1. Introduction
The Achilles tendon plays an essential role in the biomechanics of the human body, being primarily responsible for the transmission of force between the calf muscles and the foot. This tendon is formed by the tendinous portions of the gastrocnemius and soleus muscles (tricipitis surae), which join distally to form a single structure inserted into the calcaneal tuberosity. Thus, it is responsible for the plantar flexion and inversion movements of the foot, and also aids in knee flexion.1
The prevalence of injury has increased, especially among middle-aged individuals who practice recreational sports, due to the high mechanical stress on the tendon, which makes it vulnerable to ruptures and injuries. According to a study by Suchak et al. (2005),2 the incidence is estimated to vary between seven and 40 cases per 100,000 inhabitants, being more common in males and in those aged between 30 and 40 years. According to Lemme et al. (2019),1 the annual incidence varies between six and 18 cases per 100,000 inhabitants.
According to Ganestam et al. (2015),3 Achilles tendon injuries have been increasing due to population aging. The etiology of Achilles tendon rupture is considered multifactorial and is often associated with pre-existing degenerative changes at the site. In high-impact injury mechanisms, the triceps surae muscle is subjected to an eccentric load before explosive acceleration or change of direction. In this process, the Achilles tendon stores elastic energy that subsequently assists in the propulsion of the movement.
During intense contraction of the triceps surae, plantar flexion of the foot occurs, allowing the necessary momentum for movement. At this time, there is a significant distribution of forces on the Achilles tendon, which can reach six to eight times the individual’s body weight, which can result in injuries.4 Injuries can result in severe pain, significant functional limitations and a negative impact on quality of life, making mobility and resuming daily and sports activities difficult.
On examination, edema, bruising in the ankle region and a palpable gap at the level of the injury are most often noted. As for tests, the literature describes the Thompson test, which has a sensitivity of 96% and a specificity of 93%. The knee flexion test has a sensitivity of 88% and a specificity of 85%. In addition, there are other tests used for diagnosis.5
With the increase in the number of Achilles tendon injuries, there is much debate about the ideal treatment or gold standard, between conservative and surgical options. Recent literature addresses an increase in minimally invasive surgical techniques, studies of conservative techniques and a focus on quality rehabilitation to reduce the risk of a new rupture.6 Thus, the question is: “Between conservative treatment and surgical treatment for Achilles tendon injuries, which approach presents better clinical and functional outcomes, considering the rate of re-rupture, functional recovery and adverse events?”.
Thus, the systematic literature review aims to compare conservative treatment and surgical treatment for Achilles tendon injuries, analyzing the rates of re-rupture, functional recovery and occurrence of complications.
2. Materials and Methods
The study is a systematic literature review, constructed according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Therefore, the PICO strategy was used to produce the results. The acronym PICO represents an acronym for Population, Intervention, Comparison and Outcome. In this sense, the following were used:
-
P (Population): Patients with Achilles tendon injuries.
-
I (Intervention): Conservative treatment.
-
C (Comparison): Surgical treatment.
-
O (Outcome): Rerupture rate and other outcomes.
The search was then carried out in February 2025 in the databases linked to the Medical Literature Analysis and Retrieval System Online (MEDLINE). Using the Health Sciences Descriptors (DeCS)/Mesh terms, in a combined form: Achilles tendon; Conservative treatment.
The descriptors were adjusted in different ways in order to broaden the search for studies. Terminological variations were considered, as well as synonyms, and were used to perform a qualified search using Boolean operators.
Articles published between 2015 and 2025 were included in the study, with full access to the study, which answered the research question and the highlighted objectives.
In addition, only original studies were selected, including those that used randomized clinical trials, observational studies, cohort studies, or controlled clinical trials as their method, which compared conservative treatment and surgical treatment in patients with Achilles tendon injuries. Studies published in English, Portuguese, or Spanish were also included.
It is worth noting that review studies, experimental studies on animals, opinion studies, and those that did not meet the inclusion criteria or were not available in full were excluded. Furthermore, the selection of studies was made by two reviewers who independently performed the analysis of the studies.
