


INTRODUCTION
Elbow stiffness is a common problem following trauma or surgery which can result in significant impairment of the entire upper limb.1 Relatively minor injuries could lead to loss of motion, even though the elbow is quite a stable joint. The incidence of elbow stiffness was reported to range from around 5% to 56%.2 Morrey et al. generally defined the functional range of motion (ROM) of the flexion-extension arc for an adult to be from 30° to 130°, as well as forearm pronation-supination above 50° in either direction.3 Unfortunately, for individuals under 18 years of age formal thresholds haven’t been defined yet, but it is safe to say that they require a higher functional ROM than adults. Using the thresholds by Morrey et al., any limitation beyond these ranges that would impair function would be defined as elbow stiffness.3 However, this might vary for each patient depending on their needs and activities. For example, basic tasks like opening a door requires a relatively high ROM, meaning that small losses in mobility significantly affect the patients’ quality of life, especially in adolescents who are in their most physically active stages of life.2
The causes of post-traumatic elbow stiffness are usually multifactorial, as it can range all the way from intra-articular adhesions to bony impingement and capsular contracture.4 These pathologies could be worsened in adolescents due to open growth plates and their progressing anatomy, which makes the diagnosis and management more complex than in adults.5 In addition, the surgical treatment of elbow stiffness has been extensively studied in the adult population but remains limited in the children and adolescents.
In this narrative review we aim to discuss the available literature on post-traumatic elbow stiffness in adolescents, as well as the current evidence on the management of this pathology. This will be done by focusing on comparing the etiology, clinical presentation, management strategies, intraoperative considerations and functional outcome. In particular, we explore the growing popularity of arthroscopic treatment and how these may change the way we manage elbow stiffness in younger patients.
METHODS
A comprehensive literature search was conducted using PubMed, Scopus, and Google Scholar up to September 2025. Search terms included combinations of “post-traumatic elbow stiffness,” “arthrolysis,” “arthroscopy,” “open release,” “heterotopic ossification,” and “adolescent OR pediatric.” Articles were limited to peer-reviewed publications in English, including reviews, cohort studies, case series, and relevant technical notes.
PATHOPHYSIOLOGY & DIAGNOSIS
The development of post-traumatic elbow stiffness typically arises from a combination of structural and soft tissue abnormalities. The most famous classification of elbow stiffness is made by Morrey et al.3 This system is commonly categorized into intrinsic, extrinsic or a mix of these contractures. Intrinsic contractures are associated with intra-articular pathologies, like fibrous adhesions, malunion or articular incongruity or chondral injuries.6,7 In the child or young adolescent patient, persistent and unresolved radial head subluxation is a direct intra-articular contributor to post-traumatic elbow stiffness, which is common in Monteggia fractures as these are missed in up to 33% of pediatric patients.8
On the other hand, extrinsic stiffness is associated with extra-articular factors, such as capsular or ligamentous contractures, heterotopic ossification, neural adhesions, or malunions outside the joint space.6,7 Malunion of the distal humeral is a good example of an extra-articular cause of elbow stiffness in children and adolescents. When the distal segment of the humerus heals with posterior angulation it can lead to mechanical limitation of anterior forearm flexion, mostly because the posterior tilt impinges against the proximal ulna when attempting to flex.9 Such deformities are frequently seen in the adolescent patient due to their growing nature in combination with poor reduction of the fracture.9 Additionally, in certain cases, the ulnar nerve might get compressed, resulting in either worse symptoms of stiffness due to the patient unconsciously limiting motion because of the pain or directly limiting the ROM.10 This common entrapment neuropathy has been described first by O’Driscoll et al.10 However, most patients with elbow stiffness usually exhibit a mixed pattern of these components, especially those with severe injuries. For example, when physeal injuries lead to growth disturbances they can cause stiffness that are the result of both intrinsic and extrinsic factors. In the child and adolescent patient, if the developing epiphysis is affected due to ischemic injury in fractures, which is the result of poor vascularization of the central and lateral regions of the trochlea, it is most often referred to as a ‘fishtail deformity’.11 This might ultimately impair joint congruity and lead to decreased ROM, and thus elbow stiffness.11 It is important to understand the interplay between these mechanisms to identify the right approach to treating these patients.
