease as a spectrum of pathology instead of a series of “cut–offs”. Additionally, there are psychosocial factors at play for patient preparedness for surgery and for optimizing recovery that need to be discussed. With a close network of support from the medical field at academic medical centers, this is one area where they may be extremely well equipped to deliver high quality pre-operative medical optimization. Commonly discussed areas for medical optimization for TJA patients include weight and BMI, nutrition and diabetes, and smoking optimization.
It is well known that patients with high body mass index scores (BMIs) have worse outcomes in TJA, which has largely led to institutional cutoffs. Many cutoffs are around 40 kg/m2 stemming from a study published in Acta Orthopedica, showing that patients with a BMI between 35 kg/m2 to 40 kg/m2 have 2 times the relative risk of complications after TJA compared to patients below a BMI of 35 kg/m2.19 Furthermore, patients with a BMI greater than 40 kg/m2 are at 4 times the risk of complications. There have been several studied reasons, including underdosing of antibiotics, increased technical difficulties with the surgery, and even lack of appropriate nutritional status for the healing process despite higher BMIs.19
It is also well known that patients with diabetes have worse outcomes in TJA, which has also led to institutional cutoffs of Hemoglobin A1C. This research continues to evolve, including the advent of a newer lab marker, fructosamine, which reflects the blood glucose levels over the past 2 to 3 weeks. There is data to support that a fructosamine level above 293 µmol/L is associated with a higher risk of periprosthetic joint infection (PJI).20 In addition, our group found that pre-diabetes was also risk factor for post-operative complications, including respiratory failure, anemia, hypertension, and infection.21 As such, it can be argued that relying solely on Hba1c for institutional cut-offs is inadequate for determining surgical optimization. There has also been extensive research for nutritional optimization, including recommended defined values of albumin, absolute lymphocyte count, Vitamin D and zinc, each with defined nutritional interventions that can be prescribed.22
Additionally, there is published data that supports the idea of smoking being thought of as a spectrum of disease. Bedard et al. conducted a meta-analysis comparing the rate of PJI and wound complications in THA between former tobacco users and non-tobacco users. When compared to never smokers, former tobacco users had a higher odds ratio for complications, and current smokers were at a higher risk of complications than former smokers.23 Smoking history can be gathered from patients but smoking cessation can also be monitored with serum cotinine levels, with a value higher than 8 ng/mL indicative of a current smoker. This is highly recommended in the smoking population, as 15% of patients that claim to have quit smoking will have one positive test result.24
The list of factors for optimization continues, with evidence demonstrating that having multiple allergies is a risk factor for increased complications, and evidence demonstrating that adequate social support networks can ensure same day discharge for TJA, ensuring comfortable recovery at home.25–27
Within the conversation of medical optimization, there is also a conversation to be had regarding the ethics of delaying TJA for improved patient risk modification. Although there is no mortality associated with a delayed TJA, there certainly is increased suffering for the patient. This was commented on by Bronson et al. who concluded that there exists a balance between indefinite delay of a pain-reducing procedure and increased risk of morbidity from a procedure on a non-optimized patient.28
Academic hospitals serve as referral centers from the community and normally accept a more complex patient population which requires an emphasis on preoperative optimization. Despite academic medical centers having abundant resources and multidisciplinary teams at their disposal to enable them to implement such strategies for preoperative optimization, they lag behind in adoption of the ASC mentality of preoperative optimization and familiarity of postoperative care.
Patient Selection Criteria
There has been a substantial amount of work dedicated to creating a simple scoring system for appropriate patient selection for outpatient TJA. This largely includes the analysis of preoperative comorbidities as discussed above. The idea of a scoring system dates back to the original American Society for Anesthesiologists (ASA) classification which is frequently used when determining preoperative risk. However, this classification comes from a 1978 study with a poor response rate from practicing anesthesiologists and when looking at the data, there was also poor consensus for their classification criteria.29
An improved example of such scoring system is the outpatient arthroplasty risk assessment score (OARA) developed by Meneghini et al.11 This proprietary software system comprises 9 comorbidity areas, each containing specific medical conditions, with a resulting score of less than 59 indicating that the patient is safe for same-day discharge. OARA has high positive predictive value for assessing patients eligible for outpatient arthroplasty, but low sensitivity.11 The OARA score was further studied for validation by Crawford, Lombardi and Baron in their retrospective review of 1,300 TJA patients, finding that 97% of patients with “failing” OARA scores of greater than 59 were successfully discharged the same day after TJA. Of their 23 TJA patients that required inpatient admission, only 30% of them were deemed “acceptable” by the OARA score. After analyzing their patients, the authors in turn developed their own simple, elegant and effective algorithm for determining candidacy for outpatient TJA.30 Ultimately, their take-home message was that their contraindications for outpatient TJA are those with comorbidities that cannot be optimized: heart failure, valvular disease, COPD, sleep apnea with increased BMI, renal disease, anemia, stroke, delirium, or solid organ transplant.31
Why Do Same-Day Discharges Fail?