The risk of bias assessment of articles was used, proposed as a methodological quality step. The risk of bias stands out as an essential component in the review of the quality of scientific studies, especially in systematic reviews. For this purpose, the Cochrane Risk of Bias Assessment Tool was used, which applies mainly to randomized clinical studies, as it assesses the bias of randomization, allocation and blinding of participants and researchers.7,8
Randomization and the allocation sequence are understood as fundamental to ensure that participants are distributed impartially into the study groups, avoiding bias in selection. Allocation concealment becomes important because it analyzes whether the allocation is not kept secret until the inclusion of participants, whether there is a risk of manipulation in the groups, compromising the validity of the study. Furthermore, blinding of participants and researchers aims to prevent expectations about the intervention from influencing the results. Similarly, blinding outcome assessors is crucial to prevent knowledge about the intervention from being influenced in the interpretation of results.7,8
Assessing incomplete data is also important, as missing participants or missing data can compromise the integrity of the study, distorting the results. Selective reporting of results assesses whether all planned outcomes were presented, or whether only the most favorable ones were highlighted.7,8
Finally, the tool also considers other risks of bias, such as study funding and conflicts of interest, which can influence the impartiality of the results. Each study is rated for risk of bias in each of these domains, with the categories “low,” “high,” or “undetermined” providing a clear view of the methodological quality of the included studies.7,8
2.1 Ethical Considerations
This study is characterized as a systematic literature review, structured and reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, which aim to ensure transparency, replicability, and methodological rigor in the synthesis of scientific evidence. Given that the present review exclusively utilized data from studies already published in peer-reviewed journals and publicly available databases, without direct involvement of human participants or access to identifiable personal information, the research did not require approval by an Institutional Review Board (IRB) or ethics committee.
In accordance with international norms and ethical frameworks for secondary research, such as those outlined by the International Committee of Medical Journal Editors (ICMJE) and the Cochrane Handbook for Systematic Reviews of Interventions, ethical approval is not mandatory when the study does not involve the collection of new data from individuals or animal subjects. All data analyzed in this review derive from previously conducted studies that presumably underwent their own institutional ethical evaluations and received approval or waiver before participant recruitment and data collection.
Furthermore, the included studies were carefully selected based on inclusion and exclusion criteria that prioritized methodological quality and transparency in ethical conduct. When available, information regarding the ethical approval of each primary study was considered during the data extraction phase to ensure that the body of evidence reflects adherence to research integrity principles.
No interventions, surveys, or contact with patients were performed as part of this review. As such, no informed consent was required, and no risks were imposed on individuals. The synthesis of knowledge presented herein seeks to respect the ethical principles of beneficence, non-maleficence, and respect for autonomy, contributing to evidence-based clinical decision-making and the promotion of safe and effective treatment strategies.
