INTRODUCTION
Avascular necrosis of the femoral head (AVNFH) is a disease caused by a lack of blood supply to the femoral head, resulting in the necrosis of bone cells and bone marrow.1,2 AVNFH is prevalent among young and middle-aged people.2,3 The exact cause of the disease has yet to be determined, so treatment remains difficult. AVNFH progresses through several stages, and in the latter stages, joint arthroplasty is recommended.4–6
Despite many advancements in materials and surface coatings, the most recent generations of joints have an average lifespan of 15-25 years, so young patients who have undergone hip arthroplasty will face the issue of re-replacement.7 Re-replacement is more technically difficult, with a higher rate of accidents and complications, so short-stem hip joints have recently been used for primary arthroplasty to overcome the aforementioned difficulties.7–9
There are several classifications for short-stem hip joints. The American Society for Joint Research and Surgery categorizes short-stem hip joints into two groups: neck-fixed and metaphyseal-fixed.10 The femoral neck-fixed joints, such as the Cut, Silent, and Spiron joints,10 are the short-stem joints that preserve the most bone. The Spiron short-stem joint was created in 1989 in Germany.11 The joint sharf, shaped like a conical screw, features a sharp spiral thread and longitudinal grooves that increase the shaft’s contact area with the bone, resulting in a more stable and solid joint. When replacing the Spiron joint, only the femoral head is removed, leaving the neck and upper head of the femur intact, so that if the joint needs to be replaced again, it will be as convenient and easy as the first time.11
The purpose of using short-stem hip joints in general, and Spiron joints in particular, is to preserve bone.11 However, using this type of joint presents some challenges. That is, the narrow surgical field caused by femoral neck obstruction interferes with acetabulum reaming and placement. It is difficult to select and precisely position the joint shaft on the femoral neck in the desired position. As a result, it is necessary to study the hip joint anatomy of Vietnamese people in order to determine the joint size, position, and angle at which the Spiron joint shaft should be placed, restoring the anatomy and restoring the joint’s maximum function following arthroplasty.
Although the Spiron joint has been clinically used since 2001 worldwide and since 2011 in Vietnam, there have only been a few studies evaluating short-term outcomes with a small number of patients.12 Another issue that must be addressed today is that many surgeons in Vietnam do not plan before surgery and instead rely on a set of available measuring devices with a glass ball applied to the X-ray film to estimate joint size.13 This has many errors because the magnification ratio of the film does not match the magnification ratio of the measuring device, or because the measurement is done entirely by hand and with the naked eye, so the errors are even greater, negatively affecting arthroplasty outcomes. The use of digital X-rays instead of traditional X-rays, as well as the development of specialized software for joint replacement in medicine, have made measuring anatomical indicators and pre-operative planning on X-ray films more convenient and accurate. The objectives of this study are to describe several anatomical features of the hip joint in Vietnamese adults who were performed short-stem hip arthroplasty and to assess the outcomes of spiron short-stem hip arthroplasty in the treatment of avascular necrosis of the femoral head from 2012 to 2022.
PATIENTS AND METHODS
Patients
From January 2011 to December 2022, 46 patients were diagnosed with AVNFH, with 18 having both hips and 28 having only one. The patients underwent Spiron short-stem cementless total hip arthroplasty (18 for bilateral arthroplasty and 28 for unilateral arthroplasty) at the Institute of Trauma and Orthopedics, 108 Central Military Hospital. The selection criteria were: 1) Patients diagnosed with AVNFH stages IV, V, or VI according to Steinberg’s classification; 2) Age ≥18 - 50 years old; 3) Femoral neck bone shape and quality are still good. The femoral neck is not deformed, there was no lesion on the femoral neck MRI (no necrosis, the femoral neck has no necrosis calculated based on the intended position of the femoral neck in the preoperative plan); 4) The patient’s general and local condition does not preclude surgery or anesthesia; 5) The patient is pre-operatively planned on 2D software; 6) The patient has a Spiron short-stem hip arthroplasty. The exclusion criteria include: 1) The patient’s leg or foot cannot be straightened or rotated inward (not ensuring the correct position for the required scan); 2) The patient lacks complete medical records and X-ray films, fails to return for a follow-up appointment, or the follow-up period is less than 48 months.
Furthermore, between February 2012 and August 2016, 129 hips of healthy volunteers aged 18-50 were chosen to participate in a study to compare the anatomical indexes of the hip joint with those of patients with AVNFH. These people had straight hip X-rays. Inclusion criteria: Normal hip X-rays without any intervention in this area. Exclusion criteria include non-compliant X-rays, as well as deformed or pathological hip bones.
