


I. INTRODUCTION
Lunate and perilunate dislocations are uncommon injuries, accounting for approximately 7% of wrist trauma.1 However, they are frequently missed—up to 25% at initial presentation.2 Neglected lunate dislocation can result in restricted wrist motion and complications including wrist osteoarthritis, median nerve compressive neuropathy3 and flexor tendon injury.4–6
We report a case of multiple flexor tendon ruptures secondary to a neglected lunate dislocation diagnosed four years after the index trauma. A 45-year-old woman had sustained a wrist injury four years earlier; the volar lunate dislocation was missed. Two weeks before presentation she developed atraumatic loss of active flexion of the middle and ring fingers. Examination demonstrated injury to the flexor tendons of digits III and IV in association with a volar lunate dislocation, and surgery was indicated. Intraoperatively, we identified ruptures of the flexor digitorum profundus (FDP) to digits III and IV and the flexor digitorum superficialis (FDS) to digit IV at the level of the volarly displaced lunate. We performed lunate excision, reconstruction of the FDP tendons to digits III and IV with an autologous palmaris longus tendon graft, and direct repair of the FDS to digit IV. At 1-year follow-up, wrist function was good and the patient had fully recovered active flexion of digits III and IV.
II. CASE REPORT
A 45-year-old woman sustained a left wrist injury in 2020 after a fall onto an outstretched hand. She was evaluated at a local facility, but a left lunate dislocation was missed. Two weeks prior to admission she developed atraumatic loss of active flexion of the left III and IV fingers. On examination, injury to the left flexor tendons of digits III and IV was suspected. Radiographs and CT scan demonstrated a volar dislocation of the lunate. The patient underwent surgery on October 1, 2024.
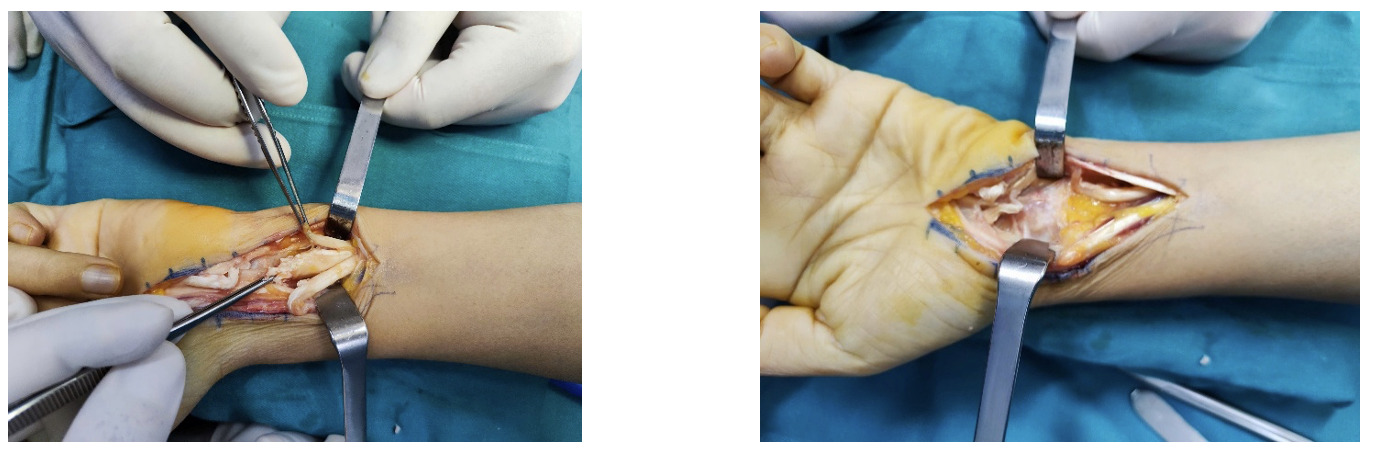
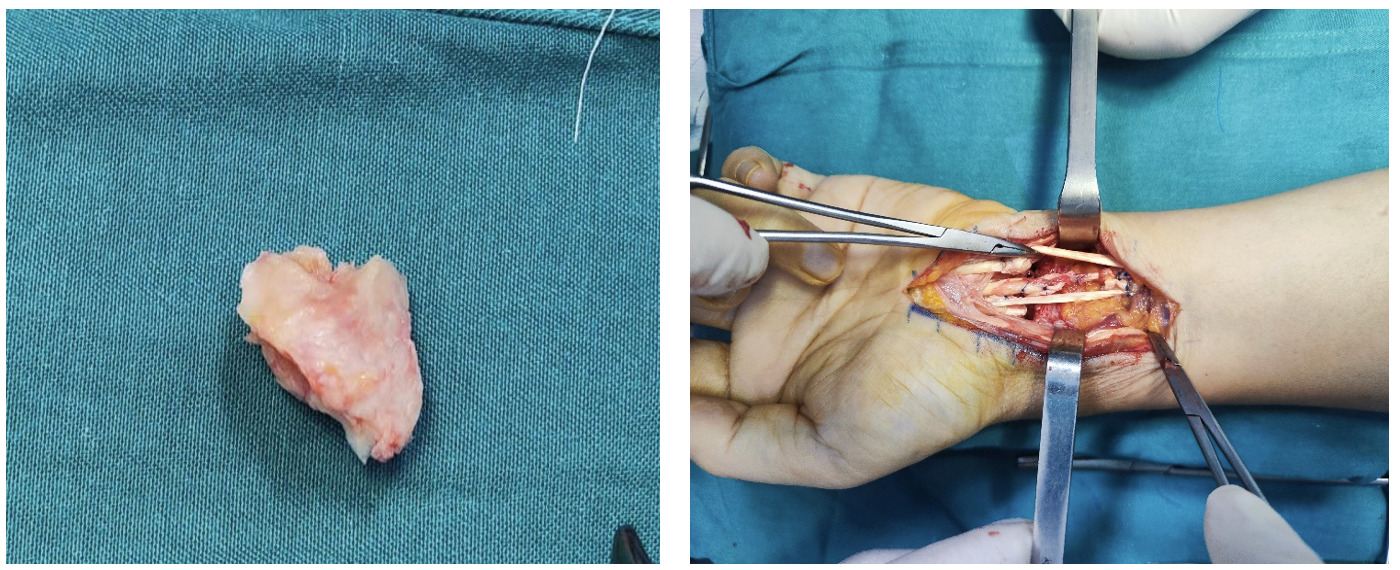
Through a volar approach, we identified ruptures of the FDP to digits III and IV and of the FDS to digit IV at the level of the volar lunate dislocation. The FDP tendons to digits III and IV were retracted with a 2-cm segmental defect and poor tendon quality, precluding direct end-to-end repair. The FDS to digit IV was retracted ~1 cm with good tendon quality. We therefore performed excision of the lunate, FDP reconstruction for digits III and IV using an autologous palmaris longus tendon graft with Pulvertaft technique, and direct repair of the FDS to digit IV using modified Kessler technique.
Postoperatively, the wrist and hand were immobilized in a short forearm cast for 4 weeks, followed by supervised rehabilitation focusing on digital flexion–extension. At 4 months and 1 year postoperatively, wrist flexion was 80° and extension 30°, and the digits achieved full active range of motion. Follow-up radiographs showed no radiocarpal degenerative changes.