Results
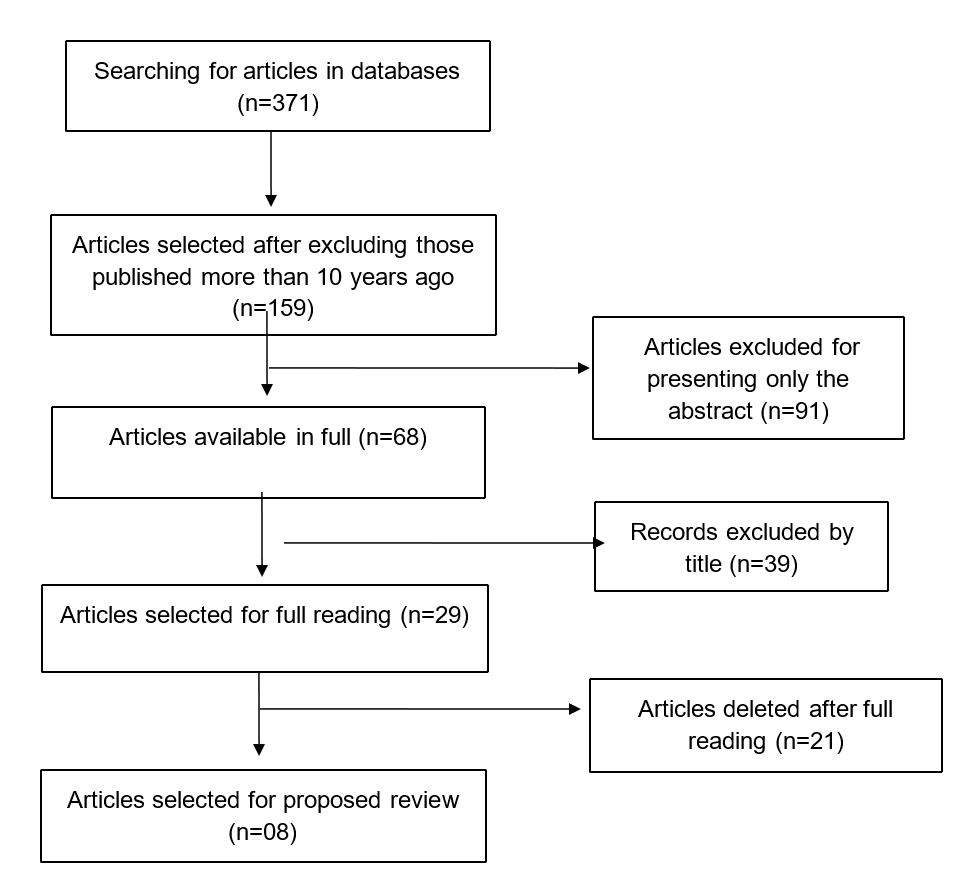
A total of 371 articles were found through the database search. Of these, 159 articles published more than 10 years ago were excluded. Through this, those that did not present their full version, those with only an abstract and some by title were excluded. Finally, 29 articles were read, and eight studies were selected, as highlighted in Figure 1, which represents the screening and selection of studies, according to the PRISMA methodology.

From then on, four tables were developed with the findings of the studies, containing the main characteristics, such as authors, year, sample, type of study, among others. The types of treatments performed in the conservative and surgical groups, the main outcomes and the risks of bias.
Thus, Table 1 presents the characterization of the articles selected in the review, according to their identification, title, authors/year; type of study, sample and follow-up (duration in months). It was then observed that randomized clinical trials, multicenter, prospective and retrospective trials were included. In addition, it is noteworthy that the main focus of the studies was to compare surgical treatments (open or minimally invasive) and conservative treatments in cases of Achilles tendon injury.
The studies varied between 30 and more than 500 participants as a sample. Furthermore, the majority had a period of duration between 12 and 24 months, except for one study that had a longer duration. It is also worth highlighting that the time frame of the selected articles was 10 years, between 2015 and 2025.
In terms of treatment results, it is observed that the studies, in their majority, report that surgical and conservative treatment have similar efficacy in many aspects, with no significant differences when compared. However, conservative treatment was associated with a higher risk of new rupture, although it resulted in fewer nerve injuries than surgical treatments.
In other studies, as reported by Saab et al. (2024),9 conservative treatment was related to greater muscle atrophy and greater tendon elongation, in addition to a significant difference in functional performance, such as in the heel raise test and in the single-leg hop, compared to surgical treatment. This suggests that surgical treatment can provide a faster functional return.
In addition, Lantto et al. (2016)10 observed that, regardless of surgical or conservative intervention, functional results were similar. On the other hand, surgery was associated with faster recovery of muscle strength, but conservative treatments showed satisfactory results in terms of long-term functional recovery. Finally, the table also shows that, in some studies, such as that of Westin et al. (2020),11 the conservative and surgical treatment groups presented good long-term results, with no significant difference in relation to patient satisfaction.
Table 2 presents the quantitative outcomes of the selected articles, comparing adverse events, mainly in relation to new ruptures. It is noteworthy that the rates for conservative treatments were higher when compared to surgical treatments. On the other hand, surgeries showed more cases of nerve injuries and infections. It is worth noting that in both groups there was loosening of the structure and thickening of the cross-sectional area of the tendon, when compared to the uninjured tendon.
In addition, the injured tendon continued to have harmful characteristics, such as elongation, thickening and inferior tissue quality, resulting in lower elasticity and strength compared to the healthy tendon. Furthermore, in general, the studies demonstrate that, although the rates of new rupture may vary, both treatments — conservative and surgical — present positive functional results, with some differences in terms of complications and recovery.
