Introduction
The prevalence of chronic knee pain has increased dramatically over the past two decades, leading to growing functional limitations, mobility issues, and a reduced quality of life.1 An aging population, rising obesity rates, and the growing burden of osteoarthritis that accompanies changes all contribute to this profound change.1 Management strategies for pain control include conservative management with physical therapy and oral medications, minimally invasive treatments such as intra-articular injections, genicular nerve blocks and ablations, and surgically invasive treatment being total knee arthroplasty (TKA) for advanced, treatment-resistant osteoarthritis.1 The functional limitations, mobility challenges, and reduced quality of life that persist in lieu of these therapies have led to a pressing need for more effective management strategies. While TKA is generally effective in relieving pain and restoring function, a notable proportion of patients continue to suffer from persistent pain after TKA.2 There is a need for interventional treatments that provide long-term pain relief, as commonly used options such as genicular nerve blocks and radiofrequency ablation offer results for a limited-duration and face coverage barriers.3–7
Peripheral nerve stimulation (PNS) is an innovative pain management modality for patients that offers a promising alternative for those suffering from chronic knee pain due to osteoarthritis and post-TKA pain. PNS functions by delivering electrical impulses to a target nerve. The quality and intensity of the stimulation is dictated by inputted parameters such as frequency, amplitude, and pulse width.8 A power source generates the impulse for stimulation thereby delivering electrical current to helically coiled electrical leads, which go on further to apply this current to afferent sensory neurons.9 This approach has gained increasing attention and relevance as a potential therapeutic option, not only for those with chronic pain following TKA but also for individuals suffering from non-operable osteoarthritis and other lower extremity pain conditions.10–13
Chronic knee pain often involves both nociceptive and neuropathic components. Nociceptive pain in osteoarthritis is driven by multiple etiologies including inflammation, synovial irritation, and cartilage degradation.14 In both osteoarthritic knee pain and post-TKA states, nerve damage and/or sensitization play a significant role in mediating neuropathic pain as well.8 PNS is uniquely positioned to address both types of pain. Romer et al. identify distinct structural phenotypes of knee osteoarthritis including inflammatory, meniscus-cartilage, subchondral bone, atrophic, and hypertrophic.15 They are distinguished by some of the aforementioned pathologies. Given the heterogeneity of osteoarthritis, a one-size fits all approach may not provide equal pain relief across the different subgroups of patients. PNS serves as a customizable therapy that influences various pain pathways. However, further investigation is necessary to more accurately determine how PNS affects these different subgroups of patients. A recent randomized placebo-control trial of a 60-day PNS treatment for post-operative knee pain not only reports on the significant pain relief outcomes, but goes on to demonstrate that walking distance was significantly improved in the treatment arm as well.16
The growing body of evidence supporting PNS suggests it may serve as a valuable alternative for patients whose pain persists despite other conventional options, and as it relates to quality of life and functional outcomes. We present the outcomes of two experienced interventional chronic pain physicians utilizing the 60-day percutaneous PNS to treat chronic knee pain.
Methods
Study Design
This is a retrospective cohort study using database and chart review aimed at evaluating the effectiveness of a 60-day PNS system for managing chronic knee pain.
Data Source
Data were sourced from the device manufacturer’s database, which contained treatment records including targeted pain areas, treatment outcomes, and patient-reported relief following 60-day PNS therapy from two experienced interventional chronic pain physicians. For comparison, twelve patient charts were reviewed as a control group from the same time period. These patients received conventional medical management, as outlined below, but did not undergo 60-day PNS therapy.
Patient Selection
Patients included in this study were ≥18 years of age with chronic knee pain due to osteoarthritis or persistent post-total knee arthroplasty (TKA) pain. Eligible patients had failed conservative medical management (CMM), including but not limited to physical therapy, NSAIDs, acetaminophen, and interventional options including diagnostic and therapeutic genicular nerve blocks and/or radiofrequency ablation (RFA). All patients in the treatment group received 60-day PNS treatment between October 1, 2019, and September 30, 2024. Twelve patients with chronic knee pain due to osteoarthritis or persistent post-TKA pain were treated with only CMM were included as the control group. Propensity score matching was not performed given the low number of patients in both groups and only descriptive statistics were used.