Study indicators
Acetabular indices
-
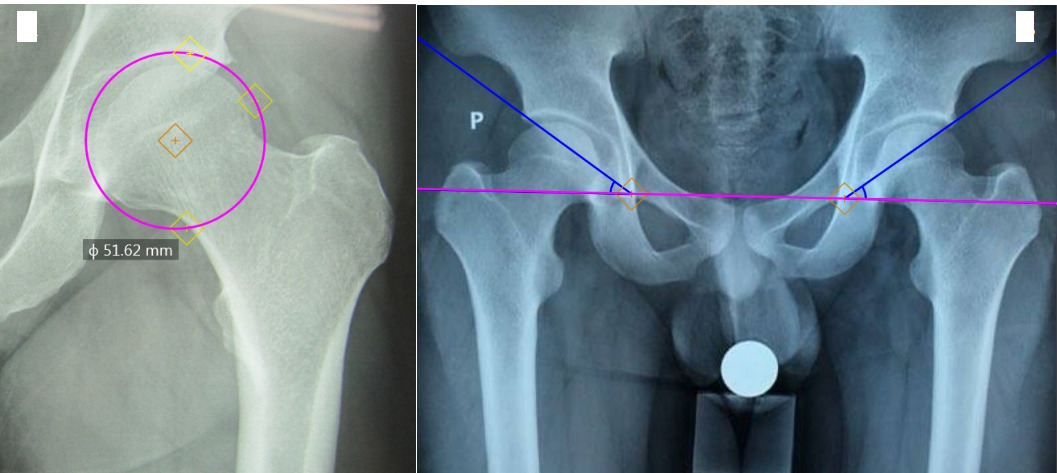
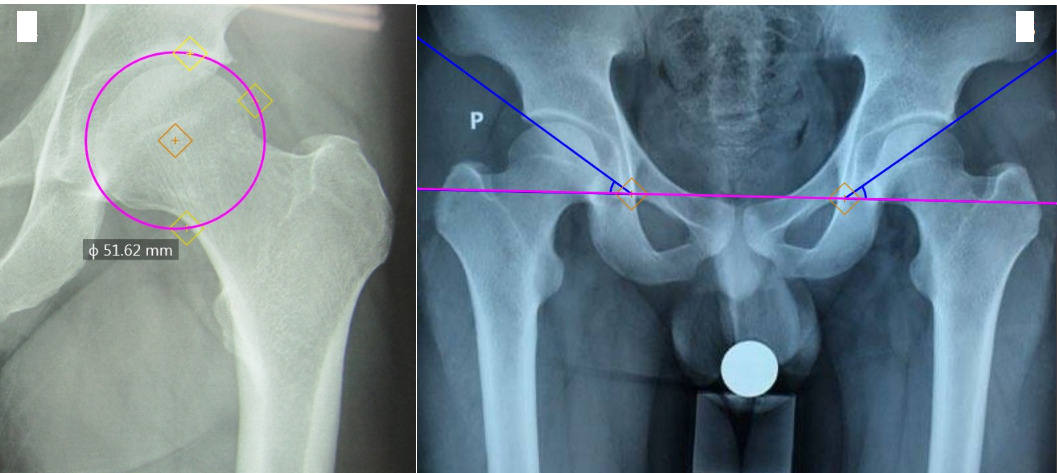
Acetabular diameter: is the diameter of the circle with an arc that fits into the acetabular socket (Figure 1A).
-
Acetabular tilt angle: is the angle formed by two straight lines, one passing through the lower medial bone edge (teardrop) of the acetabulum on both sides and one passing through the upper edge of the acetabulum and the lower medial bone edge (teardrop) of the acetabulum on the same side (Figure 1B).
Femoral neck indices
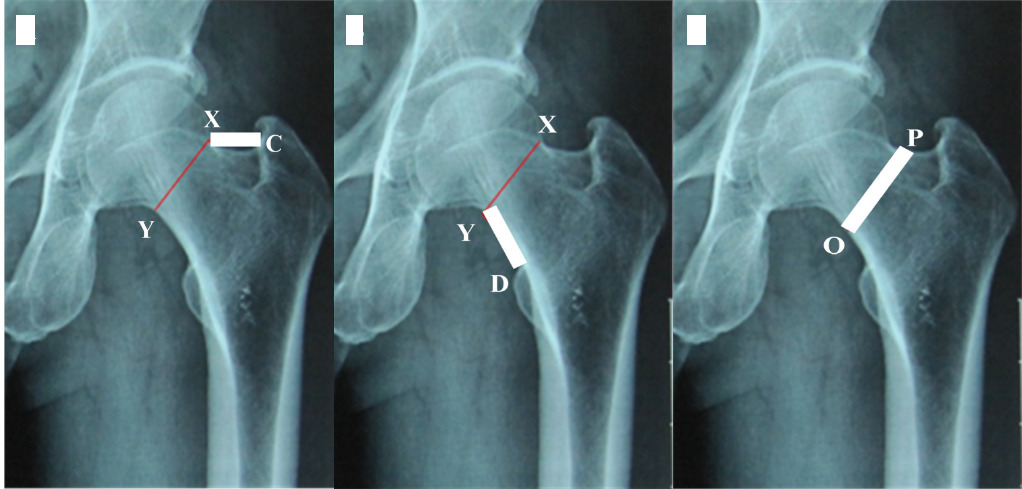
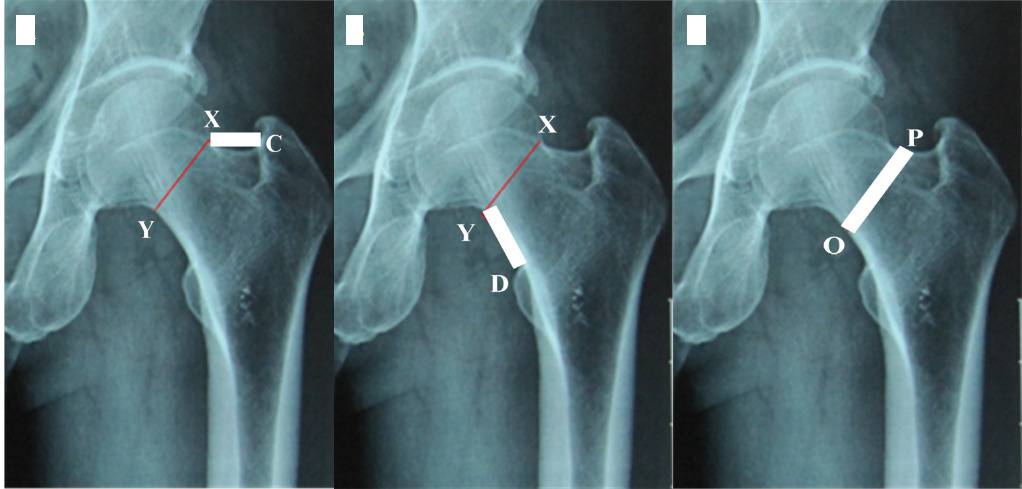
- The length of the upper border of the femoral neck The length of the upper border of the femoral neck is the distance between points X and C (Figure 2A).
