Introduction
Total knee arthroplasty (TKA) is a common surgical treatment for severe osteoarthritis that alleviates knee pain by replacing the damaged knee joint with an artificial one. Osteoarthritis is a degenerative joint disease in which the cartilage on the ends of bones wears down, causing stiffness, pain, and a reduced range of motion. In 2023, the American Joint Replacement Registry reported around 1.9 million TKA procedures worldwide.1 This number is expected to increase in the next decade as the population ages and the prevalence of osteoarthritis grows.2 This study will reveal the multiple factors that predict complications following TKA. Pulmonary complications, including prolonged postoperative ventilation, unplanned reintubation, and pneumonia, are amongst the most concerning and also most costly postoperative issues after TKA,3 as these conditions prolong hospitalization. The 5-item Modified Frailty Index (mFI-5) includes five key patient comorbidities which can predispose a patient to pulmonary complications after TKA and can help to predict risks and potentially improve postoperative outcomes in patients.
Methods
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database is a de-identified registry that includes yearly surgical data from over 700 hospitals. This database was used to select patients who underwent TKA (CPT-27447) from 2018 to 2022.4
Several clinically relevant predictors were included in the study’s analysis of pulmonary complications following TKAs. Predictors included were age, sex, BMI, ASA Class, operative time, smoking, preoperative steroid use, type of anesthesia, history of chronic obstructive pulmonary disease (COPD), history of Congestive Heart Failure (CHF), functional status (independent or not), and mFI-5. The mFI-5 defines 5 comorbidities that are predictive of postoperative complications.5 It gives a score based on the presence of the following health conditions:
-
Functional status (Partial or Total dependence for activities of daily living)
-
Diabetes Mellitus
-
COPD
-
CHF
-
Hypertension requiring medication
This index has been cited in various articles with regard to orthopedic surgeries, such as elective posterior lumbar fusions6 or repair of distal radius fractures,7 and non-orthopedic surgeries, such as Video-Assisted Thoracoscopic Surgery.8 In this analysis, an mFI-5 score greater than 1 has a strong correlation to pulmonary complications after TKA.
