Introduction
A psoas abscess is classified as a buildup of pus in the psoas muscle, which overlies the vertebral column, playing a vital role in hip flexion and stability of the lumbar spine.1,2 The psoas muscle is positioned adjacent to several critical anatomical structures, such as the abdominal lymph nodes and the spinal column.3 Also termed psoitis, this rare condition results in a pyogenic collection on the iliopsoas muscle at the distal end of the origin of the psoas muscle.4 A psoas abscess incident in clinical care is rare, as only 12 cases are reported annually worldwide.5 This is likely due to the delay in diagnosis that results from the often vague presentation.
Common causative organisms of a psoas muscle abscess include Staphylococcus aureus, Streptococcus viridans, and Mycobacterium tuberculosis.5 The primary modality of treatment for consideration of a psoas muscle abscess is surgery, followed by intensive antibiotic therapy.5 Alternative treatments include surgical drainage followed by the administration of antibiotics.6
The main cause of a psoas muscle abscess is the spread of an infection from a nearby organ or body part, such as the hip, vertebrae, or gastrointestinal tract.7 Psoas muscle abscesses may develop through an infected aortitis, commonly observed in patients with an immunocompromised status, or through an infection in the urinary tract.8,9 The infection then travels from the urinary tract straight into the psoas muscle, causing an abscess to develop.9 A psoas muscle abscess typically presents with enigmatic symptomatology, but one of the main presenting symptoms is abdominal pain.4
There are two types of psoas muscle abscess: primary and secondary. A primary psoas muscle abscess forms when an initial infection is not distinguished to a certain anatomical region.10 Primary psoas muscle abscesses are created from hematogenous or lymphatic dissemination from a remote area and are caused by infections.11 Secondary psoas muscle abscesses are created by spread from nearby structures and can be caused by certain microorganisms, including anaerobic and enteric bacteria, responsible for the source of primary infection.7,11
Case Presentation
The patient is a 69-year-old female who presents to the emergency department due to new right-sided thigh pain that had developed over the last two to three days. The patient reports mild subjective fever, nausea, and intermittent dysuria. The pain in her thigh made her limp. Denies any chest pain, shortness of breath, vomiting, diarrhea, abdominal pain, focal weakness, or headache. Two weeks prior to presentation, she underwent left-sided stent placement for ureteral stones with hydronephrosis. She complained of persistent left leg pain. Her past medical history is significant for hypertension, hyperlipidemia, osteoarthritis, emphysema, and gastroesophageal reflux disease.
The patient’s vital signs were temperature 98°F, respiratory rate 16, blood pressure 163/97 mmHg, pulse 84, and oxygen saturation 94% on room air. Her physical examination was unremarkable except for bilateral costovertebral angle tenderness. No palpable masses were noted on abdominal or groin examination, although the patient appeared uncomfortable. Her neurological examination, including cranial nerves, motor and sensory, and reflexes, was normal.
The patient’s laboratory analysis revealed an unremarkable CBC with WBC 10.6, hemoglobin 13.6, hematocrit 39.5, and platelets 436. The chemistry panel demonstrated moderate hypokalemia with a potassium of 3.0. The remainder of the electrolytes, including creatinine and glucose, were unremarkable. Urinalysis demonstrated hematuria and pyuria. CT scan of the lumbar spine demonstrated a new rim-enhancing septated cystic appearing collection in the right psoas muscle measuring 2.7 * 1.4 * 2.6 centimeters, concerning for intramuscular abscess without a clear underlying source. Interventional radiology was consulted for drainage. One cc of serous sanguinous fluid was sent for culture. Gram stain demonstrated few WBC’s and no organisms. The patient was covered with broad-spectrum antibiotics including intravenous vancomycin, ceftriaxone, and metronidazole. The patient was given intravenous ketorolac, morphine, and methocarbamol for analgesia and muscle relaxant. And was admitted to the hospitalist service. She was discharged on hospital day 4, with improvement of her back pain.
The patient returned to the emergency department a week later, complaining of right lower back pain and right thigh pain that seemed better while she was receiving antibiotics in the hospital, but after being home for a few days, came back and got so bad that she could barely walk. Even passive motion of the leg made the pain worse. The patient did not have any instrumentation to her back besides the CT-guided percutaneous abscess drainage in the last admission. Her vital signs in this second visit were temperature 97.7, pulse 100, respiratory rate 18, blood pressure 141/82 mmHg, and 96% oxygen saturation on room air. Her physical examination was unremarkable except for significant pain upon movement of the back or right leg. She also looked ill. Rectal examination revealed normal tone and no saddle anesthesia. Laboratory analysis was unremarkable in this visit.