There are several other authors that introduced ways to better characterize post-traumatic elbow stiffness. Regan and Reilly described the progression of elbow stiffness and identified three anatomical reasons for the predisposing factors of elbow stiffness.12 Firstly, the elbow joint has a highly complicated level of articular congruency and interconnection between its articulating surface, causing sudden disruptions to easily impair motility. Secondly, the anterior joint lies underneath the brachialis muscle, which makes it vulnerable to post-traumatic inflammation and heterotopic ossification. Thirdly, to have stable fixation in complex intra-articular fractures you often need long immobilization times to promote capsular contracture and fibrosis.12 Another classification by Kay focuses on the components involved in the cause of elbow stiffness13: (1) periarticular soft tissue contracture without bone formation, (2) soft tissue contracture with bone formation, (3) refers to intra-articular non-displaced fractures with associated contracture, (4) refers to intra-articular displaced fractures with associated contracture, and (5) characterizes bony bars due to post-traumatic ankylosis or ossification.13
As mentioned before, capsular contracture is one of the processes that greatly contributes to post-traumatic elbow stiffness. In the early stages following injuries, the lack of joint movement will promote fibroblast proliferation and collagen deposition, which will result in thickening and reduced elasticity of the capsule.14 It has been mentioned in the literature that starting with ROM exercises early can slow down progression of stiffness.15 However, there are other studies that mention the forceful manipulation of the elbow joint in association with an increased risk of heterotopic ossification.16 So, all contributing factors have to be carefully considered before deciding whether or not to start with early rehabilitation protocols.
To evaluate post-traumatic elbow stiffness it is important to take a detailed history, as the context will be able to provide us with the mechanism of injury and biological response to it. The severity of trauma, prior surgical interventions, duration of immobilization and neurovascular symptoms are examples of such elements that need to be understood.17 In addition, adolescents may underreport their symptoms and mask the severity of their loss of motion. During the physical examination, clinicians should look for any surgical scars, signs of previous trauma, skin abnormalities like burns, varus or valgus deformities, and swelling that may be of intra-articular or extra-articular cause.17 In most cases of post-traumatic elbow stiffness, patients usually do not experience any pain or discomfort when flexing or extending the elbow.17,18 However, when there are signs of discomfort and pain, it may indicate underlying arthritic changes or ulnar nerve involvement.17,18
On top of that, when these symptoms occur at rest and together with crepitus, it could even imply the presence of a low-grade synovitis, fractures or degeneration of the joint.7,19 The ulnar nerve could be palpated at the posterior side of the medial epicondyle.20 Figure 1 shows an intraoperative image of the ulnar nerve during an arthroscopic arthrolysis procedure, including additional pre-operative 3D CT reconstructions of the same case. Another way to distinguish the difference in cause of motion restriction is the feel of resistance at passive joint movement. When the endpoint feels firm, it may suggest a mechanical block like osteophyte formation, heterotopic ossification or dislocation.21 Heterotopic ossification would most likely be present alongside local swelling, tenderness and warmth. On the other hand, when it feels more elastic it could be indicative of soft tissue involvement like capsular fibrosis or adhesions.21