- The length of the femoral neck’s lower border is the distance between points Y and D (Figure 2B).
- The distance above, below, and in the middle of the femoral neck is the distance between the two points O and P (Figure 2C).
Indicators related to the selection and placement of Spiron joint shafts
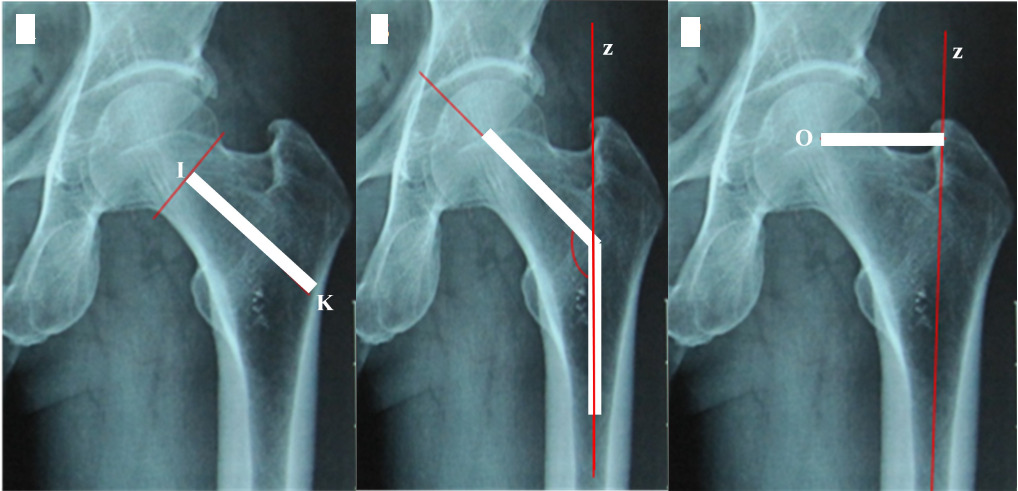
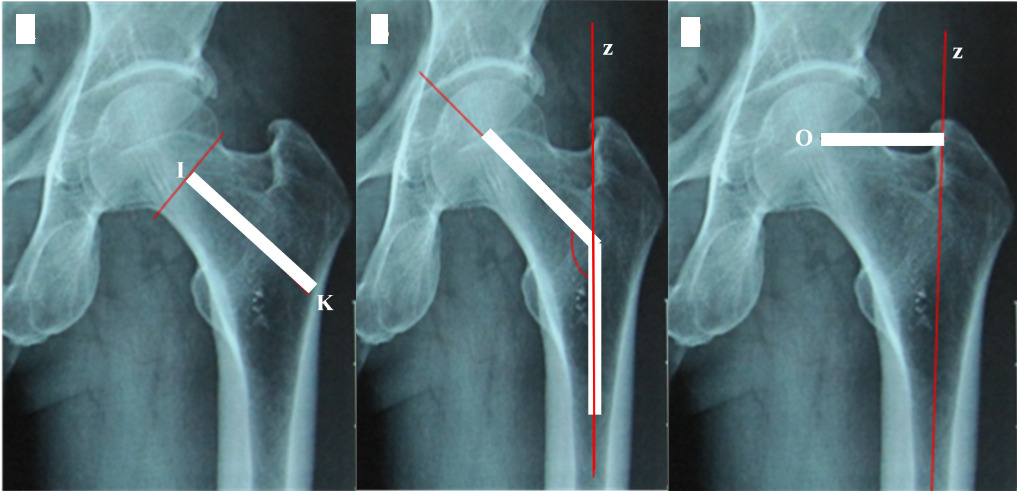
- Distance between the base of the head (close to the head) and the inner edge of the lateral femoral wall (along the mid-axis of the femoral neck): Is the distance between points I and K (Figure 3A). Point I represents the XY segment’s midpoint, while point K represents the intersection of the longitudinal axis between the femoral neck and the inner edge of the lateral femoral wall.
- The femoral neck angle is the angle formed by the axis of the neck (Line IK) and the anatomical axis of the femoral shaft (Line z) (Figure 3B).
- The offset is the distance from the center of the head to the anatomical axis of the femur. Is the distance between point O (the centre of the head) and line z (Figure 3C).
Spiron short-stem hip arthroplasty
- Preoperative computer planning: uses 2D software to plan surgery, including measuring acetabular diameter, temporarily determining femoral neck incision position, measuring distance from the base of the head to the hard bone shell, measuring distance above and below the center of the femoral neck, and measuring the angle of the femoral neck shaft.
- Preoperative patient preparation: includes all routine tests, an explanation of the patient’s condition, surgical plan, and expected outcomes.
Performing arthroplasty
The patients were anesthetized (spinal anesthesia), and the patient was lying on his side at 90o, with the operated limb above and the vertical margin of surgery behind the replaced joint.