An initial univariate analysis was performed to determine statistically significant individual associations between each predictor and the outcomes of interest. All predictors were then run through a multivariate logistic regression model.9 The following results were analyzed for statistically significant association between predictors and each pulmonary outcome while accounting for external confounding factors such as age, BMI, and ASA classification. The variables identified from this step were labeled as independent risk factors for pulmonary complications in TKA.
The statistical analyses were conducted as a two-tailed hypothesis with a significance level of 0.05 (confidence interval of 95%).
Results
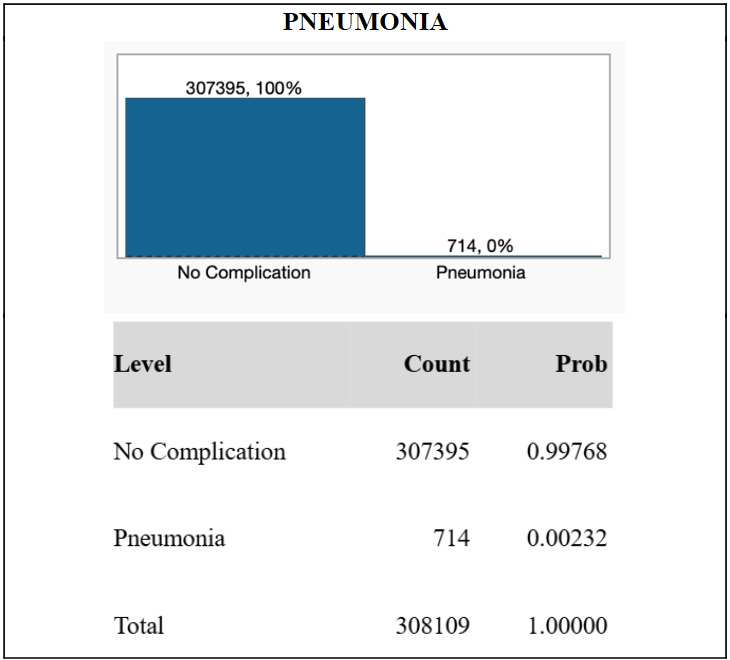
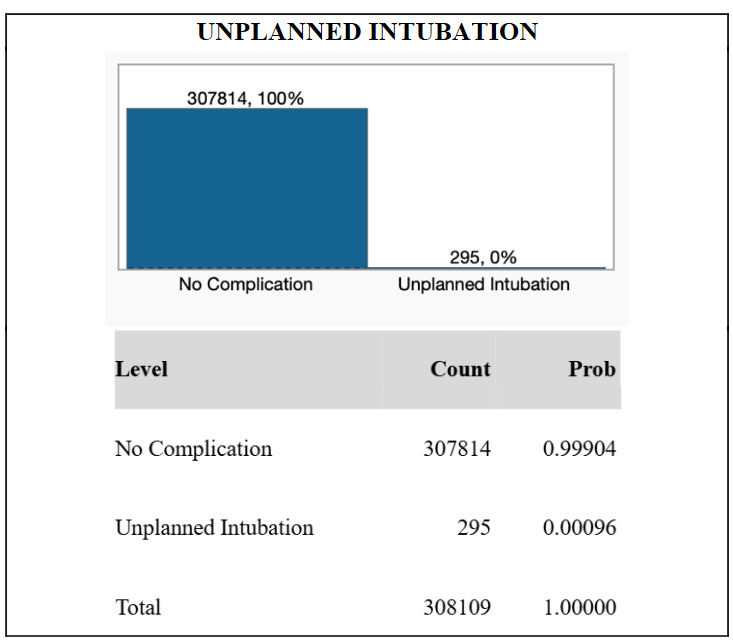
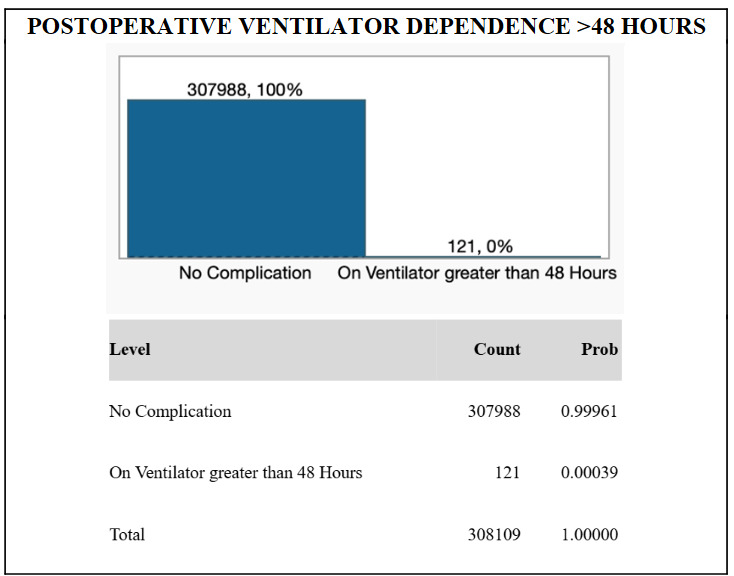
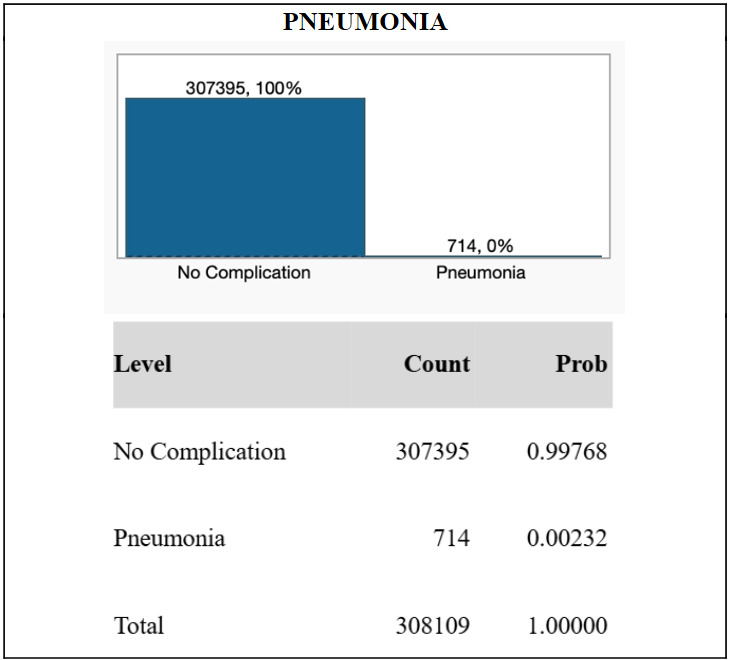
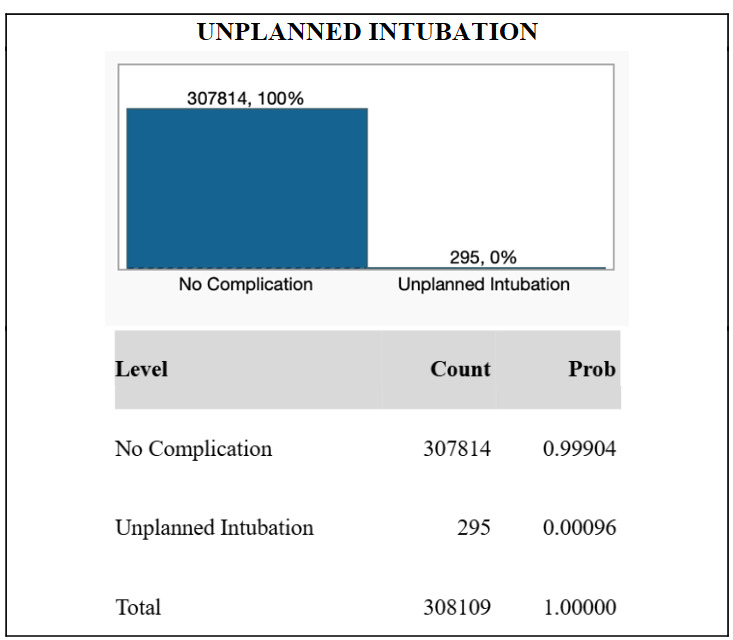
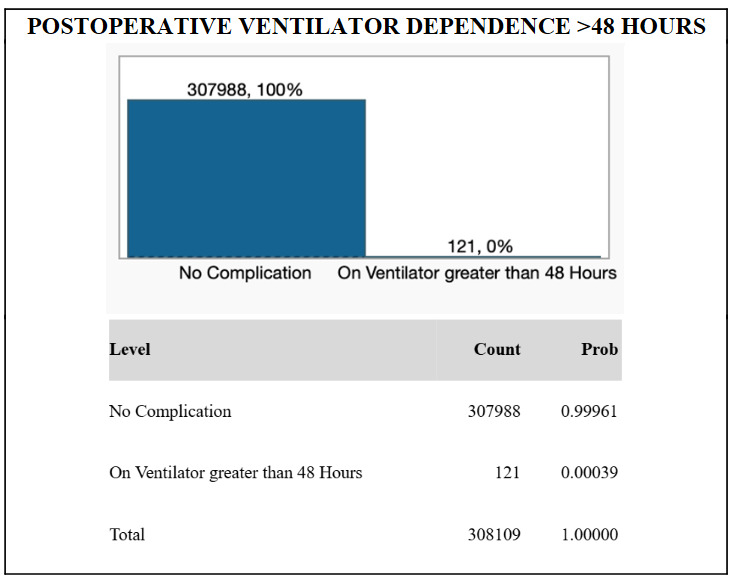
From the NSQIP database, de-identified information for N = 308,109 TKA patients were included in the study. The majority of patients in the study were female (60.7%), while 39.3% were male. The median age of the cohort was 68 years, and the median body mass index was 32.3. 121 patients (0.039%) exhibited postoperative ventilator dependence >48 hours. 295 patients (0.096%) required unplanned intubation. 714 patients (0.23%) suffered from postoperative pneumonia. These results are graphically displayed in Figures 1, 2, and 3.
