Introduction
Obligatory dislocation of the patella (ODP) is a condition when the patella dislocates during knee flexion and relocates spontaneously upon extension.1 ODP typically presents during the first decade of life. Although children may compensate initially, instability often worsens with age.2 ODP is uncommon in adults, where patellar instability is further aggravated by factors such as an abnormal Q-angle, genu valgum, patella alta, trochlear dysplasia, and medial patellofemoral ligament (MPFL) insufficiency.1 The hallmark clinical sign is the inability to flex the knee beyond 30°–70° (early to mid-flexion) while maintaining the patella in the midline.3 Recurrent maltracking may lead to patellofemoral pain and degenerative arthritis.4
While bracing, physiotherapy, and other conservative measures may relieve symptoms, they are insufficient to correct patellar instability. Delayed surgical intervention increases the risk of painful arthrosis and the need for trochlear reconstruction following early stabilization.2 Given the varied etiologies and complex anatomic abnormalities, ODP presents a challenging clinical and surgical problem. No single technique has proven universally effective. A combined approach using proximal procedures (lateral retinacular release, MPFL reconstruction, trochleoplasty, quadricepsplasty) and distal realignment (tibial tubercle transfer or patellar tendon medialization) has been suggested for managing adult ODP.5
Given the limited literature on adult ODP and the absence of an established optimal approach, we present a case managed with combination of techniques (lateral release, quadriceps lengthening, semitendinosus tenodesis, and anteromedial tibial tubercle transfer) resulted in favorable functional outcomes.
Case Presentation
Patient Information
A-31-year-old male presented with a lifelong-history of lateral patellar dislocation. He reported no childbirth complications, no family history of similar conditions, and no history of trauma. Since childhood, the patella had remained laterally displaced and irreducible, causing a painless but noticeable deformity and mild ambulatory difficulty that progressively affected daily activities. On evaluation, the patella could not be repositioned, and the knee appeared laterally deviated and asymmetric, although the patient continued to report no pain.