_intraoperative_view_showing_the_ulnar_nerve_(un)_embedded_in_scar_tissue_(white_arrow).png)
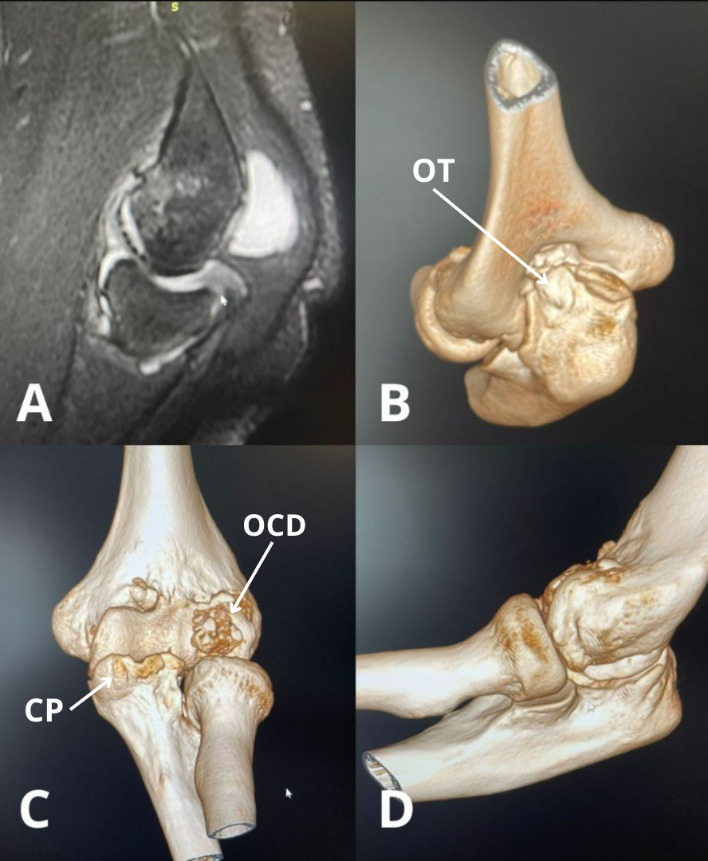
The classification system of heterotrophic ossification that would aid in treatment planning is represented by three classes, ranging from asymptomatic findings with heterotrophic ossification to complete ankylosis with or without ulnohumeral/forearm motion.22 The American Shoulder and Elbow Surgeons (ASES) also introduced standardized assessment guidelines to evaluate elbow function.23 Regarding imaging, the standard included anteroposterior and lateral radiographs.1,7,8 On the contrary, the use of computed tomography (CT) imaging would be superior when the contractures exceed 30 degrees or heterotrophic bone is present, as well as when physeal injury is suspected in skeletally immature patients or children.1,7,8 Ultrasound or electroneuromyography could be helpful to evaluate the ulnar nerve. Magnetic Resonance Imaging (MRI) is rarely used but may be reserved for the evaluation of inflammatory causes or soft tissue pathologies.1,7,8 In the child and adolescent, MRI is more often used as an accessory imaging modality to reliably measure the angle of the trochlear notch. Imaging modalities like MRI and 3D CT reconstructions are crucial when assessing joint morphology, bony impingement, or avascular necrosis, for which an example case is shown in Figure 2.
_pre-operative_mri_scan_of_a_16-year-old_patient_with_elbow_stiffness_after_chemotherap.png)
OPEN VERSUS ARTHROSCOPIC ARTHOLYSIS
The first-line approach to treating post-traumatic elbow stiffness in adolescents is conservative treatment, especially when the underlying cause has to do with soft tissue contracture and not bony deformity.21 This can be achieved through physiotherapy, bracing and splinting of the arm. The aim of conservative treatment is to restore and increase the functional ROM, while postsurgical recovery focuses explicitly on maintaining the achieved ROM.21 Claessen et al. mentioned that it is necessary to always address the bony abnormalities and deformities first before getting to the soft tissue complications, especially in post-traumatic cases.11 On the other hand, Vaquero-Picado et al. stated that if there are osseous abnormalities present causing stiffness, such as malunion or joint incongruity, then conservative treatment should not be the treatment of choice.9 However, there are more factors that need to be considered before choosing to continue with surgery.
One of those factors is the etiology of elbow stiffness, as this varies between adolescents and adults and may influence the choice and timing of the procedure. In adolescents, common causes of stiffness include osteochondritis dissecans (OCD), avascular necrosis (AVN) following supracondylar fractures, deformities from malunion, fishtail deformity, or secondary effects of chemotherapy.5,9,11 In our experience, the majority of cases in the adolescent patient is due to malunion, nonunion or pseudoarthrosis of a medial epicondyle fracture. In contrast, adult patients more frequently present with stiffness due to degenerative conditions such as synovial chondromatosis, heterotopic ossification, or post-operative complications.7,14,17 In addition, adolescent patients usually have better tissue quality, better healing response, and may tolerate minimally invasive procedures like arthroscopic arthrolysis more effectively.
