

Introduction
Pneumonia, ventilator dependence, and unplanned intubation are all dangerous pulmonary complications that can occur after femoral open reduction and internal fixation (ORIF).1,2 Understanding the risk factors leading to the complications following these procedures is important for patient survival and overall health.3,4 Blood clots caused by the broken femur can travel to the lungs, causing pulmonary embolism5,6 and the internal nailing used for the internal fixation can exacerbate pulmonary symptoms.7,8 To date, this topic has limited research,9 as most studies focus broadly on major orthopedic surgeries in general,10,11 or lump femoral ORIF with other lower extremity procedures, without isolating predictors for these specific complications.12 This study aimed to identify predictors of pulmonary complications including unplanned intubation within 30 days of femoral open reduction and internal fixation, using the large NSQIP surgical database.13,14
Methods
This study used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, which is a de-identified registry that includes the surgical data from over 700 hospitals each year.15,16 The NSQIP database was queried for patients undergoing femoral open reduction and internal fixation. The primary outcomes measured were the incidences of postoperative pneumonia, ventilator dependence greater than 48 hours, and unplanned intubation within 30 days following surgery.17 Group characteristics, including sex and comorbidities, were compared to assess significant differences between patients who did and did not experience pulmonary complications. Additional predictors examined for each of these postoperative outcomes included white blood cell count (WBC), operating time, American Society of Anesthesiologists (ASA) physical status classification, and comorbidities such as smoking, steroid use, functional status, and use of various types of anesthesia (Fig. 2). Multivariate logistic regression models were performed to analyze the significance of these predictors.18 Within this study, R2 values were used to determine the reliability of the correlation of the predictors and the outcomes.19 For every model, statistical significance was set at p<0.05.
Results
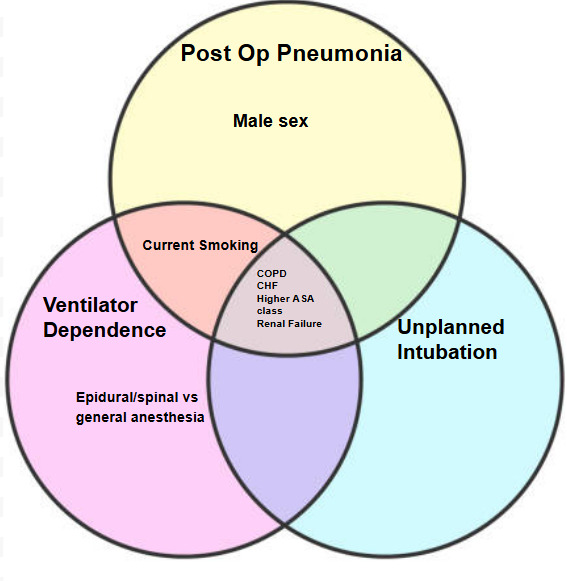
Figure 1 shows COPD and higher ASA class were strong predictors across all three pulmonary complications, demonstrating their role in risk assessment. Additionally, spinal or epidural anesthesia was significantly associated with ventilator dependence, suggesting a possible link to delayed respiratory recovery. Significant independent predictors were found for all three pulmonary complications analyzed.


Significant independent predictors for postoperative pneumonia included male sex (OR 1.87, p<0.0001), chronic obstructive pulmonary disease (COPD) (OR 2.14, p<0.0001), congestive heart failure (CHF) (OR 1.45, p=0.0015), renal failure (OR 2.49, p<0.0001), higher ASA classification (p<0.0001), and current smoking (OR 1.21, p=0.0099). For ventilator dependence >48 hours, significant predictors were COPD (OR 2.49, p<0.0001), CHF (OR 1.26, p=0.0067), renal failure (OR 1.85, p<0.0001), higher ASA class (p<0.0001), smoking (OR 2.78, p<0.0001), and epidural or spinal anesthesia compared to general anesthesia (OR 2.61, p=0.0017). For unplanned intubation, COPD (OR 2.17, p<0.0001), CHF (OR 1.45, p=0.0015), renal failure (OR 2.49, p<0.0001), and higher ASA class were significant predictors (Figure 2). There is significant overlap between predictors, with COPD, CHF, higher ASA class, and renal failure being shared between each outcome (Figure 3).

Discussion
The generated results align with current literature regarding pulmonary complications after femoral ORIF,20–22 although research on this topic is limited.9 Lifestyle factors, such as smoking, had a notable impact on pulmonary complications, indicating the importance of preoperative optimization when reducing risk.3,10 Patients exhibiting the high-risk factors identified in this analysis should be monitored more closely post operation, with higher vigilance regarding respiratory complications.2,4 A significant finding was that the use of epidural or spinal anesthesia was associated with greater odds of prolonged ventilator dependence compared to general anesthesia. This may be due to the confounding factor that patients with higher risk would have a higher likelihood of receiving epidural or spinal anesthesia opposed to general anesthesia.2 This observation aligns with previous studies comparing anesthesia types for hip and femur surgeries.2,22 The implications of this are clinically significant. If spinal or epidural anesthesia increases the risk of pulmonary complications in groups with these risk factors, there is a need for better monitoring, early mobilization strategies, and respiratory interventions to mitigate risk. Future research should cover what should be done to lower these risk factors for better pulmonary outcomes post operation.12 While spinal or epidural anesthesia is typically considered safer than general anesthesia and would be used for people with higher ASA class, it is possible that this type of anesthesia may also cause delays in the recovery of respiratory function in some patients, especially patients with other risk factors like preexisting pulmonary disease. Spinal anesthesia can reduce intercostal muscle function, causing prolonged respiratory depression in vulnerable populations.23
Pertaining to this analysis, the area under the curve (AUC) value corresponded to the reliability of the models in their ability to explain the postoperative outcomes. The AUC values generated for unplanned intubation, ventilation, and pneumonia were .69046, .73822, and .70324 respectively. These are modest values.. The corresponding R2 values for the whole model analyses of pneumonia, ventilation, and unplanned intubation were .0588, .0680, and .0436. Typically an R2 value above 0.15 is considered reasonable in clinical medicine, thus these values suggest that the current models do not adequately explain the variance. Additionally, the odds ratios used to determine the significance of the predictors in this study were used to compare the odds in which various events were to occur in relation to each other.24
The results of this study can be utilized by hospitals and healthcare providers to preemptively screen for risks of postoperative pulmonary complications following femoral open reduction and internal fixation. This can be beneficial to reduce the price and duration of patients’ hospital length of stay and diminish the possibility of negative outcomes surfacing post operation.25
Conclusion
In this database, higher ASA class, COPD, CHF, renal failure, male sex, and smoking were independently associated with increased risk of pulmonary complications after femoral ORIF.
This information can help surgeons further understand the pulmonary risks in this procedure.
Surgeons can monitor high-risk patients more closely. Patients can be encouraged to lower their risks of pulmonary complications through lifestyle changes, especially regarding variables like smoking.