-
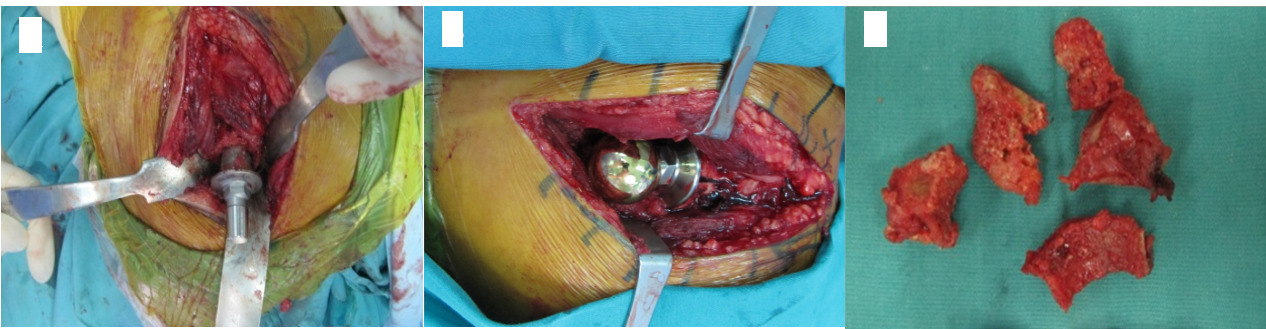
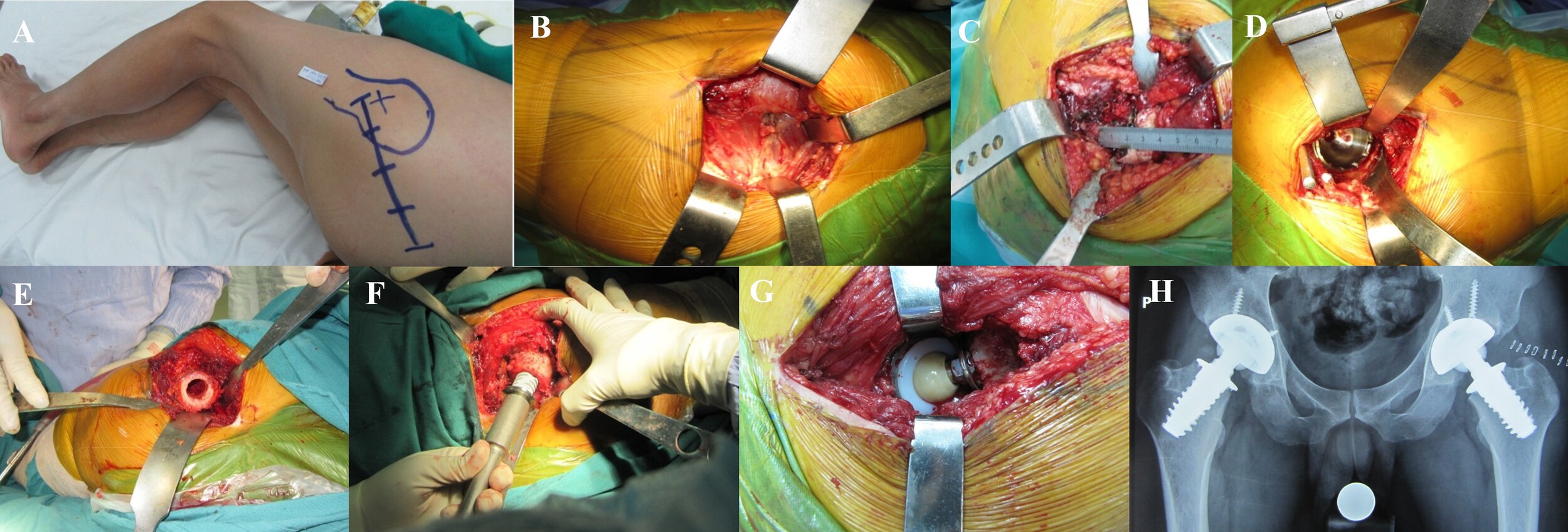
Step 1: Cut the skin to expose the hip joint, then cut the femoral head.
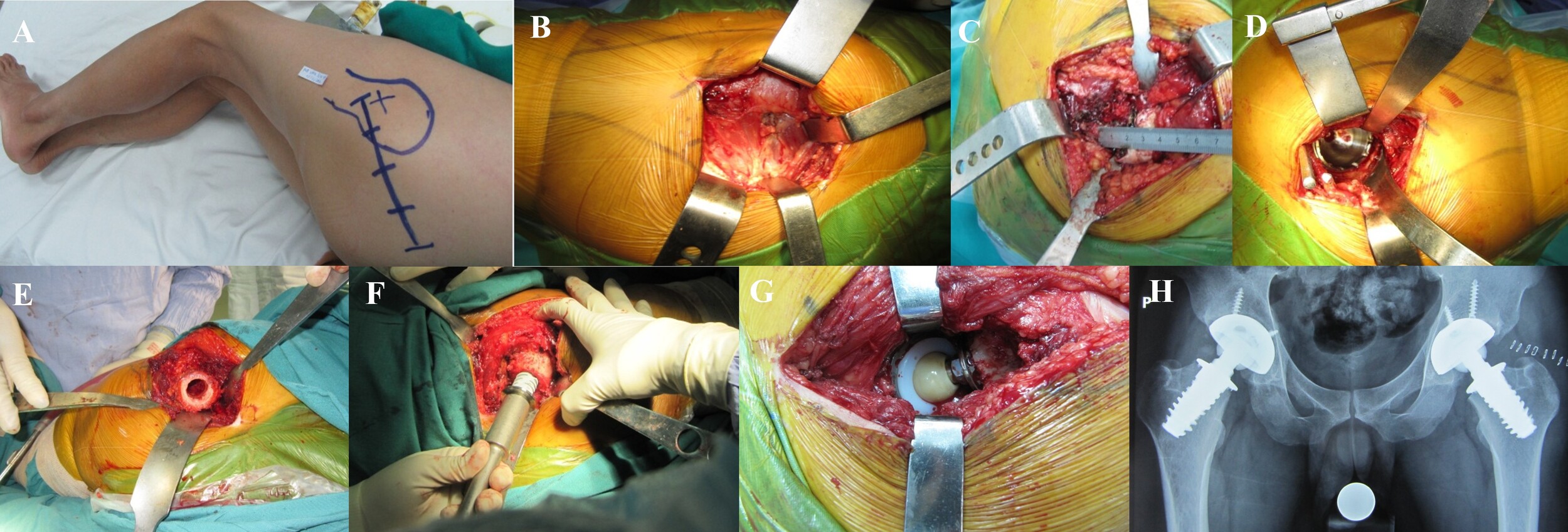
- Using the posterolateral (Figure 4A) and anterolateral incisions, the fascia was incised along the skin incision, the gluteus maximus muscle was separated, the gluteus medius muscle was left intact, and the leg was adducted and slightly internally rotated to expose the iliofemoral muscle group (Figure 4B).