Importantly, ASC’s do not have the same resources as hospitals do, so failure of outpatient TJA in many cases is not an option. Goyal et al. won the Otto Aufrank award for their multi-center randomized study looking at inpatient versus outpatient THA and reasons for failure of same day discharge. This study showed that in the 220 included patients, there was no difference in VAS pain and other post-operative metrics between inpatient and outpatient THA. However, 24% of patients in the outpatient cohort were unable to be discharged the same day for the following reasons: hypotension 33%, pain 22%, patient preference 19%, nausea 15%, failing physical therapy (PT) 7%, and post operative urinary retention (POUR) 4%.32 Fraser et al. published another study with the same goal of identifying the reasons for failed same-day discharge, demonstrating that 26% of patients who were identified as candidates for same-day discharge failed. Their reasons included: patient preference 43%, hypotension 29%, failed PT 18%, POUR 7%, and pain 4%.26
As demonstrated above, an important factor preventing same day discharge is post operative hypotension. It is estimated that up to 25% of THA patients and 11% of TKA patients experience postoperative hypotension.33 Important contributing factors include opioid use for pain control and blood loss during surgery. After those have been optimized, it has been shown that administration of steroids, which act as an anti-inflammatory and depress vagal activity, can improve hypotension.34 Another medication, ondansetron, counteracts the sympathetic block from the spinal anesthesia that causes hypotension and bradycardia through peripheral serotonin receptor activation.35
Although POUR is an important delay to discharge, it must be noted that per the urology guidelines, post operative urinary retention is not an indication for inpatient admission.36,37 Important risks include spinal anesthesia, use of opioids, elderly males with pre-existing symptoms, increased intra-operative time (25% increased risk with every 15-minute increase in the operating room), delay in post-operative ambulation, and administration of intraoperative fluids in a dose dependent manner.38 If POUR does happen, administration of bethanechol or tamsulosin been shown to be effective.39–43 If POUR occurs a second time, insertion of a foley with urology outpatient follow up for trial of void is indicated.
Importantly, having access to an easy transition to inpatient admission risks having misaligned perspectives from team members and patients, which may convince the patient they would be better off monitored in the hospital with an admission. This is another factor that comes in to play when specifically looking at the academic medical center setting for transitioning towards outpatient TJA.
Protocols to Optimize Same Day Discharge After TJA
After pre-operative factors such as comorbidities, patient preference, psychological factors, and social support for the patient have been optimized, there exists 4 predictable physiologic disturbances that adversely impact rapid recovery: volume, blood loss, nausea, and pain.
Regarding volume, there is a well-conceived notion that patients should be “nil per os”, known as NPO, after midnight. However, there is evidence-based data demonstrating that you can safely consume clear liquids with carbohydrates up until 2 hours prior to surgery, which has demonstrated no effect on gastric volume, gastric pH, aspiration risk, or regurgitation risk.44 Importantly, in a cohort of patients who presented for surgery following the above protocol and then NPO 2 hours prior to procedure, patients were less hungry, had less nausea, and had less pain.45 In addition, following this above protocol allows for better volume balance in the peri-operative setting, avoiding hypotension, dizziness, and post-operative urinary retention.
Regarding reduction of blood loss during surgery, the three commonplace strategies include optimization of pre-operative anemia, permissive hypotension, and administration of Tranexamic Acid (TXA). Tranexamic acid competitively inhibits the conversion of plasminogen into the active form of plasmin, which in turn degrades fibrin products and is considered an antifibrinolytic, with no thrombogenic nature. Taeuber et al. published a systemic review containing 216 randomized controlled trials, concluding that there is no increased risk of thromboembolic events when administering TXA.46 Sabbag et al. also showed that TXA was safe to administer in patients with history of a blood clots.47 It is imperative to have this discussion pre-operatively with the anesthesia team for the safe administration of this medication to reduce blood loss during the surgery.