Furthermore, whenever no improvement is seen in the ROM, surgical treatment is usually indicated. However, making the decision to move on with surgery is not always straightforward. When is an open release necessary and in which cases will the arthroscopic approach provide similar or even superior outcomes? Especially in the adolescent patient, where skeletal maturity must be taken into consideration and biological responses can be unpredictable. What initially looks like a fixed deformity may partially resolve over time, or in contrast, could progress despite conservative measures. This uncertainty complicates the decision-making process and timing of surgical intervention. Thus, investigating the literature is essential to evaluate how these types of surgical approaches perform, particularly in the adolescent population. Table 1 provides a general overview of the literature discussed in this section.
While both techniques demonstrated similar outcomes in regard to functional improvement, the recent literature tends to favor arthroscopic procedures due to the lower complication and revision rates, although numbers vary between studies.23 In the past few years, arthroscopic arthrolysis has gained popularity due to its minimally invasive nature, but it is more technically demanding than the open approach.23 The choice between the two approaches depend on multiple factors. The presence of intra- or extra-articular pathologies, degree of flexion contracture, prior surgical history, and the visibility or stability of the ulnar nerve all play an important role in the restoration of ROM. In addition, open release of the ulnar nerve should be considered when the ROM is under 90 degrees, or when flexion deficit persists where the posterior bundle of the medial collateral ligament has to be incised. In the latter, anterior transposition is necessary.
However, the literature does not universally agree upon all these indications. For example, Graves et al. and Siemensma et al.20,21 both mention heterotopic ossification to play a key role in the management of elbow stiffness, as its location and involvement outside the joint capsule would be a challenge better managed through the open approach.20,21 In contrast, a clinical study done by Bachman et al.24 does not consider heterotopic ossification as a contraindication for arthroscopy, nor does it mention it to be a determining factor in surgical decision-making.24 Their single-surgeon study compared open and arthroscopic heterotopic ossification removals and found that there was no increase in major complication and reoperation rates when arthroscopy was used. This suggests that Bachman et al. had a less restrictive threshold for arthroscopic procedures, particularly among experienced surgeons who are comfortable with managing extra-articular pathologies. Their interpretations are a good starting point that highlight the differing perspectives between surgeons, one where accessibility and safety is prioritized, and the other leaning towards surgeon skill and minimally invasive procedures.
Another differing opinion between authors is the management of the ulnar nerve. Siemensma et al.21 state that the inability to localize or stabilize the ulnar nerve is a relative contraindication for the arthroscopic approach and recommend a fully open release in these cases.21 Graves et al.20 have a different strategy for such cases, as they vouch for performing the arthroscopic approach while managing the nerve through a concurrent open release.20 This way, they have the benefits of minimally invasive surgery, while also staying in control of the ulnar nerve. In addition, O’Driscoll et al.10 suggested that doing a limited open ulnar nerve decompression at the start of the surgery would prevent iatrogenic injury and traction neuropathy of the nerve post-operatively.
A common determining point whenever the choice has to be made between open and arthroscopic arthrolysis is the prior surgical history on the elbow. Chow et al.25 categorize previous elbow surgery as one of the contraindications to the arthroscopic approach, which may be due to the multiple incisions or altered local anatomy.25 They reported it to be more challenging and associated with higher complication rates.25 The risk of iatrogenic injuries and limited arthroscopic access would favor an open release for better control.26–28 On the other hand, a study by Leschinger et al.29 indicated that prior surgical history of the elbow should not exclude arthroscopic arthrolysis, which probably was achieved through detailed pre-operative planning and associated with great success rates.29 In their study, they compared clinical outcomes of patients undergoing arthroscopic and open arthrolysis, assessing improvements in ROM, complication rates, and post-operative recovery. In one of the comparing groups, they included 13 patients (43.3%) with a history of prior elbow surgery.29 In our clinical experience, the use of imaging modalities to navigate through the anatomical landmarks intraoperatively and guide portal placement is the way to perform arthroscopy safely and effectively, even in complex cases with prior surgical history.