_to_digits_.png)
_to_digit_iv_usi.png)


III. DISCUSSION
Perilunate dislocation is an uncommon injury, accounting for approximately 7% of wrist trauma.1 Because of its rarity, it is frequently missed at the initial assessment with a reported rate of up to 25%.2 Therefore careful clinical evaluation and meticulous review of true AP and lateral wrist Xray are essential.
Lunate dislocation corresponds to stage IV of Mayfield’s progressive perilunate instability and to stage 2 in the Herzberg classification.7 Lunate dislocations are categorized as volar or dorsal, with the dorsal pattern being far more common.2 In volar lunate dislocation, the short radiolunate ligament is the sole structure preventing the lunate from completely migrating into the carpal tunnel.8
For acute lunate dislocations, treatment options include closed reduction and cast immobilization, percutaneous K-wire fixation, or open reduction with ligament repair/reconstruction. In chronic presentations—particularly beyond 4 months—the lunate is generally irreducible; surgical options then typically include lunate excision, proximal row carpectomy, or four-corner arthrodesis .9
When the lunate dislocates volarly, it can cause carpal tunnel compression and chronic attritional abrasion of the flexor tendons during repetitive motion, which over time may lead to flexor tendon rupture at the wrist level. In such cases, tendon damage often spans a long segment, and the tendon ends are of poor quality.
There have been prior reports of flexor tendon ruptures to neglected lunate dislocation, with surgical strategies such as: lunate excision with side-to-side tenodesis of the ring and small finger FDP tendons to the middle finger FDP,4 lunate excision with scaphocapitate fusion, followed by staged flexor tendon reconstruction,5 and lunate excision with primary repair of the FDS to digits II–III plus palmaris longus autograft for the FDS to digit V and the FDP to digits III–IV.6
In our patient, the lunate dislocation had been neglected for 4 years. Preoperative radiographs and CT showed no radiocarpal degenerative changes. Intraoperatively, the FDS to digit IV had a short retraction with good tendon quality, allowing direct end-to-end repair; by contrast, the FDP to digits III and IV were retracted (~2 cm) with poor-quality ends. Accordingly, we performed lunate excision, direct repair of the FDS to digit IV, and reconstruction of the FDP to digits III and IV using an autologous palmaris longus tendon graft.
IV. CONCLUSION
Perilunate dislocation is rare and easily missed; over time it can lead to median nerve involvement and wrist flexor tendon injury. Surgical reconstruction of the wrist flexor tendons with an auto palmaris longus graft, combined with lunate excision, yields good clinical outcomes.