To ensure procedural consistency, all cases were performed by two experienced interventional pain physicians (JH and GC) with significant experience performing PNS therapy. Target nerves were selected based on pain patterns and clinical judgment. Procedures were performed under image guidance (fluoroscopy or ultrasound) according to physician preference and nerve targets. This consistency in technique minimized operator variability and ensured comparability of outcomes across cases.
Device Description
The device used in this study was the SPRINT PNS system (SPR Therapeutics Inc., Cleveland, OH). It consists of a percutaneous, coiled lead that is implanted under image guidance without the need for surgical incision or permanent implantation. The system is designed for temporary use over a 60-day period, after which the lead is removed. Its minimally invasive nature allows for outpatient implantation and removal, contributing to its favorable safety profile and ease of clinical use.
Data Collection and Analysis
The data collected for this study includes:
-
targeted area of pain (i.e., knee pain)
-
responder status (defined as those treated who achieved ≥ 50% of pain relief)
-
percentage of pain relief in the responders (method to assess overall effectiveness).
Ethical Considerations
This study is a retrospective analysis of data from a device manufacturer’s database. A control group was included, consisting of patients with similar pain complaints who did not receive 60-day peripheral nerve stimulation (PNS) therapy. Only treatment outcomes were collected, and no identifiable patient information was accessed. All data were deidentified and the analysis focused exclusively on outcomes. Furthermore, the study was conducted in accordance with the principles outlined in the Declaration of Helsinki, ensuring adherence to all ethical guidelines for research involving human data.
Results
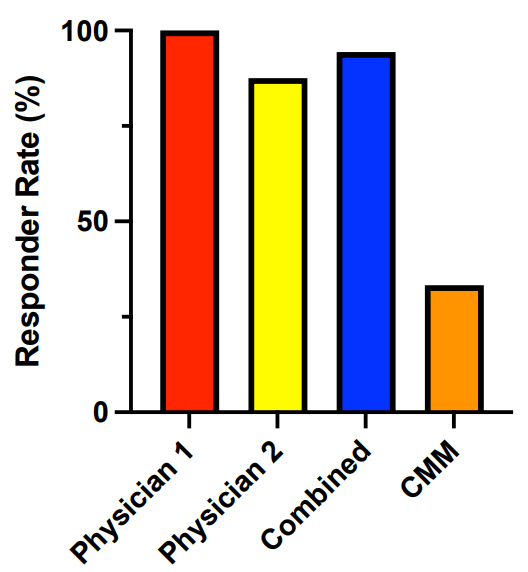
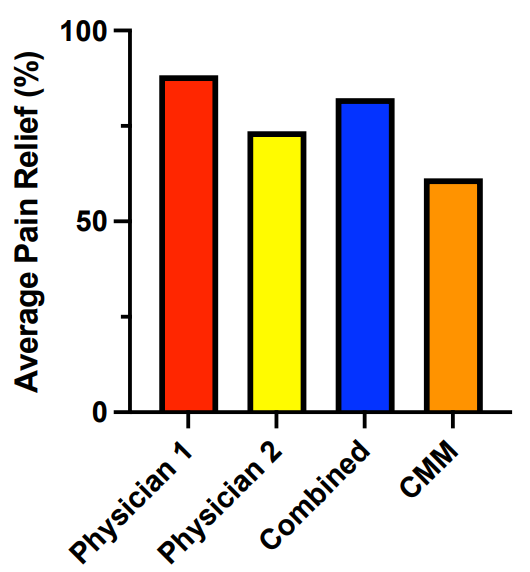
This retrospective chart review analyzed the outcomes of 18 patients who underwent 60-day PNS therapy for chronic knee pain treated by two experienced interventional chronic pain physicians. Detailed evaluations of their response rates and average pain relief following PNS placement was assessed.
Physician #1 treated 10 patients with 100% (10/10) being responders with the weighted average pain relief from baseline being 88.3% (Figure 1 and 2). Physician #2 treated 8 patients with 87.5% (7/8) being responders with the weighted average pain relief from baseline being 73.6% (Figure 1 and 2). The overall responder rate across the 18 patients was 94.4% (17/18) (Figure 1). The weighted average pain relief among all responders was 82.3% (Figure 2). In the CMM group, 33.3% (4/12) of patients were responders. Of the four patients who were responders, the weighted average pain relief was 61.3%.