At our center, as we are familiar with complex elbow arthroscopy, we have been able to safely expand our indications for arthroscopic arthrolysis. Even though this technique is very demanding and is associated with a flat learning curve, our team has been able to overcome these barriers due to the high volume of these procedures. A technical note worth mentioning is that in cases where intra-articular access is hindered, typically caused by significant scarring or capsular distortion due to previous surgeries, senior author (C.K.) makes use of an extra-articular approach. In these situations, the procedure starts outside the joint and is followed by a capsulotomy, which allows the rest of the arthrolysis to proceed safely.30,31 Figure 3 presents arthroscopic images taken during the procedure.
_release_of_the_anterior_capsule_(ac)_intr.png)
Although open arthrolysis is currently the gold standard for treating severe and complex cases of elbow stiffness, its techniques leave limited room for innovation compared to the evolving arthroscopic approaches.32–34 This is why, the attention should be shifted toward expanding arthroscopic alternatives, especially in younger patients where less invasive procedures should be considered. A study by Hilgersom et al.35 reported an 86 percent return-to-sport rate and a low overall complication rate of 3.7 percent in the pediatric patient, which supports arthroscopy as a safe and viable approach compared to the open technique.35 Additionally, in the prospective study by Leschinger et al.34 that compared the short term results of arthroscopic and open procedures, they reported that arthroscopic arthrolysis was associated with a greater reduction in post-operative pain and improved DASH scores, suggesting that arthroscopy may offer better functional advantages over open surgery.34 However, their study was not limited to the child or adolescent patient.
In addition, whenever faced with cases of deformed elbows, severe burns or revision surgeries, arthroscopic arthrolysis tends to be difficult to perform.36,37 When we compare both surgical options, some of the advantages of the arthroscopic procedure are improved joint visualization, decreased rates of infection, and faster return to activities.31,38 Several cases have shown the improvements in the ulnohumeral motion that open release can lead to in post-traumatic elbow stiffness, with increased ROM up to 60% in flexion/extension and 58% in pronation/supination.7,39 For arthroscopic release, the results were similar as the numbers of improvement in ROM, which ranged from 29 to 70%.7,39 In regard to the adolescent patient, recent studies established that without joint incongruity or degeneration, adolescents can achieve results comparable to those seen in adults.35,40 Figures 4 demonstrates the functional improvement achieved following arthrolysis, with intraoperative assessment and immediate gain of ROM.
_limited_extension_prior_to_the_arthroscopic_arthrolysis_procedure._(b)_full_extension_.png)
CONCLUSION & FUTURE DIRECTIONS
In this article, we provided an overview of post-traumatic elbow stiffness in adolescents, went over current diagnostic modalities, treatment options, and surgical approaches. In addition, a particular emphasis was given to the evolving role of arthroscopic techniques in treating elbow stiffness. Post-traumatic elbow stiffness in the adolescent patient presents a complex challenge, as it requires an individualized approach based on multiple factors. Currently, open arthrolysis of the elbow remains the most widely used option, particularly in severe cases. However, with its technique slowly reaching the ceiling in terms of potential improvements, our efforts should shift towards refining the arthroscopic procedures that will deliver greater outcomes as more research emerges. Further research is needed to evaluate long-term outcomes, complication rates and learning curves associated with the adolescent and pediatric population. As well as comparative studies with open approaches should be focused on to determine optimal recovery rates, recurrence rates, and joint integrity over time. Notably, at our clinic, we favor the approach that makes use of arthroscopic arthrolysis, which has been safer and gained better functional outcomes in the adolescent population than the open approach.
Corresponding author
Mikail Chatzivasiliadis
Medical Student
Department of Spine and Deformities, European Interbalkan Medical Center, Thessaloniki, Greece
Aristotle University School of Medicine, Thessaloniki, Greece
tel: 0031642006024
e-mail: mikail@chatzi.com
Acknowledgements
None
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Christos Koukos, Paulo Arrigoni and Stylianos Kapetanakis. The first draft of the manuscript was written by Mikail Chatzivasiliadis and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Informed Consent
Written informed consent was obtained from the patient and the parents for publication of this study and any accompanying images.