


INTRODUCTION
Intertrochanteric femoral fractures, accounting for approximately 50% of hip fractures, are a leading cause of morbidity in elderly patients, typically resulting from low-energy falls.1 The incidence of these fractures is increasing with the aging population, with an estimated 304 cases per 100,000 inhabitants in 2019, in the US population, contributing to 1-year mortality rates of 20–32%.2–4 Intertrochanteric femoral fractures are typically treated with internal fixation, intramedullary fixation or dynamic hip screw (DHS) depending on fracture characteristics, to facilitate early ambulation and reduce the risk of complications and mortality.5 Despite high union rates of up to 90%, mechanical complications, including lag screw cut-out (1–5%), and implant breakage (0.4–0.88%), remain significant challenges.6–9
In this case report, we present an 87-year-old patient who suffered a subcapital femoral neck fracture along with fracture of the cephalic lag screw, one year after a successfully healed intertrochanteric fracture treated with a cephalomedullary intramedullary implant. The purpose of our study is to highlight this rare complication, present our therapeutic approach and discuss its implications in the context of current literature on cephalomedullary nail failures.
CASE PRESENTATION
An 87 year old female patient with a history of arterial hypertension and early-stage dementia presented at the emergency department after a fall from standing height. Plain radiographs demonstrated a subcapital fracture of the right femur accompanied by a fracture of the cephalic lag screw of a previously implanted intramedullary nail. The nail itself was still in the same position, and no signs of loosening or failure at the original fracture site were identified. Following this, a computed tomography (CT) scan was made to evaluate the condition of the previous intertrochanteric fracture and confirmed no evidence of fracture non-union, malalignment, or any other structural abnormalities. Figure 1 shows the anteroposterior X-ray and CT scan of the subcapital femoral neck fracture and fractured cephalic lag screw.
_anteroposterior_x-ray_demonstrating_the_subcapital_femoral_neck_fracture_and_a_fractur.png)