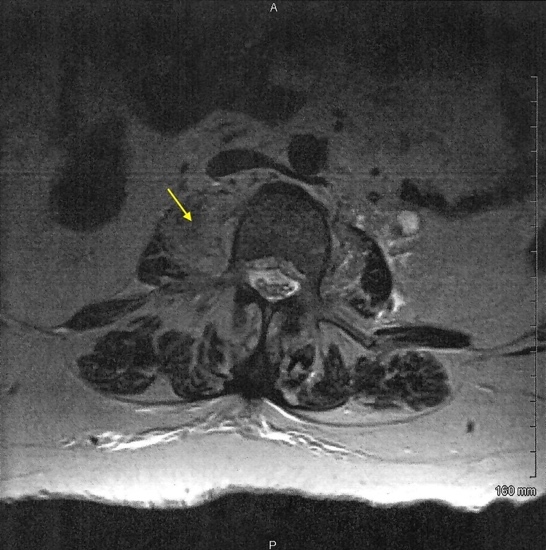
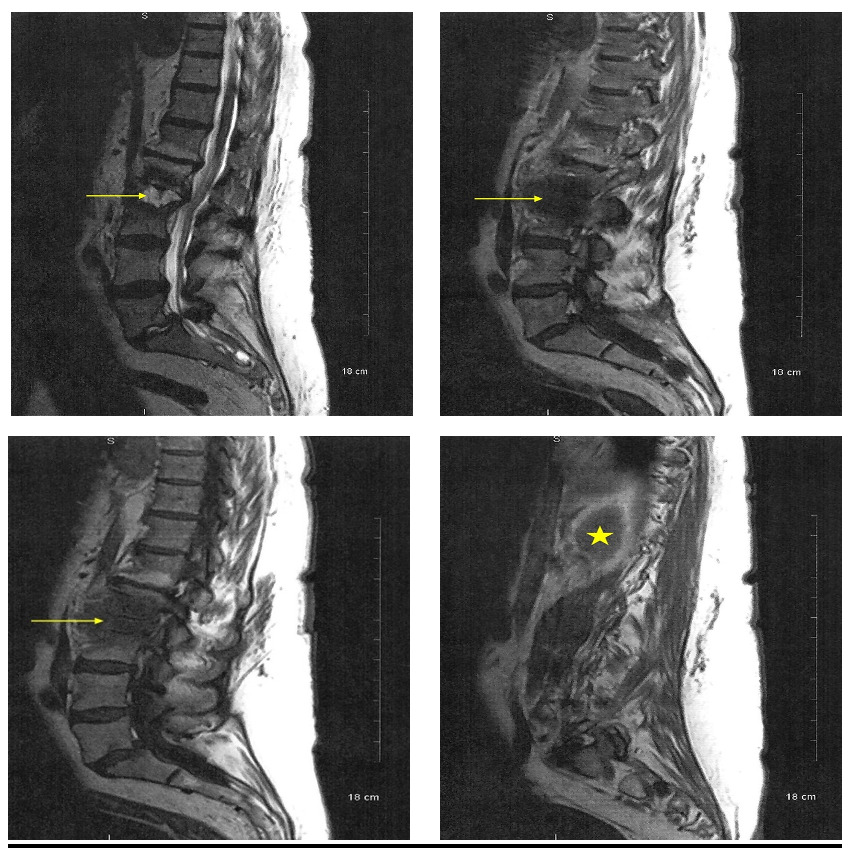
A lumbar spine MRI with and without IV contrast was obtained and revealed a low-density collection with peripheral heterogeneous and enhancement in the right psoas muscle measuring approximately 3cm by 1.5 cm extending to the right from the L2-L3 disk space (Figure 1). A subtle lucency along the inferior endplate of L2, suggestive of a developing fracture line, was also noted. The central canal of the L2-L3 space demonstrates moderate central canal stenosis. Also noted was an additional abscess more inferior to the original abscess. There was also a suggestion of septic synovitis of the posterior facets from L2 to L4 (Figure 2). Moderate hydro ureteral nephrosis was still present on the left. The left psoas muscle was normal.
The patient was again admitted to the hospital for neurosurgical and infectious disease consultations.
.jpeg)
.png)
Discussion
Characteristic presenting symptoms of a psoas muscle abscess are back pain, vague abdominal pain, fever, limp, malaise, weight loss, and a groin lump. There are various treatments that are effective in treating a psoas muscle abscess.12 The first line of treatment is usually broad-spectrum antibiotic therapy. Surgical drainage represented the previous standard procedures in previous clinical practices, but percutaneous drainage is a modern technique utilising a safer and more effective procedure and is much preferred now. New research has proven that some smaller abscesses can be treated solely with antibiotics and without drainage.12
Treatments tend to vary based on criteria such as mode of spread and size of the psoas muscle abscess. Antibiotic treatment is recommended for all abscesses; however, surgical drainage isn’t always necessary, especially considering the invasive nature of the procedure.13 The first line of treatment is antibiotic therapy, and the next steps are determined based on the efficacy of the initial antibiotic treatment. If the abscess is still large, then surgical drainage is required. However, if the initial antibiotic treatment reduces the size of the abscess, then subsequent surgical drainage may not be necessary, and the patient can be continued to be managed with further administration of antibiotics.13
Psoas muscle abscesses are also found in certain rarer presentations. In one case described by Lucia MH et. al, a patient presenting with prostate cancer developed a secondary psoas muscle abscess from contiguous spread from lumbar osteomyelitis. The osteomyelitis spread hematogenously or through local infection from nearby organs and tissues, causing the development of the psoas muscle abscess.14 In another case described by Diaco ND et. al, a patient with chronic lymphocytic leukemia developed a psoas muscle abscess due to Mycobacterium avian. The infection originated in the lymph nodes, and then, a primary psoas muscle abscess was developed from the lymphatic spread of the Mycobacterium avium.15 In an article described by Al-Khafaji MQ et. al, management of a psoas muscle abscess using an MRI scan to diagnose the abscess and following with a CT scan for drainage guidance provided a methodology for better efficacy in the treatment of a psoas muscle abscess.16
Conclusion
In this case study, the patient had developed a psoas muscle abscess and presented with right-sided thigh pain. The infection had also spread to the spine, leading to septic synovitis. Despite being treated with broad spectrum antibiotics and drainage of the collection, the patient was readmitted to the emergency department only a week later, exhibiting worsening symptoms of right lower back pain and right thigh pain. MRI had shown a low-density collection with peripheral heterogeneity and enhancement in the right psoas muscle. Reasons for initial treatment failure in such cases could include inadequate removal of the complete abscess or rapid regrowth due to parallel infection in the body. The patient had also undergone left-sided stent placement for ureteral stones with hydronephrosis two weeks before the psoas muscle abscess was discovered. One week after the psoas muscle abscess was removed, moderate hydroureteral nephrosis was still present in the same location.