_for_each_physician_and_combined_af.png)

Discussion
This retrospective database and chart review study highlights the potential of 60-day PNS as an effective treatment modality for chronic knee pain. The findings of our study, notably the high responder rate (94.4%) and average pain relief among responders (82.3%), underscore the utility of this therapy in providing adequate and meaningful relief for patients who have not achieved such with other conventional treatments (i.e., medication, physical therapy, surgery). The results of this study support previous research demonstrating the benefits of neuromodulation for chronic knee pain management.11,17–21 A systematic review by Lin et al. on the topic of US-guided PNS for knee pain exemplifies how PNS is an effective treatment option for a wide breath of knee pain etiologies, including pre- and post-TKA patient populations as well.22 The rise of ultrasound guidance has enhanced the precision of electrode placement by allowing for more accurate targeting of specific neural structures. Additionally, fluoroscopy can also be utilized for certain nerve targets, such as the genicular nerves, offering another reliable imaging modality for procedural guidance.
Furthermore, 60-day PNS offers a non-pharmacologic and minimally invasive alternative to long-term opioid therapy, which remains a significant concern due to the risks associated with dependence, addiction, and overdose. Given the illicit opioid crisis, the availability of effective non-opioid treatments such as PNS is increasingly important for both patients and healthcare providers. Previous research indicates that PNS may reduce the need for opioids thereby minimizing the risk of opioid-related adverse effects.23 In a clinical retrospective multicenter trial looking at 25 post-TKA patients who underwent a landmark-guided implantation of a PNS system targeting branches of the saphenous nerve, subjects were able to significantly reduce their opioid medication from a median of 80 morphine milligram equivalents (MME) preoperatively to 20 MME at 3- and 6-months post-implant.24
60-day PNS can be a viable option for patients who are not surgical candidates or for those who have failed traditional interventional approaches and pharmacotherapy. It may be particularly beneficial for individuals who have not achieved adequate or sustained relief following genicular nerve blocks and RFA. Of note, it is important to carefully consider timing when selecting PNS candidates, as placing PNS on the same nerve targets immediately after neurodestructive therapies such as RFA may reduce its efficacy.19,25 In contrast, there is evidence to support the concept that PNS may be more beneficial when introduced earlier within the treatment paradigm. A systematic review by Previtali et al. describes different pain trajectories in knee OA patients, high-lighting the need for the early introduction of effective management strategies to alter a potentially unfavorable pain course.26 Patient outcomes may improve if PNS, traditionally reserved for refractory pain, is introduced earlier in the treatment algorithm. This could have downstream effects on altering the natural history of chronic pain in addition to preventing central sensitization. In a prospective case series by Gilmore et al., the authors discuss PNS within the context of treating chronic low back pain, but note that the benefits of earlier introduction of PNS into the treatment plan may obviate the need for permanent implantation of a stimulator in addition to providing an alternative to other treatment strategies such as chronic opioids, neurodestructive procedures (RFA) and surgery.27 In a recent survey of 94 interventional pain physicians in practice, most respondents (77%) answered that they would utilize PNS to treat nociceptive pain from major joint osteoarthritis.28 Interestingly, a range of 50-85% of respondents would not change their current utilization of PNS on encountering a range of minor adverse events including soft-tissue reactions, minor infection, and lead migration or loss of efficacy while a range of 41-58% of respondents would reduce their utilization with more significant adverse events such as skin erosion, major infection, or lead fracture.28 Cost-effectiveness, patient selection, and potential risks (while minimal) may all preclude widespread adoption of the practice of introducing PNS earlier in the treatment continuum.
Optimal patient selection and procedural planning are essential to maximizing the therapeutic benefits of PNS in managing chronic knee pain. Studies within the context of SCS have shown that the psychological component to pain may have a substantial impact on treatment efficacy.29 This insight is also relevant to PNS for chronic pain and highlights the value of incorporating psychological assessments to optimize patient selection and treatment efficacy. However, for temporary 60-day PNS therapy, psychological testing is not routinely performed by our physicians. This approach is based on the temporary nature of the device, its low-risk profile, and the fact that it is fully reversible. If a patient later chooses to pursue a permanent neuromodulation system, psychological clearance is then obtained as part of the standard pre-implant evaluation process.
More recent research also examines the significance of patient education in the management of chronic knee pain. A recent randomized control trial including 80 patients conducted in Southern Iran evaluated the impact of self-care education on osteoarthritic knee pain.30 The notable reductions in pain intensity and improved quality of life in this group underscores the role of integrating patient education into a PNS therapy plan. Increasing engagement and adherence with the therapy may lead to optimization of long-term results.