When reviewing the surgical history of the patient, it was revealed that she had sustained a right-sided intertrochanteric (AO/OTA 31A1.3 type) femoral fracture due to fall from her height, one year prior to her current admission. The hip fracture was uneventfully treated with closed reduction and the use of a cephalomedullary intramedullary implant (Dyna Locking Trochanteric DLT™ Nail, U & I Corporation 529-1,Yonghyun-dong, Uijungbu Kyunggi-Do, Korea). Figure 2 shows the preoperative radiographic image of the fracture and the immediate postoperative X-Ray. There were no postoperative complications and the patient was discharged at a rehabilitation center with instructions to bear weight as tolerated. According to her caregiver the patient was doing well and walking with minimal support, and therefore she did not visit our outpatient clinic for regular follow-up.
_anteroposterior_radiograph_of_the_pelvis_showing_a_displaced_intertrochanteric_fractur.png)
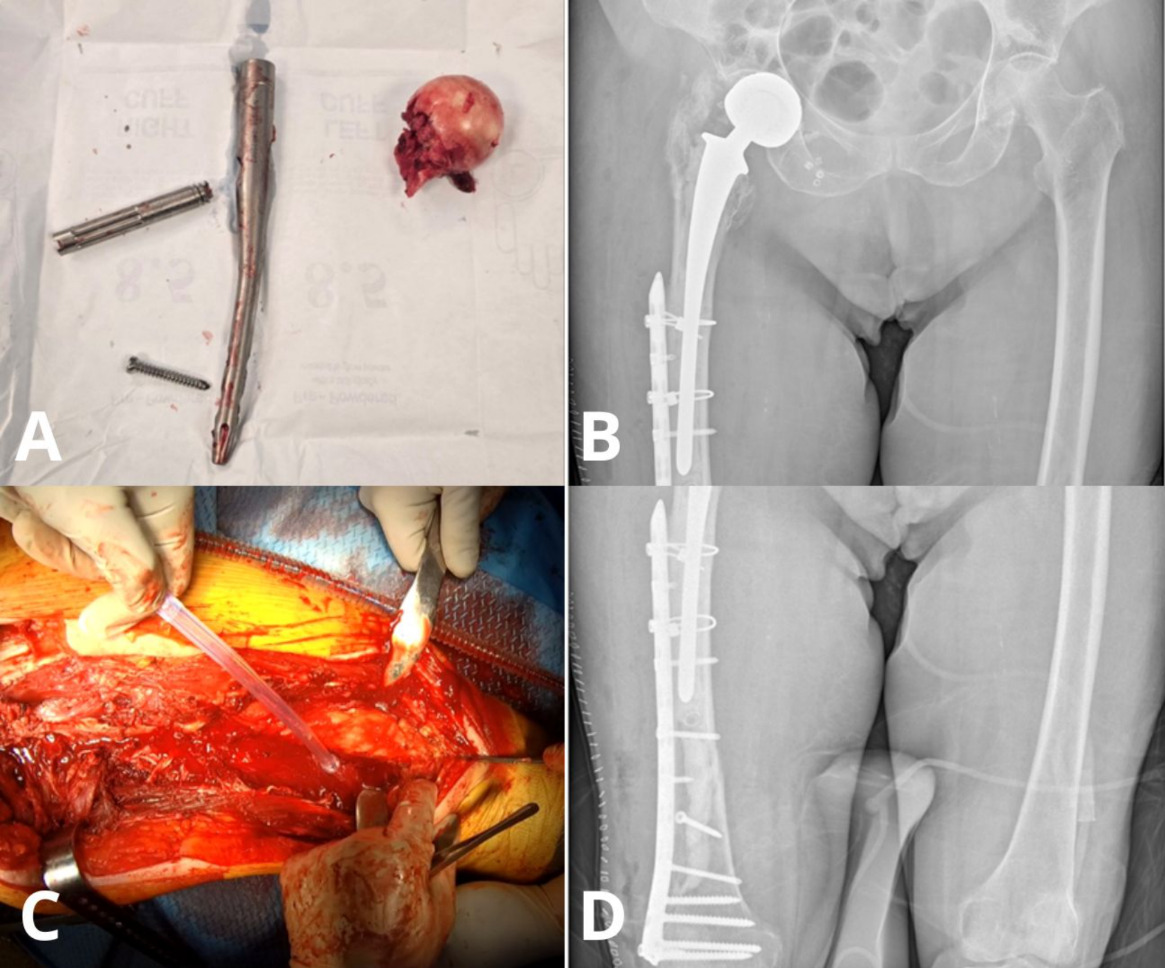
After the diagnosis of the patient’s current injury, she was admitted for revision surgery. Intraoperatively, the previously implanted cephalomedullary nail was extracted, including the fractured cephalic lag screw and femoral head to allow for reconstruction. Given the patients’ advanced age, poor bone quality, and the nature of the injury, the surgical team decided to proceed with a cemented total hip arthroplasty (THA). The choice of THA was made due to re-fixation not being a viable option given the location of the new fracture and her osteoporosis. In addition, a dual mobility implant was chosen to decrease the possibility of postoperative dislocation. Unfortunately, the patient intraoperatively suffered a simple spiral supracondylar femoral fracture while removing the intramedullary nail. The intraoperative fracture was addressed with internal fixation using two interfragmentary lag screws and a long supracondylar locking plate. Next, the acetabular and long femoral component were cemented in place, and after inserting the dual mobility bearing, hip stability was confirmed. Intraoperative fluoroscopy was used to evaluate correct positioning of the implant at the end of the procedure. Figure 3 depicts the retrieved implant and the femoral head, as well as the immediate postoperative radiographic image.
The postoperative course was uneventful without any complications. The patient was instructed to use a walker and partially bear weight for three months. Three months postoperatively, the patient was able of full weight bearing with the aid of a walker. The patient’s caregiver provided written informed consent to publish material that may relate to the patient.
