Introduction
Hip pain is a common complaint among athletes which typically results from acute injury, repetitive overuse, or developmental conditions.1 Currently, common hip pathologies can be addressed by hip arthroscopy which is a rapidly growing field within sports medicine. Hip arthroscopy has historically been used as a diagnostic tool for unexplained hip abnormalities, but with progress over the past few decades, this technique has evolved to allow surgeons to surgically treat various pathologies of the hip.2 This is attractive to athletes because it is a less invasive technique which allows for a quicker return to sport at or near the same level of play for many athletes.
Hip arthroscopy procedures have been well tolerated by the athletic population with durable long-term results. A recent systematic review found that patient reported outcome measures (PROMs) significantly increased in athletic cohorts who received hip arthroscopy for FAI with RTS rates ranging from 73%- 100%.3 Among the various treating hip pathologies, the current evidence indicates high RTS rates (87-93%) after hip arthroscopic procedures.4 In addition, these results were further corroborated in a long-term study which found that primary hip arthroscopy in athletes results in 85.7% survivorship at a minimum 10 year follow up.5 Returning to sport in a timely manner is often an important issue for athletes, coaches, teams, and the clinical care providers. While there are numerous publications examining RTS rates, and general rehabilitation protocol following hip arthroscopy, there is often variability within the current literature on the objective criteria used to release athletes back to sport following hip arthroscopy procedures.6 There remains a gap in the knowledge for a criteria- based testing protocol as a means of progressing athletes back to sport following hip arthroscopy.
Therefore, the purpose of this systematic review is to review the existing literature to describe the objective RTS criteria to better inform providers with a standardized testing protocol to follow when releasing patients to return to sport after hip arthroscopy.
Methods
Eligibility Criteria
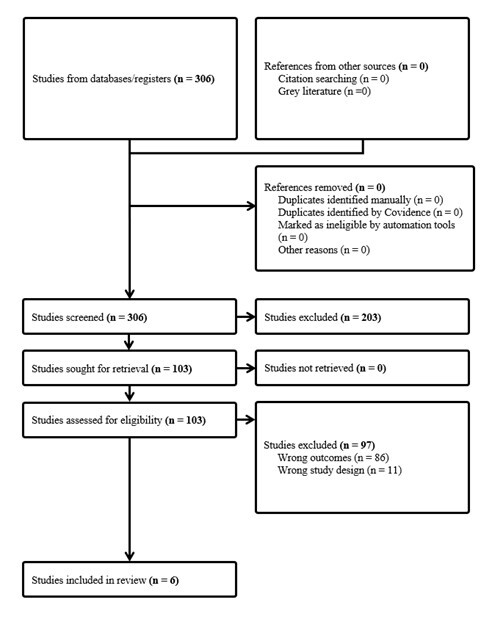
A comprehensive literature search of several databases was performed by the Mayo Clinic Library on June 14, 2024, according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Results were limited to English language, human studies which included patients who were between the ages of 10-50. Studies published between 2010-2024 were included. Databases that were utilized included Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, and Daily, Ovid EMBASE, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus. The search strategy was designed and conducted by an experienced librarian with input from the study’s principal investigator and study team. Controlled vocabulary supplemented with keywords was used to search for return to sport following hip arthroscopy in humans. The actual strategy listing all search terms used and how they are combined is available in the appendix.
Three-hundred and six articles were identified and screened independently by two authors (C.H, P.S) Studies eliminated by both reviewers were removed. Disagreements were resolved between the reviewers. Articles excluded during screening included clinical commentaries, not published full-text, systematic reviews, or review articles. Remaining studies were reviewed for the following inclusion criteria: (1) interventions including hip arthroscopy, (2) hip joint based interventions and outcomes, (3) objective return- to- sport criteria, (4) clinical population, and (5) one or more clinical outcomes (strength, range of motion and patient reported outcome measures. Exclusion criteria were not meeting any of the inclusion criteria and studies presented as abstract at conferences without full text available. Six (n=6) studies were ultimately included. Figure 1 includes the PRISMA flow chart.

Data Collection
Working in duplicate using a computerized extraction form, P.S and C.H abstracted data describing the study design, population, and objective RTS criteria. All age and RTS times available were included (mean, SD), (range). All objective RTS criteria available was included.