Perioperative Analgesia in Total Joint Arthroplasty
Other peri-operative protocols that favor same-day discharge are the use of spinal anesthesia and use of propofol instead of inhalation agents, both critical for reducing post-operative nausea and vomiting (PONV) and promoting same-day discharge. One-shot spinal anesthesia using either bupivacaine, mepivacaine, or lidocaine results in fewer complications, no increased risk of pneumonia, fewer falls, less thromboembolic disease, and shorter OR times.48,49 Spinal anesthesia administered with a sedative, such as propofol, has been shown to have an excellent length of action and lower side effect profile as compared to midazolam and dexmedetomidine.50
As far as prophylaxis for PONV, the protocols have now evolved to administering dexamethasone, which can have an antiemetic effect and an analgesic effect at a more potent dose, as well as ondansetron. In those with a history of PONV, a scopolamine patch has shown to be effective at mitigating symptoms.51,52
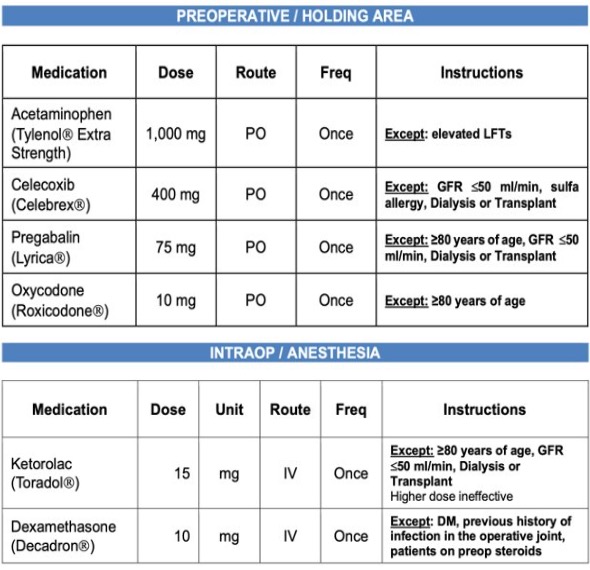
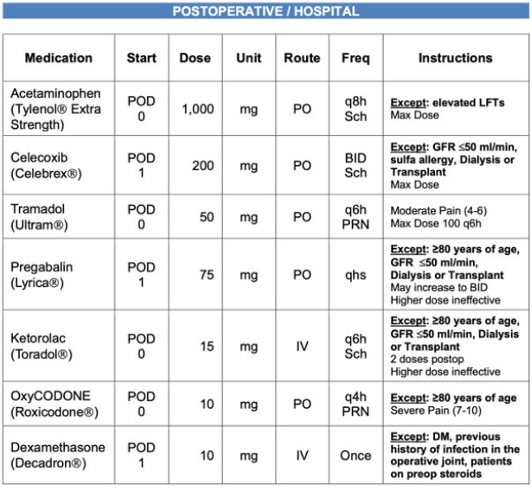
Peri-operative pain management in the arthroplasty population has also had remarkable advancements, emphasizing a multimodal pain approach and preemptive analgesia with a more sparing use of opioid medications which have been shown to delay same day discharges after TJA.53 Figures 1 and 2 give an excellent summary of the recommended regimen in an organized pathway that has been shown to promote better pain control and same day discharge. Notably, while pre-operative oxycodone can assist with post-operative pain control, there are some institutions which entirely avoid pre-operative opioids, which is a further advancement in the multimodal pain regimen pathway.


As part of the multimodal analgesia regimen, many institutions employ an adductor canal block, and there is evidence to support infiltration of an anesthetic between the popliteal artery and capsule of the knee (IPACK), which demonstrates lower pain scores, lower patient usage of opioids, and faster discharge.54 Unfortunately, IPACK comes with the potential complication of foot drop, which may hamper same day discharge. Regarding the best nerve block for THA, there are three main methods which are being reviewed in the literature for efficacy, including fascia iliaca block, quadratus lumborum block, and erector spinae block. Although these can assist with post-THA analgesia, THA patients also do fairly well without nerve block. Another aspect of the multimodal approach is the periarticular injection, for which there is no definitive consensus.
Conducting consistent protocols at an academic center is feasible given the consortium of highly skilled team members present within the hospital setting. However, challenges at an academic center include lack of consistency in regards to anesthesia and surgery personnel. The use of established protocols and appropriate training prior to change of personnel is imperative for success and standardization of care.