DISCUSSION
Even though the use of cephalomedullary nails has been widely accepted as the standard treatment for intertrochanteric fractures, rare mechanical complications can still occur. Lag screw cut-out has been reported to be the most commonly observed mechanical failure, ranging from 1% to 5%.8 One of the most predictive parameters that contribute to this complication is the Tip-Apex Distance (TAD), as values greater than 25 mm can cause reduced anchorage to the femoral head.10 Another critical factor is osteoporosis, which might lead to migration of the lag screw due to poor holding strength and cyclic loading.11 Furthermore, varus malalignment and high shear forces in osteoporotic bone during weight-bearing amplify the risk.12,13 In our case, the TAD was within acceptable limits and no evidence of varus malalignment was present.
While lag screw cut-out is the most common mechanical complication following intertrochanteric fractures, implant breakage is considerably rarer, ranging from 0.4% to 0.88% in large multicenter studies as mentioned before.6–9 This type of complication is usually associated with material fatigue, which is the result from prolonged cyclic loading, especially whenever there is delayed union or non-union at the lag screw-nail junction.14 In addition, unstable or comminuted fracture patterns also play a role, especially those without medial cortical buttress support or lateral wall support that transfer the increased load to the implant.15 Tarrant et al. analyzed 110 patients with unstable intertrochanteric fractures and found that medial calcar comminution was significantly associated with implant failure, especially nail breakage, which shows the importance of anatomic support for implant longevity.15 Furthermore, undersized or short nails reduce overall stability, and early weight-bearing in non-healed fractures cause high axial and torsional stresses on the implant.15 A case report by Smidt et al. described a lag screw breakage, probably due to repeated stress and micro-motion at the lag-screw junction in a patient with non-union.16 However, it is important to know that there are many more factors that can contribute to implant breakage, including design flaws or stress risers at the lag screw–nail junction, poor fracture reduction or incorrect nail sizing, and patient-related contributors like high BMI, osteoporosis, and early mobilization.17
Finally, a rare but documented complication following a healed intertrochanteric fracture is a subcapital femoral fracture, without associated fracture of the lag screw. A study by Lung et al. , described five elderly female patients who suffered from a subcapital femoral fracture after previously undergoing internal fixation of an intertrochanteric fracture using DHS.18 All five were after low-energy falls and the mean time interval from initial surgery to new fracture was 11.2 months, similar to our case. They managed the patients with hemiarthroplasty, THA and one underwent revision of internal fixation .18 The stress concentration at the femoral neck just proximal to the original fracture may have contributed to the new fracture. In addition, Kaneko et al. and Arington and Davino described similar injuries in elderly patients of subcapital femoral fractures after healed intertrochanteric fractures.19,20 Kaneko et al. reported two cases that occurred within four months after initial fixation by using a proximal femoral nail. They mentioned that the fractures were due to osteoporosis and stress concentration at the subcapital region.19 Both cases were managed with implant removal and conversion to THA.19,20 Arrington and Davino reported a subcapital fracture that occurred six weeks after they internal fixation with DHS.20 They suggested that lag screw depth of more than 8 mm from the subchondral bone puts concentrated stress in the subcapital area and contributed to the complication.20 The sliding nature of the DHS implant limits stress distribution which might have led to mechanical overload as well, even with healing of the original fracture. Both studies reported no implant breakage.
In our case, a traumatic fall from standing height in an 87-year-old osteoporotic patient caused acute mechanical stress on the femoral head and implant, which most likely exceeded its structural limits. The implant specific lag screw features winglets that are designed for better fixation offering increased rotational stability, compression, and resistance to cut-out. However, this design can create a weak point at the winglet-screw junction. This area may act as a stress riser and is more vulnerable to fatigue and eventual breakage under repeated loading. This is what likely happened in our case. Given the patient’s advanced age and poor bone quality, we opted for a cemented dual motility THA to reduce the risk of periprosthetic fracture.
CONCLUSION
The concurrent subcapital femoral neck fracture and cephalic lag screw fracture in our 87-year-old patient, occurring one year after a healed intertrochanteric fracture treated with a cephalomedullary nail, is a rare complication unreported in the literature. This case emphasizes the interplay of implant design, osteoporosis, and trauma in rare complications, highlighting the need for long-term bone health assessment and fall prevention in elderly patients with cephalomedullary nails.
ACKNOWLEDGEMENTS
None.