Finally, Table 3 presents the assessment of the risk of bias of the selected articles, taking into account three main domains: randomization, allocation concealment and blinding of evaluators.
Regarding randomization, most studies showed a low risk of bias, indicating that participants were randomly allocated appropriately. Regarding allocation concealment, most studies showed a low risk, which indicates that the allocation of participants was maintained blindly and without interference. On the other hand, one study showed a high risk, which suggests that the allocation process may have been susceptible to bias, with the possibility of researchers interfering in the allocation of participants. In addition, one study did not provide sufficient information to determine the risk related to allocation concealment, being classified as undetermined.
Finally, in the domain of blinding of evaluators, the vast majority of studies had a high or undetermined risk, thus highlighting that the blinding of evaluators was not adequately described or implemented, resulting in a high risk of bias for these articles.
Overall, the assessment revealed that most studies presented a low risk of bias in the domains of randomization and allocation concealment, but the implementation of blinding of assessors was a critical point, with several studies presenting high risks due to the lack of adequate blinding or the lack of clear information about the process.
Discussion
According to Fabião et al. (2023),4 the choice of treatment for Achilles tendon injuries derives from the joint decision between physician and patient, weighing the functional benefits and complications inherent to each treatment option. The surgical option may include open, minimally invasive or percutaneous techniques, while the conservative modality is essentially based on plaster immobilizations and functional orthoses.4
According to the review proposed by the study, it was observed that there was no consensus on the best treatments or gold standard treatment for Achilles tendon injuries. The articles sought to compare, for the most part, conservative and surgical treatments, through clinical, prospective, retrospective and multicenter studies, each in its own style. However, each treatment presented benefits and risks, with no better or worse being presented.
Traditionally, conservative treatment is based on the principle of plaster immobilizations or functional orthoses for a period of approximately six to eight weeks. In this mode, the ankle is placed in plantar flexion, neutralizing the ankle position over time. This has the benefit of not having the risk of complications related to surgery, such as wound healing problems, scar tissue, tendon adhesion, infection or nerve damage. However, according to studies, this form of treatment would result in higher rates of new ruptures, reaching 9% of cases. In this sense, it is worth noting that more than half of these new ruptures occurred in the first 10 weeks after the injury.4,12,13
When it comes to surgical treatment, there are several techniques categorized, generally as open, minimally invasive and percutaneous. The main objective of this form of treatment is to restore the length and tension of the tendon. The open approach is performed through the posteromedial approach, proceeding to the suture of the distal and proximal ends of the tendon. The percutaneous approach allows the tendon to be sutured by puncturing its ends. The minimally invasive approach was developed in an attempt to reduce the risk of skin problems associated with open surgery and the risk of injury to the sural nerve reported with the percutaneous approach, as highlighted by Fabião et al. (2023).4
Thus, the main benefit of surgical treatment would be the reduction in the rate of new ruptures, reaching 4% of cases. On the other hand, this form of treatment can lead to a higher risk of complications such as deep vein thrombosis, wound healing problems and scar adhesions.12,14
A study by Ochen et al. (2019)15 highlighted that the incidence of complications after surgical treatment was 4.9% and after non-operative treatment, 1.6%. The main complication after surgical treatment was infection, which occurred in 2.8% of patients. The main complication after nonoperative treatment was deep vein thrombosis, which occurred in 1.2% of patients.
Furthermore, Kosiol et al. (2023)14 showed that early functional rehabilitation protocols reduce the rate of new ruptures in patients treated non-surgically to a level similar to that of patients treated surgically. Thus, the authors pointed out that such rates can be positively influenced by early functional rehabilitation protocols, since tendons need a functional stimulus for healing and parallel orientation of collagen fibers. For Saab et al. (2024),9 regardless of the treatment listed, there is a need for strict immobilization for at least three weeks in both treatment cases. In this sense, minimally invasive surgical techniques have been developed to reduce the risk of complications associated with open surgical repair.