- Cut a portion of the external rotator cuff and quadratus femoris muscle, the L-shaped joint capsule, expose the hip joint, rotate the leg inward to dislocate the hip posteriorly, and measure the upper and lower borders of the femoral neck (Figure 4C).
- Cut the femoral neck with a saw so that the cutting plane is perpendicular to the femoral neck axis, then use a knife to clean the surrounding bone spurs.
-
Step 2: Reaming and Installing the Acetabulum:
- Examine the acetabular cartilage, round ligament, and osteolysis (if present). Ream and place the artificial acetabulum as you would with a standard hip arthroplasty.
- Place the Hohmann bone elevator, then resect the cartilage, clean the bone spurs, and clean the remaining round ligament.
- Remove the base of the acetabulum with a small reamer, then gradually increase the diameter until all of the cartilage has been removed. Place the acetabulum in a trial position and compare to the preoperative plan.
- Place the acetabulum at a 45o angle to the horizontal plane and tilt 15o forward. A surface roughener has been used to fix the acetabulum. If the bone quality is poor, 2-3 more fixing screws may be added (Figure 4D).
-
Step 3: Prepare the femoral neck:
- Determine the center of the femoral neck, insert the blunt-headed Kirschner nail along the femoral neck’s axis near the hard bone wall, and measure the length of the articular shaft to be replaced.
- Determine the diameter of the articular shaft by using specialized coins with different diameters of 18, 20, 22, 24 mm to measure the diameter of the femoral neck.
- Ream bone marrow, install a trial shank and cap, reset the hip joint, and measure leg length.
-
Step 4: Insert the handle, replace the head, realign the joint, and close the incision:
- Place the Spiron joint handle: Using the measured length and diameter, turn the handle clockwise by hand until the small tabs on the handle plate are firmly embedded in the hard bone shell (Figure 4F).
- Select the crown: S (Small) is -5, M (Medium) is +0, and L (Large) is +5. Try the crown, inspect the movement, perform the piston test, measure the length of both legs, install the crown, and realign the joint (Figure 4G).
- Irrigate, stop bleeding, do not insert a drain (only if absolutely necessary), and suture the incision.
Post-operative monitoring and exercise
- Take bilateral hip X-rays (Figure 4H), and remove drains 24 hours after surgery (if applicable).
- Monitor and evaluate post-operative progress.
- Exercise as prescribed by Birkenhauer B. following short-stem Spiron hip arthroplasty. The patient begins passive and active exercise on the second day after surgery to regain joint range of motion, which includes flexion, extension, abduction, and hip joint. Exercise gradually increases muscle strength in key muscles such as the iliopsoas muscle, gluteal muscle, and quadriceps.
- Remove the stitches 12-14 days after surgery.
- Patients use two crutches for 6-8 weeks after surgery to reduce the impact force on the joint shaft because there is no biological connection between the bone, joint shaft, and acetabulum.
Postoperative outcome assessment and data collection
- Post-operative check-up intervals include: immediately after surgery, 8-12 weeks after surgery, 12 months, 36 months, and 48 months.
- Evaluate hip joint function using the Harris score at three time points: before surgery, 12 months, 36 months, and 48 months after surgery.
- Assessment contents include surgical wound progress, complications, X-ray changes, acetabular position, joint rotation, Harris-scale artificial hip function, pain level, walking ability, and range of motion.
- Patient, clinical, and paraclinical data are obtained from the patient’s medical records.
Data analysis
Data were entered into Epidata 3.0 software and analyzed using medical statistical algorithms in SPSS 22.0 software to calculate experimental parameters such as mean, standard deviation, and correlation between two quantitative variables. Qualitative variables were presented as percentages. For qualitative variables, use the Chi-square test (χ²) (adjusted with Fisher’s exact test, Phi, and Cramer’s V as needed). For quantitative variables with normal (or relatively normal) distributions, use the t-test, paired test, or ANOVA test.
RESULTS
Of the 46 patients who had Spiron short-stem hip arthroplasty, 44 (95.6%) were men and only 4.4% were women. Patients aged 41-50 years accounted for 59.7%, followed by those aged 31-40 years (37.5%) and 25-30 years (2.8%), with a mean age of 40.6 years. Out of the 46 patients, 18 underwent bilateral hip arthroplasty (39.1%), 13 underwent right hip arthroplasty (28.3%), and 15 underwent left hip arthroplasty. Of the 64 hips that were operated on, 46.9% had stage IV AVNFH, 45.3% stage V, and 7.8% stage VI. In terms of pain severity, 57.8% of the joints were in severe pain, 39.1% in moderate pain, and 3.1% in mild pain. In terms of mobility, 59.4% of the joints had severe limitations, while 40.6% had moderate limitations. The Harris score of 64 hips revealed that 30 hips (46.9%) were in stage IV, with a mean Harris score of 48.3, 29 hips (45.3%) were in stage V, with a mean Harris score of 44.2, and 5 hips (7.8%) were in stage VI, with a mean Harris score of 41. The average Harris score across all AVNFH stages was 45.9 points (Table 1).