Outpatient Arthroplasty at the Ambulatory Surgical Center versus Academic Center
Efficiency in outpatient arthroplasty is about maximizing patient outcomes and surgeon productivity while decreasing the use of hospital resources. However, an important consideration with decreased use of hospital resources is adequate preparation for emergent situations. This includes quick availability for intra-operative instruments and augmentation, such as backup trays, cables, diaphyseal engaging stems or plates for diaphyseal femur fractures, readily available cementing materials, suture anchors, constrained implants, and much more. This also includes established protocols for emergencies, such as vascular injuries that require urgent vascular consultation or transfer to a center with on call vascular surgeons. Such situations are rare, however, the availability of these instruments and assistance is vastly different at the ambulatory center versus the academic center. The academic facilities provide a certain “safety-net” of ease of admission if needed, ease of access to advanced instrumentation, and rapid access to consulting services on-site if required.
Organizational differences in an academic center as opposed to a stand-alone ambulatory surgical center or specialty specific hospital setting lead to certain challenges in implementing outpatient arthroplasty strategies. DeCook et al. reports on the emphasis of efficiency at ambulatory surgical centers and the challenges of changing culture within the hospital setting.55 One such challenge is the multitude of bureaucratic layers and the significant amount of time required for significant change to be instituted. Such limitations are avoided in physician-centers, and often with reduced administrative bloat.
Tertiary referral academic centers have tremendous volume, variety of procedures, and call to attend to, not only for non-orthopaedic services but also for unplanned presentations through the emergency room that require admission for operative intervention, such as PJI. Academic centers are also known for their training, leading to variability in team members and frequent change. Similar principles apply to the variety of anesthesia staff at the academic medical centers assisting with the case, versus the select few that work within an ambulatory surgical center. These various factors hamper the efficiency of an outpatient joints practice. In contrast, ambulatory surgical centers are more likely to have dedicated staff who become familiar with arthroplasty procedures, leading to less variability, consistency, and efficiency.56,57 In addition, given the leadership structure at ambulatory surgical centers, the cost savings and efficiency improvements come to realization more quickly. Surgeons with ownership stake in ASCs are financially motivated to play crucial roles in each process from case start times, turnover times, implant costs, and more.
One avenue that portends an advantage at an academic center is judicious use of technology and the ongoing research efforts. Often, academic support provides capital resources that can be invested in outpatient arthroplasty protocols and technological advancements within the department. That being said, it is imperative that all technological advancements and additions to the practice are made with the value formula in mind. Implementation of technology will always increase the cost but does not always improve quality. For this reason, structured analysis is needed to compare the costs, benefits, and outcomes after implementation of technology. One such example demonstrated that robot assisted TKA compared to controls had lower perioperative complication rates and shorter lengths of stay, but cost an additional $1,000 for the patient.58
In conclusion, throughout this review we have understood the importance and impetus to bring total joint arthroplasty to the ambulatory surgical center, which ultimately benefits the patients. We have applied evidence-based principles to develop, first and foremost, appropriate patient selection criteria, and second of all appropriate perioperative protocols to improve patient outcomes and safe same-day discharge. Lastly, we have discussed the unique position that academic centers are in within the outpatient arthroplasty space and considerations for moving forward.
Author Contributions
David Constantinescu- wrote manuscript, involved in study design, data acquisition and analysis, drafting and the final review of the manuscript prior to submission.
Gilberto Lobaton- wrote manuscript, involved in study design, data acquisition and analysis, drafting and the final review of the manuscript prior to submission.
Jordan Eskenazi- wrote manuscript, involved in study design, data acquisition and analysis, drafting and the final review of the manuscript prior to submission.
Aneesh Samineni- wrote manuscript, involved in study design, data acquisition and analysis, drafting and the final review of the manuscript prior to submission.
Victor Hernandez- wrote manuscript, involved in study design, data acquisition and analysis, drafting and the final review of the manuscript prior to submission.
Disclosures
Victor Hernandez: AAHKS: Research support| AAOS: Board or committee member| American Association of Hip and Knee Surgeons: Board or committee member| American Association of Latino Orthopaedic Surgeons: Board or committee member| DePuy, A Johnson & Johnson Company: Paid consultant| Enovis: Paid consultant |Miami Orthopaedics Society: Board or committee member |OMEGA: Research support |OREF: Research support |Zimmer: Paid consultant