However, a study by Myhrvold et al. (2022)13 highlighted that randomized and controlled clinical trials comparing non-operative treatment, open repair, and minimally invasive surgery were unable to associate good short- and long-term results, due to the limited sample sizes and current studies. According to Myhrvold et al. (2022),13 open repair or minimally invasive surgery in patients with Achilles tendon injury did not improve total scores at 12 months compared to non-operative treatment. In addition, Westin et al. (2021)11 highlighted that surgical treatments indicate direct health costs and indirect costs, such as sick days, compared to non-surgical treatment.
On the other hand, surgical treatment, for Lannto et al. (2016),10 resulted in faster and better recovery of calf muscle strength throughout the range of motion of the ankle joint compared to the non-surgical group. There were also better results in the domains of physical functioning and bodily pain for patients treated surgically. For the authors, surgery resulted in better health-related quality of life in the domains of physical functioning and bodily pain compared to non-surgical treatment. However, there was no statistically significant difference between the treatments in terms of satisfaction or willingness to recommend to friends or family, as both reported good results in long-term follow-up.16
It is worth noting that Kosiol et al. (2023)14 observed, in their study, a superior performance of surgery in restoring calf muscle strength of the triceps surae muscle compared to conservative treatment. However, neither the operative nor the conservative treatment restored the muscle to the same strength as the healthy side. These results correlate by highlighting that, regardless of the treatment selected, the injured tendon remains elongated, thickened and of inferior tissue quality.
Thus, the length of the Achilles tendon on the injured side was seen to increase by 50.9% at rest and by 44.4% under load, with no statistically significant difference for the operative or conservative treatment. Furthermore, the tendon diameter on the injured side was increased to 113.0% at rest and to 124.5% under load, with no statistically significant difference for surgical or conservative treatment.17
Therefore, it is highlighted that erroneous rehabilitation can be produced by excessive tendon stress and the degree of separation of the tendon end in non-surgical treatment. For this reason, non-surgical treatment requires an effective and quality rehabilitation plan. This is because, for Westin et al. (2021),11 the type of rehabilitation can moderate the effectiveness of the treatment, including individual aspects of the patient, such as muscle mass, body habitus, physical condition before the injury and the way in which they performed physical activity previously.
For Ochen et al. (2019)15 and Myhrvold et al., (2022),13 conservative and surgical treatment constitute equivalent treatment options for Achilles tendon injuries, but they highlight the need for more systematic reviews of randomized controlled clinical trials and observational studies, through more in-depth investigation of rehabilitation protocols, weight-bearing restrictions, and treatment modalities.
In addition, Westin et al. (2021)11 highlight that the reduced rates of new ruptures after surgical treatment have been the main argument in promoting surgery as the main treatment option compared to non-surgical treatment. However, such a benefit, by itself, does not indicate an intrinsic relationship between patient-related factors and the treatment approach. This is because, through their study, Westin et al. (2021),11 it is verified that there is no inferiority or superiority for surgical or conservative treatment. Only, there are cases that require one or the other and that should be listed together with the patient’s needs and in medical evaluations.
Non-surgical treatment with an appropriate rehabilitation strategy can result in acceptable functional outcomes, new ruptures, and lower overall costs, without the risk of wound complications. On the other hand, surgeries, regardless of the method, can reduce new ruptures, but cause other adverse events and a higher cost. Therefore, including patients’ preferences and expectations regarding clinical outcome is imperative when deciding on the treatment approach. Patient adherence becomes critical to the success of interventions.11
It is also worth noting that the proposed study may have a risk of bias in the articles analyzed, as they present differences in follow-up time, location, techniques, professionals, and other important aspects for a good evaluation. In addition, the results may be influenced by missing articles regardless of the extensive search in the databases.
Furthermore, the incidence of complications may be affected by the use of different treatment protocols, which makes a comparative analysis of the literature difficult.
Therefore, it is clear that there is a need for future research on treatments for Achilles tendon injuries, through current clinical trials, with more rigorous methodologies and longer follow-up periods. This is because there is disagreement between studies regarding the best treatments, indicating a substantial need for more research in this area. Studies that seek to compare ages, comorbidities, variety of populations and the success of treatments are suggested.