Of importance, no patient in our study experienced a significant adverse event or complication related to the placement or function of the PNS device. This finding is consistent with the broader literature on PNS, which has consistently reported low rates of complications and high patient satisfaction.22 The minimally invasive nature of PNS and its reversibility, notably the ease with which it can be discontinued, contribute to its favorable safety profile. This added layer of safety and flexibility affords prompt resolutions to concerns as they arise.
Limitations
This study has several limitations that should be considered when interpreting the findings. Firstly, as a retrospective review, this study is inherently limited by the quality and completeness of the available data as obtained from the device manufacturer’s deidentified outcomes database. As such, important clinical variables such as patient age, gender, functional recovery metrics, and analgesic medication usage before and after the 60-day PNS therapy were not available for analysis. A prospective randomized study would allow for the gathering of additional data, reduce potential biases, and support the evaluation of other secondary endpoints. Another limitation of this study is the reliance on patient-reported percentage of pain relief as the sole outcome measure. Although this metric offers a standardized approach to assessing perceived pain intensity, it does not encompass other important dimensions of treatment impact, such as improvements in physical function, daily activity level, or overall quality of life. Due to the retrospective nature of the study and the constraints of the database, other outcome measures such as functional scores or patient-reported outcomes were not available. Future prospective studies should incorporate a more comprehensive set of validated tools.
Additionally, the generalizability of these findings is limited by the small sample size (n=18) and the use of data from only two interventional pain physicians. However, both physicians are experienced neuromodulators who routinely incorporate PNS into their clinical practice, ensuring appropriate patient selection and consistent treatment application. This study serves as a pilot analysis to evaluate early outcomes of chronic knee pain with 60-day PNS therapy.
A multi-center, prospective study with a larger and more diverse cohort is needed to validate these findings and improve generalizability. The physicians in this study primarily targeted the superomedial and superolateral genicular nerves, but other targets seen in practice may include the infrapatellar saphenous nerve or branches of the femoral and sciatic nerves.
The absence of long-term follow-up data represents another key limitation of this study. Pain relief and response rate was assessed within the 60-day treatment period of the PNS device, however there is a paucity of data on the long-term benefits of the therapy and if it reliably persists beyond this time frame. Furthermore, while the data were collected from a manufacturer-managed database, the outcomes reflect real-world clinical practice by experienced interventional pain physicians whose patients were included in this analysis. Nonetheless, we acknowledge the potential for reporting bias inherent in manufacturer-managed datasets and emphasize the need for future independently conducted studies using objective and standardized outcome measures to validate these findings.
Conclusions
The significant pain relief and high responder rates observed in this study, along-side prevailing literature, support the inclusion of neuromodulation in modern treatment algorithms for chronic knee pain, particularly for patients at risk of surgical complications or challenged by long-term opioid dependence.31 As our understanding of chronic pain mechanisms continue to be elucidated, PNS may play an increasing role in the multidisciplinary management of a variety of chronic pain issues. With the increasing evidence to support PNS as a modality for treating knee pain, the authors of this study hope to stimulate future discussion for updates to multidisciplinary guidelines.32 This certainly includes the ability to offer meaningful relief and improvements in function and quality of life for those with chronic knee pain. The findings of this study highlight the promise of 60-day PNS therapy as an effective intervention, with the majority of patients experiencing substantial benefits. However, further research is needed to better understand the variability in patient outcomes and to evaluate the long-term effectiveness of this approach. In addition, independent studies, outside of manufacturer-supported databases, are also encouraged to assess PNS outcomes more broadly.
Author Contributions
Conceptualization, Jamal Hasoon; Data curation, Alexander Rothkrug and Christopher Robinson; Formal analysis, Jamal Hasoon, Alexander Rothkrug and Christopher Robinson; Investigation, Alexander Rothkrug and Christopher Robinson; Methodology, Jamal Hasoon and Christopher Robinson; Project administration, Jamal Hasoon and Christopher Robinson; Resources, Jamal Hasoon; Supervision, Jamal Hasoon and Christopher Robinson; Writing – original draft, Jamal Hasoon, Alexander Rothkrug and Christopher Robinson; Review & editing, Grant Chen and R. Yong.