

Introduction
Clavicle fractures account for about 5% of all fractures in adults and 44% of shoulder girdle injuries, among which acromial fractures occur in 10–28% of cases.1 These injuries are characterized by complex anatomical structures and high instability, which significantly complicate their treatment. Despite the variety of available treatment methods, the incidence of complications such as deformity, pseudoarthrosis, osteomyelitis, and limb dysfunction reaches 25–35%.2
Conservative treatment requires prolonged immobilization, which extends the period of disability, while the high risk of fracture non-union often necessitates repeated hospitalizations. Even in cases of successful bone fusion, complications frequently occur, including shortening, malalignment, or improper union of the clavicle, which are accompanied by functional impairment.3
Surgical methods, including plate osteosynthesis and intramedullary fixation, are used to achieve anatomical reduction and to shorten rehabilitation time.4 However, intramedullary osteosynthesis is associated with complications such as infection, osteomyelitis, implant deformation or breakage, and insufficient fixation stability.5 Plate osteosynthesis is considered the gold standard, as it provides rigid fixation and rotational stability.6 Nevertheless, existing plate designs are often not well adapted to the anatomical curvature of the clavicle, necessitating intraoperative bending, which weakens the structural integrity and increases the risk of metal erosion.7 Additional risks are associated with empty screw holes near the fracture line, which reduce the overall fixation stability.8
The mismatch between the stiffness of metallic implants and that of bone tissue disrupts physiological load transfer, promotes bone resorption, and weakens fixation.9 For instance, the elastic modulus of Ti–6Al–4V alloy (124 GPa) significantly exceeds that of cancellous (3 GPa) and cortical (12–17 GPa) bone.10 This discrepancy leads to stress concentration at the bone–implant interface, impairing osseointegration and long-term stability.11 Reducing implant stiffness decreases the stress transmitted to bone and promotes a more uniform distribution of mechanical loads.12 Ideally, an implant should provide sufficient rigidity during the early stages of fracture healing while allowing a certain degree of flexibility during later stages of consolidation.
A promising direction in modern osteosynthesis is the development of implants that replicate both the morphological shape and the elastomechanical properties of bone, thereby improving biological integration and functional outcomes. However, excessive reduction in implant strength may compromise stability and increase the risk of fixation failure, highlighting the need to design new implants that are anatomically adapted to the clavicle and meet contemporary biomechanical requirements.13
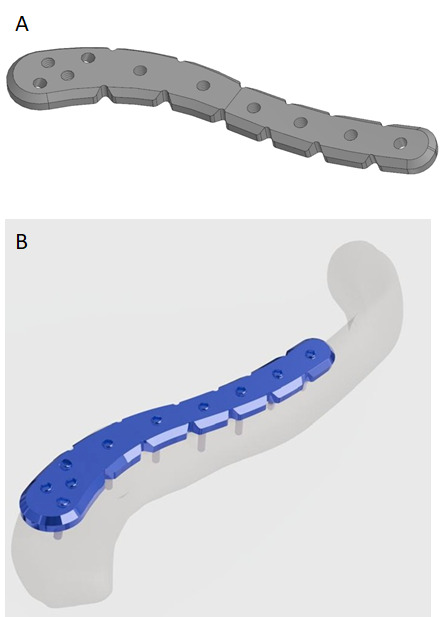
The newly developed clavicle plate, similar to existing models (ChM, Trauson), features an expanded lateral end designed for fixation at the acromial portion of the clavicle. Unlike the ChM analogue, in the expanded segment of the plate, the holes are oriented in two different directions—two directed posteriorly and two anteriorly—providing enhanced rigidity of fixation. In contrast to the Trauson plate, all holes in the developed implant are of uniform size and internally threaded to accommodate 3.5 mm locking screws. The multidirectional orientation of the holes allows for more reliable stabilization of bone fragments and secure attachment of the plate to the clavicle.
In this study, our original design - an anatomical fixation plate for the acromial end of the clavicle (Figure 1) - was used for internal fixation of a distal clavicle fracture in an adult patient.
__three-dimensional_stl_model_of_the_clavic.png)
Case Presentation
Ethical Considerations
This case report was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Local Ethical Committee of the National Scientific Center of Traumatology and Orthopedics named after Academician N. D. Batpenov (Approval No. 2, July 19, 2023).