Limitations
Despite the methodological rigor adopted in this systematic review, certain limitations must be acknowledged, as they may influence the interpretation, consistency, and generalizability of the findings. One of the primary limitations concerns the heterogeneity of the included studies, especially regarding the duration of follow-up, the diversity of rehabilitation protocols, and the variability in the clinical and demographic characteristics of the participants. These discrepancies limit the possibility of direct comparisons across studies and may dilute the statistical power of aggregated conclusions.
The follow-up periods ranged significantly, from as short as 12 months to over 180 months. While long-term data offer valuable insights into the durability of treatment outcomes, they may also reflect changes in clinical practices, rehabilitation technologies, and surgeon expertise over time. Conversely, shorter follow-up periods might fail to capture late complications, reruptures, or long-term functional deficits, thus presenting an incomplete picture of treatment efficacy.
Rehabilitation protocols also varied considerably between studies. While some trials adopted early mobilization strategies and functional orthoses, others relied on prolonged immobilization. The lack of standardization in post-treatment care introduces a relevant confounding variable, as functional recovery and rerupture rates are directly influenced by the quality and timing of rehabilitation. It becomes challenging, therefore, to discern whether the reported outcomes are attributable to the surgical or conservative interventions themselves, or to the differing rehabilitative approaches employed.
Population heterogeneity represents another significant source of bias. The included studies encompassed participants with varied ages, baseline levels of physical activity, comorbidities, and injury mechanisms. For example, individuals involved in high-performance sports may respond differently to treatment compared to sedentary individuals or the elderly. The absence of subgroup analyses in most trials impairs a nuanced understanding of how specific patient profiles may benefit more from one treatment modality over another.
Moreover, although this review prioritized randomized controlled trials (RCTs) and high-quality observational studies, differences in methodological designs, such as sample size, blinding procedures, and randomization techniques, further limit comparability. Many studies presented high or unclear risk of bias in the domain of outcome assessor blinding, which may have introduced measurement bias, especially in the evaluation of subjective variables such as pain and patient satisfaction.
Publication bias may also be present, as studies with negative or inconclusive results are less likely to be published. In addition, language bias must be considered, as the search was limited to articles published in English, Portuguese, and Spanish, possibly excluding relevant data available in other languages. Although comprehensive search strategies and Boolean operators were used to maximize retrieval, it is possible that eligible studies were inadvertently missed.
Finally, the lack of meta-analysis or quantitative synthesis in this review constitutes an additional limitation. Given the heterogeneity in data reporting, outcome definitions, and statistical measures, the pooling of results was deemed methodologically inappropriate. Consequently, the findings of this review are based on narrative synthesis, which, although informative, may be subject to interpretative bias.
These limitations highlight the need for future research with standardized methodologies, clearly defined outcome measures, homogeneous rehabilitation protocols, and stratified analyses by patient characteristics. Only through such refinements can the orthopedic community advance toward evidence-based and personalized therapeutic strategies for Achilles tendon ruptures.
Conclusion
This review indicated that there is no consensus in the literature on a gold standard treatment for Achilles tendon injuries. Both surgical and conservative approaches have benefits and risks, and the choice of treatment is based on a shared decision between physician and patient. Surgical treatment tends to reduce the rate of new ruptures, but is associated with higher risks of postoperative complications, while conservative treatment avoids surgical complications, but has a higher rate of new ruptures.
In addition, studies indicate that early functional rehabilitation can reduce the risks of conservative treatment, making it comparable to surgery in terms of efficacy. However, the choice of the best approach should consider individual factors, such as age, level of physical activity and patient preferences, since both methods can offer good long-term results.
The findings of this review therefore highlight the need for more randomized and controlled clinical studies, with more rigorous methodologies and long-term follow-up, to clarify the best therapeutic strategies. Future research should consider variables such as age, comorbidities and different population profiles, in order to provide more solid guidelines for clinical practice.
Authors’ contributions
Nilton Santos Júnior – conceptualization, methodology, investigation, writing – original draft.
Leonardo Santana – data curation, formal analysis, writing – review and editing.
Rafael Rodrigues – methodology, supervision, writing – review and editing.
João Pedro Cruz Oliveira – project administration, validation, correspondence.
Conflicts of interest
The authors declare no conflicts of interest.
Funding and additional information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The work was not previously presented at scientific events.