The anatomical indexes of the hip joint of AVNFH patients and healthy people (Table 2)
- Acetabular diameter: Patients with AVNFH had an average acetabular diameter of 48.2 mm, compared to 49.4 mm for healthy people. AVNFH patients had a higher rate of acetabular attachment diameters between 48 and <50 mm compared to healthy people (40.6% vs 34.1%).
- Acetabular tilt angle: patients with AVNFH had an average of 44.1o, while the healthy people had 41.8o. At tilt angles > than 40 – 45o, AVNFH patients had a higher rate than the healthy group (64.1% vs. 59.7%).
- Upper femoral neck length: the average length of AVNFH patients was 15.3 mm, while the healthy people measured 17.6 mm. AVNFH patients had a higher rate for lengths between 8.3 and 15 mm, but lower rates for lengths between 19 and 26.8 mm compared to healthy people (32.8% vs 24.0%; 18.8% vs 27.9%).
- Lower femoral neck length: The average length of AVNFH patients was 21.6 mm, while healthy people had 23.3 mm. AVNFH patients had higher levels from 14.3 to <20 mm (31.2% vs 24.8%), but lower levels from >25 to 34.2 mm (20.4% vs 27.9%).
- Distance above and below the center of the femoral neck: The average distance between AVNFH and healthy people was 32.9 mm and 34.5 mm, respectively. There was little difference in the distance levels between AVNFH patients and healthy people.
Indicators for selecting and placing Spiron articulating shafts (Table 3)
- The average distance between the base of the head and the medial edge of the lateral femoral wall was 50.1 mm in AVNFH patients and 51.2 mm in healthy people.
- Femoral neck-shaft angle: The average femoral neck-shaft angle in AVNFH patients was 131.6o, while healthy people had 132.1o.
- The distance between the center of the femoral head and the shaft: The average distance between AVNFH and healthy patients was 36.4 mm and 37.9 mm, respectively.
The Spiron joint indexes used during surgery for patients included (Table 3)
- The 50 mm acetabulum was the most commonly used (51.6% of patients), followed by the 48 mm acetabulum (32.8%), the 46 mm acetabulum, and the 52 mm acetabulum (7.8%).
- Number of screws used to fix the Spiron joint: 57.8% of patients did not require screws for fixation, 40.7% used two screws, and 1.5% used three screws.
- The joint head with diameter -5 (S-small) was used by 76.6% of patients, followed by type 0 (M-medium) (18.7%) and type 5 (L-large) (4.7%).
- 59.4% of patients used a 20-mm diameter articulating shaft, followed by 22-mm (31.5%) and 18-mm (9.1%).
- 54.7% of patients used 50 mm joint shafts, followed by 45 (31.3%), 55 (12.5%), and 60 mm (1.5%).
Clinical and X-ray indicators of patients underwent Spiron short-stem hip arthroplasty at four time points: prior to surgery, 12 months, 36 months, and 48 months after surgery (Table 4).
Clinical features
- Pain level: Prior to surgery, 25.0% and 71.9% of patients experienced moderate to severe pain, respectively; after 12 and 36 months, these rates decreased to 1.6% and 0.0%. However, after 48 months of surgery, it increased to 4.7% and 3.1%, respectively.
- Walking ability: Before surgery, 40.6% and 59.4% of patients had mild and severe limitations, respectively; 12 months after surgery, this rate was 23.4% and 3.1%, followed by 36 months (34.4% and 1.6%) and 48 months (37.5% and 4.7%).
- Total range of motion: before surgery, mild and severe limited motion were 43.8% and 56.2%, respectively; 12 months after surgery, this rate dropped to 25.0% and 0.0%, 36 months (26.6% and 1.6%), and 48 months (39.1% and 4.7%).
- Hariss score: prior to surgery, the average Hariss score was 46.8, 12 months after surgery was 92.2, 36 months (91.6), and 48 months (81.2). The Harris score for stage IV was higher than for stages V and VI.
X-ray features
- There was no difference in acetabular tilt angle between preoperative (40.2o) and postoperative (12, 36, 48 months) (39.9-40.1o). However, the distance from the center of the head to the anatomical axis of the femur (35.2 mm) and limb deviation (9.2 mm) before surgery differed from those after surgery (37.2 - 39.6 mm and 3.1 - 3.6 mm).
- The occurrence of bone support pillar and bone platform support after surgery at 12 months was 4.6% and 15.6%, respectively, at 36 months (7.8% and 48.4%) and 48 months (15.6% and 65.6%). The indexes for bone joint connection area, cortical bone hypertrophy, and heterotopic ossification increased from 1.5% after 12 months to 3.3-4.4% after 36 months and 6.3-9.4% after 48 months.
- Preoperative Harris scores were good and excellent in 0.0% of patients, but increased to 20.3% and 78.1% after 12 months of surgery, 17.8% and 76.1% after 36 months, and 14.1% and 64.1% after 48 months, respectively.