Patient D., a 39-year-old male of Kazakh origin, presented with right shoulder pain and impaired upper limb function following a fall onto the right shoulder approximately two hours prior to admission. The symptoms developed immediately after the injury. The right upper limb was initially immobilized using a sling bandage. Upon removal, swelling and deformity of the right shoulder were observed. Palpation revealed marked tenderness, crepitus, and abnormal mobility at the acromial end of the clavicle. Shoulder motion was restricted due to pain, but there were no signs of sensory deficits or numbness in the affected limb. A physical examination was performed, followed by radiographic evaluation.
X-ray imaging demonstrated a displaced comminuted fracture of the distal clavicle (Figure 2), with the proximal fragment displaced superiorly. The fracture was classified as type IIb according to Neer.

Surgical Procedure
After obtaining written informed consent, open reduction and internal fixation were performed the same day under general endotracheal anesthesia using the newly designed anatomical plate. Following thorough four-stage antiseptic preparation, a 7.0 cm incision was made over the acromial end of the clavicle. Both sharp and blunt dissection were carried out, exposing an oblique comminuted fracture with partial disruption of the coracoclavicular ligament; however, the acromioclavicular ligament remained intact.
The bone fragments were anatomically reduced, and a custom-made plate was positioned on the superior surface of the clavicle. It was temporarily held in place with Kocher clamps and then fixed with seven locking screws (Figure 3). Under fluoroscopic guidance, proper alignment was confirmed, and any residual displacement was corrected. Hemostasis was achieved using electrocoagulation. The wound was closed in layers with interrupted sutures, covered with a sterile dressing, and the limb was immobilized in a sling. Estimated intraoperative blood loss was 100 mL.

Active hand and wrist movements, isometric contractions of the biceps and forearm muscles, and elbow flexion–extension exercises were initiated on postoperative day 2.
Results and Follow-Up
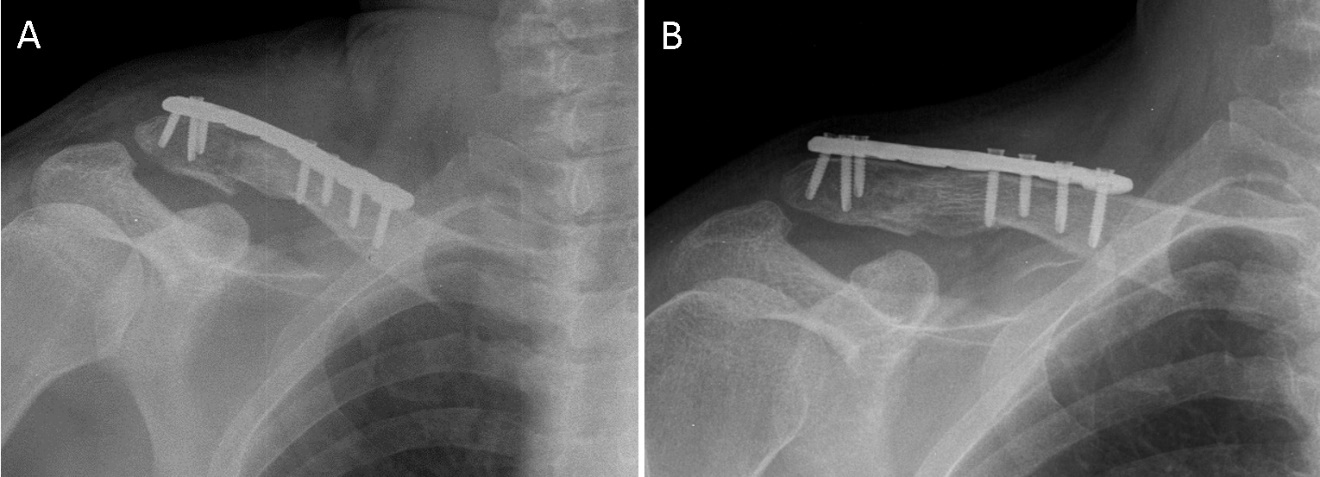
Postoperative radiographs confirmed anatomical alignment of the fracture fragments and stable osteosynthesis using the developed plate and screws (Figure 4A). The bone and implant positions were satisfactory. The patient followed a standard orthopedic regimen, including sling immobilization for 14 days. From day 15, supervised horizontal shoulder movements were initiated, and by the fourth postoperative week, gradual active shoulder exercises were introduced as tolerated.