Quality Assessment
A pair of reviewers worked independently to determine the reported methodological quality of eligible cohort studies using the Newcastle-Ottawa-Scale for cohort studies (Table 3). For the cohort studies, the authors assessed the adequacy of the representativeness of exposed cohort and non-exposed cohort, ascertainment of exposure, comparability of cohorts, bias protection in the outcome assessment, and adequacy of outcome follow-up. Case series were not included in the quality assessment. The reviewers came to a consensus on bias assessment with a supervisor (MH).
Data Extraction and Analysis
Study characteristics, patient characteristics, arthroscopy details, RTS rates, and objective RTS criteria were extracted from each study. Because all of the included studies were cohort studies, there was heterogeneity in the variables collected and reported which did not allow us to perform a meta-analysis. A descriptive review was conducted on all the studies, and objective RTS criteria reported by each study are detailed in table 2.
Results
In total, 6 studies were included in this review (Table 1). Clapp et al,7 Frank et al (2019),8 and McDonald et al.9 were retrospective cohort studies. Waltz et al,10 Saito et al,11 and Frank et al (2018)12 were case series that measured outcomes of athletes following hip arthroscopy. Clapp et al.7 and Frank et al (2019).8 investigated outcomes of hip arthroscopy in a matched cohort study between athletes and non-athletes. McDonald et al.9 investigated performance data on hockey players who received a hip arthroscopy to matched control hockey players. All 6 studies included in this review investigated outcomes following arthroscopic treatment for femoroacetabular impingement (FAI). The average age ranged from 18 to 31.3 years. Notably, there was variability in the amount of male and female patients in the studies, with Frank et al. (2019)8 reporting 100% female patients, and Saito et al.11 and McDonald et al.9 including 0 female patients in their studies. Some studies published data and protocol on specific sports, including skiing/ snowboarding, soccer, swimming and hockey. Clapp et al.7 and Frank et al. (2019)8 reported RTS protocol for multiple different sports, including: soccer, softball, running, dancing, golf, baseball, basketball, hockey, etc. The average time to RTS, while not reported in all of the studies, ranged from 3.4- 8.9 months.
Table 2 includes a summary of the objective RTS criteria used in these studies. Five studies reported using sports testing as a criterion to return to sport.7–11 Patient reported outcomes were also a criterion in 4 studies where patients needed to be pain free to RTS.7,8,11,12 Sufficient range of motion in the hip (equal to the contralateral side or a numerical benchmark) was required to RTS in 3 studies,10–12 whereas hip strength was described as a criterion in 2 studies.10,12 Performance-based criteria, including agility, dynamic and functional control were reported in 3 studies as criteria to RTS.7,8,11
Sports Specific Tests and Performance Based Criteria
The included studies used “Sports Specific Tests” and “Performance Based Criteria” without clear definitions of these terms. Therefore, we decided to group them together. Waltz et al.10 described using the Hip Sports Test as a method for RTS clearance. The Hip Sports Test- designed to evaluate function during rehabilitation after hip arthroscopy, determines readiness to RTS through the assessment of strength, coordination, agility, and pain-free ROM. The Hip Sport Test consists of 4 exercises that are performed for a designated amount of time, including a single-leg squat, lateral agility test, diagonal agility test, and a forward box lunge. After completion of the 4 exercises, the points earned from each exercise are added together, and a total score of 17 or higher is considered a passing score. The entire test takes less than 15 minutes with minimal equipment.13 Clapp et al.,7 Saito et al.,11 Frank et al. (2019)8 and McDonald et al.9 all required patients to pass a RTS test for which details were not specified in the study.
Of the studies that used performance-based criteria as an objective measure of sufficiency to release patients back to sport, Clapp et al.7 and Frank et al. (2019)8 allowed patients to RTS if they had full dynamic functional control which was not defined. Saito et al.11 stated that patients were allowed to return to soccer if they were able to perform all sport specific drills at full speed.
Pain- Free
Clapp et al.7 and Frank et al. (2019)8 reported that patients were cleared if they could participate in sports without pain. Saito et al.11 reported that in order to return to soccer, patients should have pain- free ROM, as well as the ability to perform all sport-specific drills at full speed without pain and discomfort. Lastly, Frank et al. (2018)12 determined that patients were able to return to swimming following hip arthroscopy if they were determined to be pain- free in the hip complex. Patient-reported-outcomes were used to monitor and measure pain during recovery for all studies.
Range of Motion
Waltz et al.10 stated that patients were allowed to RTS if they had symmetrical ROM. Saito et al. reported that a ROM assessment is conducted for patients before they were cleared to RTS. To return to swimming, Frank et al. (2018)12 reported that patients regained full ROM and there was no significant differences in hip range of motion compared with preoperative values, including flexion, internal rotation, and external rotation.