Complications following Spiron short-stem hip arthroplasty (Table 5)
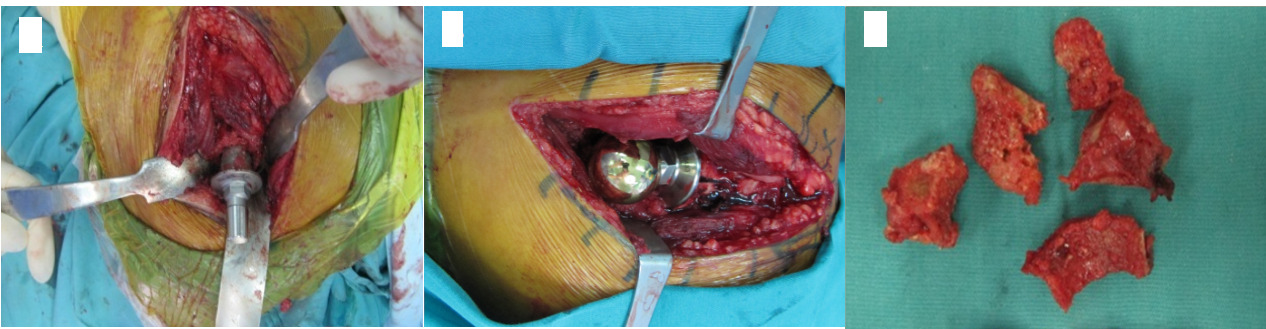
- There was one femoral neck fracture (1.6%) during Spiron hip arthroplasty (Figure 5).
- Acetabular displacement occurred in one joint (1.6%) 36 months after surgery, and in two joints (3.1%) 48 months later.
- The proportion of joints with surgical site infections 12 months after surgery was 1.6%.
- The proportion of joints with lateral popliteal nerve injury was 6.3% after 12 months of surgery, 3.1% after 36 months, and 1.6% after 48 months.
- The number of joints with partial osteolysis around the joint handle was 3.1% after 12 months of surgery, 7.8% after 36 months, and 18.8% after 48 months.
- The number of joints with a clear border around the joint was 3.1% after 12 months of surgery, 15.6% after 36 months, and 21.9% after 48 months.
- The number of joints that needed to be replaced was 1.6% after 12 months of surgery, 1.6% after 36 months, and 12.5% after 48 months.
DISCUSSION
In our study, patients ranged in age from 25 to 50 years old, with an average of 40.6 years. The question is whether joint arthroplasty is truly necessary for younger patients. The majority of the patients in the study had been treated with internal medicine for an extended period of time, resulting in muscle atrophy and deformed femoral heads. In many cases, the acetabulum degenerated, the joint space narrowed, and the constant pain caused physical and mental damage. Therefore, it is reasonable to prescribe hip replacement for these patients. Spiron short-stem hip arthroplasty is recommended for patients aged 18 to 50 years old because the lifespan of a standard hip joint is only 15 to 25 years, which increases the risk of having to replace the hip again. As a result, prescribing Spiron hip arthroplasty for these patients is more appropriate and advantageous for their next joint arthroplasty. The average age of patients with spiron hip arthroplasty by Birkenhauer11 (average age 60.1), Lugeder14 (average age 51), Ender15 (average age 50). Thus, the average patient age in this study is significantly lower. Because these countries’ life expectancy is higher than that of Vietnamese people, owing in part to better nutritional conditions, the bone quality of people of the same age in developed countries is frequently higher.
The femoral neck angle of Vietnamese adults is frequently measured on dry femurs, with little variation. According to studies on Vietnamese people, the femoral neck angle ranged from 129° to 132° in men and 128.32° to 128.41° in women.16,17 Our findings are quite similar to those of other studies conducted in Vietnam.16,17 However, the average femoral neck angle in Indians is 126.55°,18 while in Europeans it is 136° for men and 133° for women.19 Vietnamese people have a higher femoral neck angle than Indians, but lower than Europeans. Jerosch et al.20 indicated that the average change in the femoral neck angle after surgery was (-0.5o) (SD: 4.1o), with the largest increase at 11o and the largest decrease of 16o. The patient’s femoral neck angle was restored after surgery, as opposed to before. In a study of Nanos short-stem joint replacement patients, Ettinger et al.21 found that the average femoral neck angle after surgery was 134.6° (± 4.3°), higher than the pre-surgery angle of 133.8° (± 4.8). Thus, the change in the femoral neck angle before and after surgery of the patients in this study is consistent with previous studies.
Birkennheur et al.11 advised against using Spiron short-stem hip arthroplasty in patients with a femoral neck angle of less than 122o. However, in this study, no case of a preoperative femoral neck angle less than 122o was found. Birkennheur et al.11 found that if the femoral neck angle is too low, the shaft is likely to be displaced and penetrate the hard bone wall. In this study, four patients had a femoral neck angle ranging from 120o-125o; clearly, these cases should be considered and addressed when replacing the Spiron joint. The data showed that the patients’ post-operative femoral neck angles increased by an average of 3.2o when compared to before surgery. Another study in Vietnam12 found that the average post-operative femoral shaft angle and anatomical axis was 143.85° ± 8.02° (95% of values were between 141.78° - 145.92°), which was higher than the pre-operative 134.43° (95% of values were between 133.1° - 135.7°). Setting the femoral neck angle higher postoperatively than preoperatively is preferable to setting it lower. However, these studies have not determined how many degrees higher the allowable limit is.11,18,19,21
Restoring the distance from the center of the head to the anatomical axis of the femur, as well as limb length, is an important goal of hip arthroplasty and hip function restoration.22,23 Our data show that the average distance from the center of the head to the anatomical axis of the femur is 38.3 mm, distributed unevenly in the range of 27.1 - 51.2 mm, which is consistent with the Roy24 and Siwach25 studies. Since the early days of hip arthroplasty, there has been much debate in the medical literature about whether to raise or lower this index.26 Jerosch et al.20 reported that the distance from the center of the head to the anatomical axis of the femur increased by 0.28 cm (SD 0.45 cm), and hip function was fully restored. Amenabar27 also found that after surgery, the distance between the center of the head and the anatomical axis of the femur increased by 0.6 mm compared to the opposite side. In terms of biomechanics, increasing the distance from the center of the head to the anatomical axis of the femur expands the lever arm, reducing the load on the joint, lowering the risk of collision, and expanding the artificial joint’s free range of motion.26,28 The disadvantage is an increase in load at the distal end of the articular shaft.26 In this study, the distance from the center of the head to the anatomical axis of the femur after surgery was larger than before surgery and comparable to that of healthy people. The distance between the center of the head and the anatomical axis of the femur after surgery and at the last check was equal. Jerosch et al.20 reported that when replacing a short-shaft hip, the ideal is to restore this index to its original value, but the general trend is for the distance from the center of the head to the anatomical axis of the femur to increase following surgery.