The R2 for postoperative ventilator dependence was 4.3%, 5.3% for unplanned intubation, and 5.9% for pneumonia.10
Univariate analysis showed that, among all individual associations between predictors and postoperative ventilator dependence, statistically significant relationships included mFI-5, age, ASA class, smoking status, sex, preoperative steroid use, type of anesthesia used, and BMI.
For postoperative intubation, notable variables included mFI-5, ASA class, age, type of anesthesia used, sex, preoperative steroid use, smoking habits, and BMI.
In testing against pneumonia, significant variables included mFI-5, age, ASA class, smoking habits, type of anesthesia used, preoperative steroid use, sex, and BMI.
Multivariate logistic regression controlling for confounders demonstrated statistically significant increases in the rates of ventilator dependence, unplanned intubation, and pneumonia with increasing mFI-5 levels. Full results obtained from the multivariate logistic regression model are displayed in Table 1.
Discussion
This study on the effectiveness of the mFI-5 index demonstrates that it is a strong and independent predictor of postoperative pulmonary complications following TKA. Specifically, the mFI-5 creates a strong relationship between high frailty scores and significantly greater risks of pneumonia, unplanned reintubation, and ventilator dependence exceeding 48 hours after a TKA procedure. These higher scores were found to be associated with increased rates for all three pulmonary complications, even after adjusting for other risk factors including ASA class and age, meaning that they detect additional risk not found by existing measures.
Since this scale is closely correlated with the 3 major complications of postoperative ventilator dependence, intubation and pneumonia, it is a single tool which can be used to streamline patient risk assessments or serve as an addition to existing screening procedures for more reliable predictions. For instance, combining ASA classification with the mFI-5 is one way for surgeons and anesthesiologists to create a more uniform method of risk stratification.8 The 5 items included in the scale are concisely scored based on patient history without adding additional testing costs. Facilities can also use the scale for budgeting and planning as it is closely related to the number of resources used for surgical procedures.
The mFI-5 scale has been found to be useful not only in orthopedic surgeries; existing literature has shown it to correspond to risk in a variety of other surgical settings. Shah et al. established that the index was a predictor of 30-day complications and readmissions in adult spinal deformity patients.11 McGovern et al. showed that frailty scores were associated with malnutrition, systemic inflammation, and short-term outcomes in colorectal cancer surgery.12 Agathis et al. also established the utility of the mFI-5 in older patients undergoing hernia repair,13 while Khalafallah et al. showed that the index was predictive of mortality in brain tumor patients.14 Similarly, the study by Balasundaram et al. indicated that frailty was predictive of increased utilization of resources after endovascular aneurysm repair.15 These observations add further support to the universal use of the mFI-5 as a predictor of surgical complication risk.
However, limitations in this study exist and can affect the validity of its findings; the application of the ACS-NSQIP database is presented with possible variability from programming mistakes as well as variability in reporting from hospitals. The mFI-5 itself also does not address every major area of frailty such as cognition, nutrition, or mobility, which can influence pulmonary outcomes. Further, specific perioperative patient management factors including different ventilation methods or time for mobilization were not specified. Further studies can be done to determine the impact these factors have on risks for pulmonary complications and outcomes following surgical interventions.
Conclusion
The mFI-5 scale is shown to be a concise and useful system for predicting postoperative pulmonary complications following TKA. After the data analysis, it is seen that patients with a higher mFI score were associated with greater likelihood for pneumonia, unplanned intubation, and ventilator dependence (> 48 hours) after surgery.
This index can provide valuable information not only on TKA but potentially on any procedure that requires intubation and regional anesthesia.
The mFI-5 can further benefit patients by being used alongside other measurements, such as the ASA classification that assesses pre-surgical illness, to increase visibility and prepare TKA patients for postoperative complications. Further, aside from aiding other measurements in clinical screening, the mFI-5 holds enough simplicity to be used in under-resourced areas without adding much cost.
These findings highlight the potential for this index’s use in clinical screening, notably in underserved communities, in which it could effectively assist clinicians in perioperative planning and managing postoperative outcomes in a more statistically-grounded way.