_immediately_after_surgery__(b)_co.jpeg)
The postoperative course was uneventful. Daily wound dressings were performed for 10 days, with primary healing achieved and sutures removed on day 11. The patient adhered to the prescribed rehabilitation plan, including immobilization and restricted shoulder movement for 14 days.
At the two-month follow-up, radiographs showed maintained reduction, stable osteosynthesis, and radiological signs of fracture healing (Figure 4B). The patient reported no pain or discomfort, and physical examination revealed no asymmetry of the shoulders and a well-healed postoperative scar without inflammation.
The right shoulder joint exhibited a full, pain-free range of motion. Functional assessment using the Constant Shoulder Score and the ASES questionnaire demonstrated an 11-point difference between the injured and healthy sides, indicating a good clinical outcome. The ASES score of 85 reflected an excellent functional result.
Following the final evaluation, the patient was advised to avoid strenuous physical activity.
Management and Outcomes
Clavicle fractures, particularly those involving the lateral end, present a significant clinical challenge due to their anatomical complexity and high instability. Modern treatment strategies include both conservative and surgical methods, with the latter increasingly favored because of the high risk of nonunion and deformity following nonoperative management, which often leads to functional impairment and reduced quality of life.14,15
Various surgical options, such as plate and intramedullary fixation, have specific advantages and limitations. Plate osteosynthesis provides reliable fixation and excellent rotational stability but may cause soft-tissue irritation or require implant removal. In contrast, intramedullary fixation is less invasive and reduces operative time and infection risk but offers inferior stability in complex fractures.16 The choice of treatment should therefore be individualized, considering fracture morphology, displacement, and patient-specific anatomy.17
Type IIB fractures according to the Cho classification are particularly unstable due to coracoclavicular ligament disruption. In such cases, standard plate fixation may be insufficient, and combining plate fixation with ligament reconstruction yields better outcomes.18 Hook plates, although effective in some cases, are associated with acromioclavicular joint degeneration and a frequent need for implant removal.19
Anatomically contoured plates that replicate the clavicle’s natural curvature and distribute mechanical loads more evenly represent an important advancement. The plate used in this case incorporated multidirectional screw-hole orientation to enhance fixation stability and minimize complications, consistent with modern biomechanical principles.13 The patient underwent open reduction and internal fixation with this implant, followed by standard postoperative rehabilitation. The recovery was uneventful, and radiographic evaluation four weeks postoperatively demonstrated satisfactory fracture consolidation, confirming the stability of fixation.
Overall, this case demonstrates that anatomically designed plates can improve clinical outcomes, reduce surgical trauma, and minimize implant-related complications. Future research should further explore biomechanical optimization and patient-specific plate design.20
Conclusion
In conclusion, we propose a standardized surgical approach for adult patients with fractures of the acromial end of the clavicle, particularly those classified as Neer type IIB and type V. Open reduction and internal fixation using an anatomically contoured plate positioned on the superior surface of the clavicle was applied to restore the distal clavicular structure and ensure stable fixation. In this case, satisfactory clinical and functional outcomes were achieved, supporting the potential clinical applicability of this technique.
Although the present report describes a single patient, the same procedure has also been successfully applied in a series of additional cases, demonstrating consistently favorable results. Nevertheless, further studies with larger patient cohorts and longer follow-up periods are required to comprehensively assess long-term clinical outcomes, particularly with respect to the potential development of post-traumatic osteoarthritis.
Disclosure
The author(s) report no conflicts of interest in this work.
Funding
This research was funded by the Committee of Science of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. BR21881815).
Ethical Approval
The case report was conducted in accordance with the Declaration of Helsinki and approved by the Local Ethical Board of the National Scientific Center of Traumatology and Orthopedics, named after academician N. D. Batpenov (July 19, 2023/No. 2).
Informed Consent
The patient gave written informed consent for the publication of her clinical data.