Limb discrepancy is a common problem following hip arthroplasty, and it can be caused by a variety of factors.29,30 First and foremost, the surgeon fails to consider the length of the limb during the surgery when installing the prosthetic shaft and head. Patients who do not have surgery for a long time may have atrophied muscles on the side of the hip joint with AVNFH, causing the joint to be loose when the hip joint is replaced and the two legs are equal, and when the head index is increased to make the joint stable, the two limbs become uneven. Many studies, particularly for patients with bilateral AVNFH, prioritize making the joint stable in the first surgery, with the next surgery adjusting to restore limb balance for the patient. Therefore, when examining patients between two surgeries, the rate of limb discrepancy is higher.20,21,27 Previous studies reported that a difference of 10mm or more between the two limbs following hip arthroplasty affects gait, pain, and rapid acetabulum wear, so patients must wear orthopedic shoes.31,32 Furthermore, studies have found a correlation between the condition of limb lengthening after surgery and sciatic nerve damage, lateral popliteal nerve palsy, and sciatic nerve palsy when the difference between the two limbs is large.31,32 The primary cause of limb imbalance is incorrect placement of the joint shaft, and the reduction in the distance from the center of the head to the anatomical axis of the femur (offset) is due to incorrect placement of both the joint shaft and the acetabulum.33–35 Therefore, in hip arthroplasty, special attention should be paid to balancing the limb and restoring the distance from the center of the head to the anatomical axis of the femur, avoiding a limb deviation of more than 10mm and reducing this distance by more than 5mm compared to the healthy side.22
Our findings indicate that the rate of complications in patients undergoing short-stem hip arthroplasty is quite high compared to previous studies.36 Spiron short-stem hip arthroplasty has some complications similar to standard hip replacement. However, the most concerning aspect of short-stem hip arthroplasty is the rate of re-replacement and displacement of the joint shaft.36,37 Complications that can occur after surgery, such as fractures around the short shaft, fractures of the joint shaft, deep infection, bone loss…, can necessitate hip replacement; previous studies have also documented the occurrence of these complications after surgery.5,38,39 In this study, there was one femoral neck fracture and one acetabular fracture. We had to fix three acetabular screws and allow the patient to compress late; after examination, the bone healed well and the acetabular was not displaced. There was one case of superficial wound infection after 12 months. In addition, lateral popliteal nerve injuries, partial osteolysis around the joint shaft, and periarticular lucency occur more frequently over time. As a result, 48 months after surgery, 8 cases of hip replacement were reported due to these complications. Because the short-stem hip joint has a relatively short history of development, surgeons are often concerned about the rate of replacement. Oldenrijk40 and Steens15 found that 2.5% and 11.0% of joints required replacement after more than three years of follow-up, respectively. The rate of joint replacement among the patients in this study is quite high. The Spiron hip arthroplasty technique is more difficult than standard hip arthroplasty; additionally, Spiron hip arthroplasty was first performed in Vietnam, so the initial surgeons were not yet adapted, so Spiron hip arthroplasty was incomplete, the rate of complications and re-joint replacement was still high. Later, as surgeons improved their techniques, the rate of complications and re-joint replacements decreased significantly. To improve the efficiency of hip arthroplasty, surgeons must be trained and supervised technically.
CONCLUSION
Spiron short-stem hip arthroplasty for young Vietnamese patients revealed many outstanding benefits because the upper head and metaphysis structure remain intact, making standard hip replacement later quite simple. Furthermore, it demonstrates that if the surgeon’s surgical indication selection and technique, as well as the measurement of hip joint anatomical indicators and computer planning, are not perfected and strictly adhered to the pre-operative plan, the risk of complications and re-joint replacement is extremely high.
ACKNOWLEDGMENTS
We thank the Spiron-stem hip arthroplasty patients who agreed to participate in this study. We would also like to thank the 108 Military Central Hospital for their assistance in performing this study.
AUTHOR CONTRIBUTIONS
Mai Duc Thuan: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Resources, Data curation, Writing – original draft, Visualization, Writing – review & editing, Visualization, Supervision. Nguyen Quoc Dung: Conceptualization, Methodology, Validation, Resources, Data curation, Writing – review & editing.
ETHICAL STATEMENT
This study was approved by the ethics committee of the 108 Military Central Hospital. This study was conducted in accordance with the Declaration of Helsinki and the guidelines and regulations of the Vietnamese Ministry of Health. All the patients consented to participate in this study, and informed consents were signed by themselves in all instances.
PATIENT’S CONSENT
The patients were informed that data from the research would be submitted for publication, and gave their consent.
FINANCIAL DISCLOSURE
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
CONFLICT OF INTEREST
The authors declare no competing interests.