Hip Strength
In 2 studies, sufficient strength of the hip to the contralateral side was used as an objective criterion to RTS. Waltz et al.10 stated that patients who had 90% of hip strength to the contralateral side were cleared to RTS. Frank et al. (2018)12 said that patients were allowed to RTS if they had regained full muscular strength which was not defined within the study.
Discussion
The aim of this systematic review was to investigate the objective return- to- sport criteria used following hip arthroscopy. This review found that although there are high rates of return to sport for athletes following hip arthroscopy, there is a large amount of heterogeneity in the objective testing used to determine RTS.14 In total 6 studies were included that reported using objective measures as criteria to RTS. Overall, there were 5 different types of criteria for patients, including sports specific performance testing, pain-free movement, full ROM and hip strength, as well as performance-based measures. Most of the studies who reported using sport testing as a criterion did not specify what kind of tests were involved, impacting our understanding of specific clearance criteria.
Many of the studies in our review included detailed rehabilitation protocol before return- to-sport clearance. Waltz et al. emphasized using physical therapy to progress to active range- of- motion, strength, and endurance. Towards the end of the rehabilitation protocol, these authors emphasized that a discussion between the athlete, physical therapist, and surgeon on return to play and competition occurs. Clapp et al,7 Saito et al, Frank et al (2019),8 Frank et al (2018),12 and McDonald et al.9 included a standardized 4 phase rehabilitation protocol, with focus on ROM, dynamic muscular control, and endurance. Phase 4 in the protocol emphasized return to preinjury level of sports participation with safe and gentle sport- specific drills. Saito et al. included a reference to Stalzer and colleagues15 review on rehabilitation following hip arthroscopy. This review by Stalzer et al.15 details a 4 phase recovery process, with detailed description of hip movement and progression at general timepoints.16 Also, all of the studies used PROMs as another method of patient follow- up and as a supplement to evaluate return- to- sport readiness. It will be critical for patients and the rehabilitation field to develop criteriabased, objective return to sport testing protocols following hip arthroscopy.17,18
This review identifies several limitations in current literature. All included studies were retrospective cohort studies or case series examining athlete outcomes following hip arthroscopy. These studies generally had small sample sizes and short follow-up periods. Longterm studies would be valuable to better understand the relationship between hip arthroscopy outcomes and objective return-to-sport (RTS) criteria. Additionally, well-conducted randomized controlled trials (RCTs) are needed to validate and determine the most appropriate RTS criteria for safely returning athletes to sport.
In this review, we found that patients undergoing hip arthroscopic procedures often lack standardized, objective RTS criteria, in contrast to patients who undergo anterior cruciate ligament (ACL) reconstruction procedure. While ACL rehabilitation is guided by strict, evidencebased RTS criteria which evaluate factors such as strength, range of motion, and functional performance to ensure safe return to sport, hip arthroscopy patients typically follow less structured protocols. This discrepancy is due to a lack of consensus on specific, measurable criteria for hip arthroscopy recovery, leaving clinicians to rely more on subjective assessments and individual clinical judgment. As a result, athletes recovering from hip arthroscopy may not have clear benchmarks to guide their safe return to sports, highlighting a significant gap in the rehabilitation process that warrants further research and development of evidence-based guidelines.
Conclusion
This review found that there is a lack of consensus on what testing should be performed to release patients back to sport following hip arthroscopic procedures. Common criteria that are mentioned in the studies included in this review are passing sports specific testing, absence of pain, symmetrical ROM, and regaining hip strength. Future research should be conducted to investigate which objective measures are most important for a patient to achieve a successful RTS outcome.
Authors Contributions
Scott: Ms.Scott helped with screening of articles, data synthesis, and manuscript preparation.
Hegarty: Mr. Hegarty helped with screening of articles, data synthesis, and manuscript preparation
Johnson: Mr. Johnson helped with data synthesis, manuscript preparation, and clinical insights.
Eischen: Mr. Eischen helped with data synthesis, manuscript preparation, and clinical insights.
Krych: Dr. Krych helped with formulating research questions, manuscript review and preparation, and clinical insights.
Nagelli: Dr. Nagelli helped with formulating research questions, data synthesis, manuscript preparation and review.
Hevesi: Dr. Hevesi helped with formulating research question, data synthesis, manuscript preparation and review, and clinical insights.
Conflicts of Interest
There are no conflicts of interest.