The patient had no reported medical comorbidities, including diabetes mellitus, hypertension, cardiovascular disease, pulmonary disorders, or neuromuscular conditions. He was not on any regular medications and had no documented drug contraindications. Body mass index was within normal parameters (BMI 24.2), cardiovascular and respiratory assessments showed no abnormalities. The patient had experienced gait impairment with increasingly impacted daily activities and occupational functions. Despite the apparent deformity, the patient reported minimal discomfort but experienced mechanical difficulties.
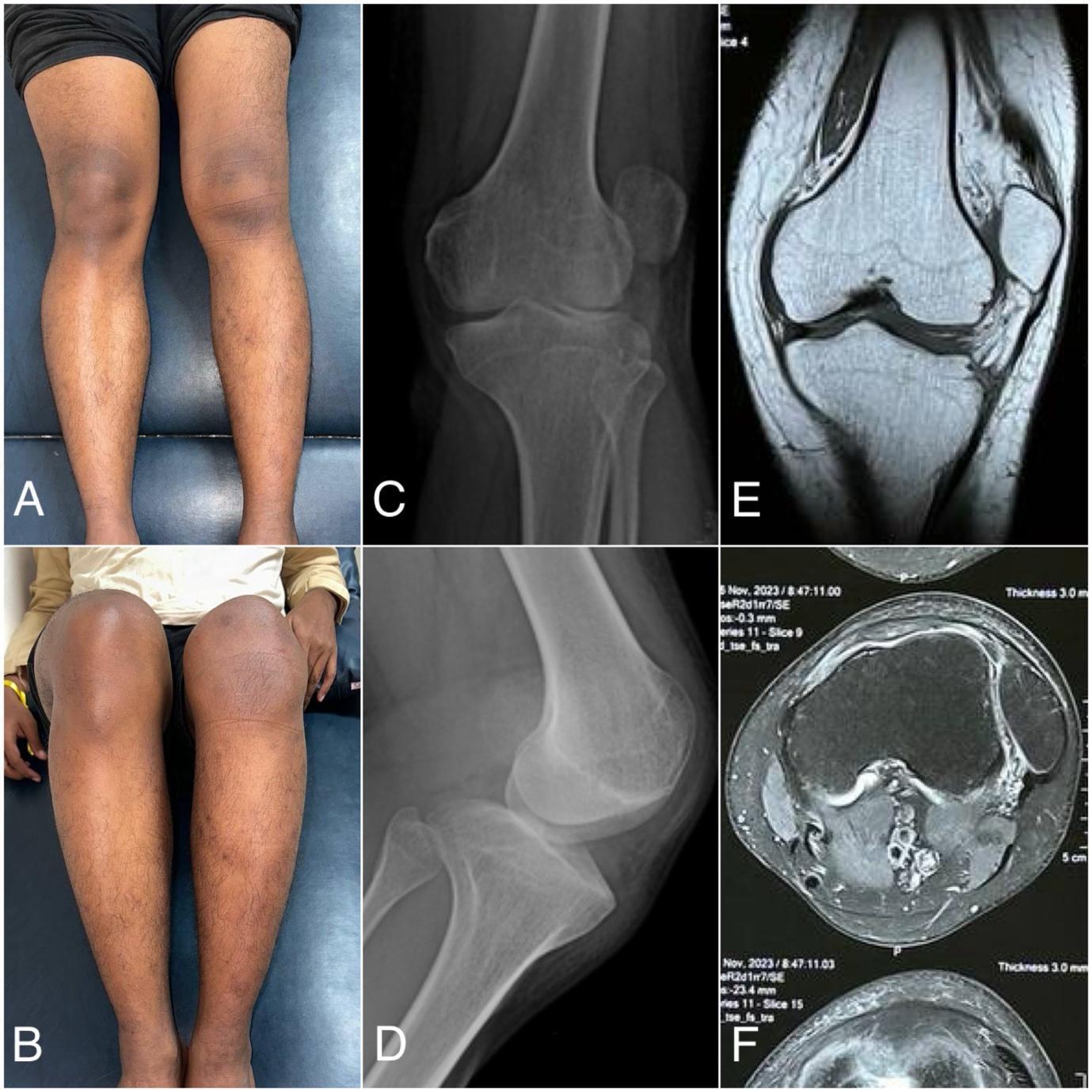
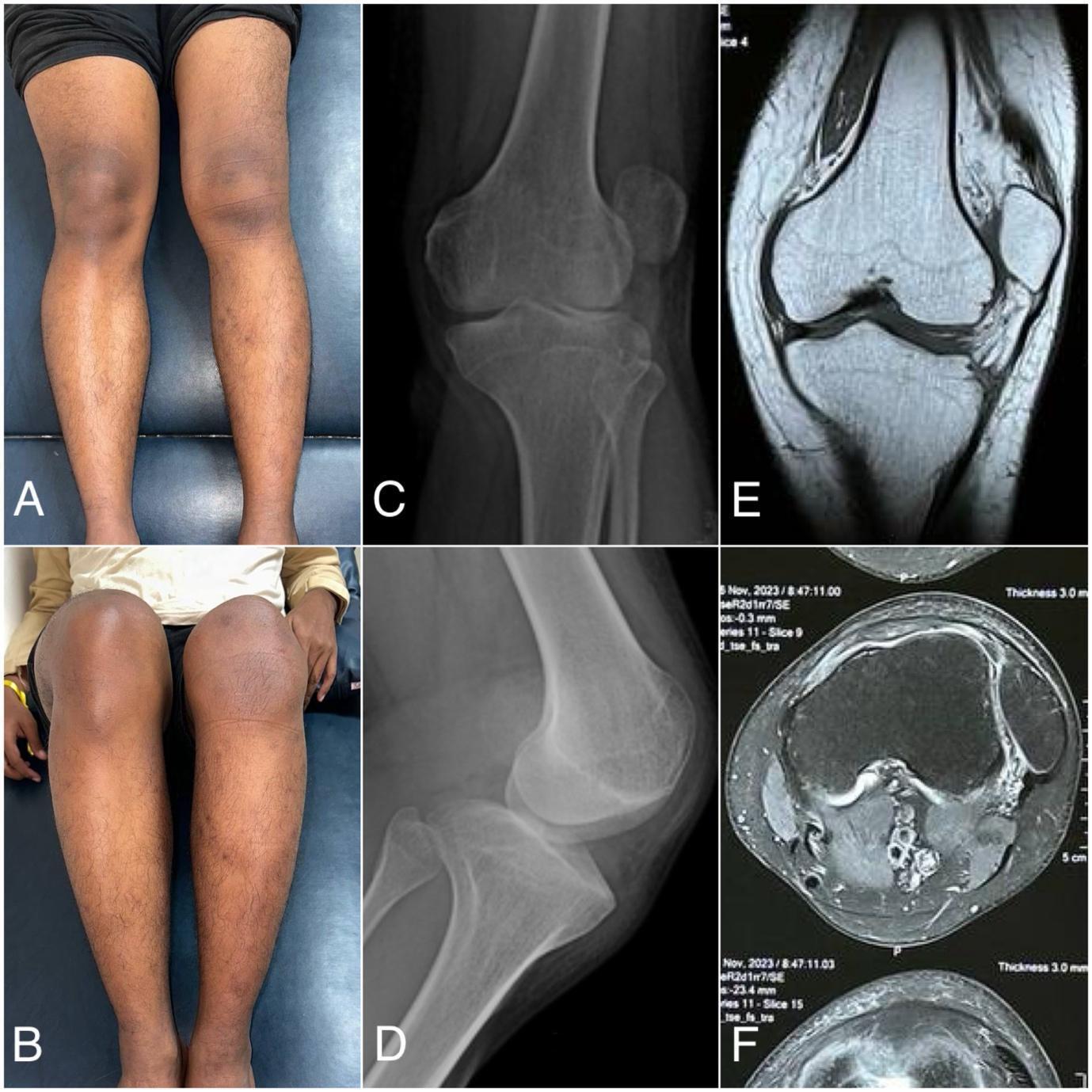
The physical examination showed a deformity of the left knee, and a J-track sign was visualized on his lateral side of the left knee (Fig 1A, 1B). The apprehension test showed a positive sign of lateral dislocation of the patella but without pain. The passive lateral patellar tilt test yielded a negative result due to the widespread stiffness and tightness of the soft tissue connection along the lateral border of the patella. There was no swelling, but the patella was clearly palpable on the lateral knee. Only 75 degrees of knee flexion range of motion and 20 degrees of knee extension range of motion from the horizontal axis. Clinical scoring using the Tegner Lysholm score of 69 and the IKDC score of 62.1, which indicating moderate functional limitation. Anteroposterior and lateral knee radiographs, as well as coronal and axial MRI scans, revealed a patellar lateral dislocation associated with trochlear dysplasia (Fig 1).
Preoperatively, the patient laboratory result showed within normal limit. Hemoglobin 4.82 10^6/µL, Erythrocytes 4.82 10^6/µL, Leucocytes 8.9 10^3/µL, Thrombocytes 334 10^3/µL, Albumin 4.57 g/dL, Blood Urea Nitrogen 8 mg/dL, Creatinine 0.95 mg/dL, Natrium (Na) 140 mmol/L, Kalium (K) 4.2 mmol/L, Klorida (Cl) 103 mmol/L. The patient was in excellent overall condition and classified as American Society of Anesthesiologists (ASA) Physical Status Class I.
Operative procedure
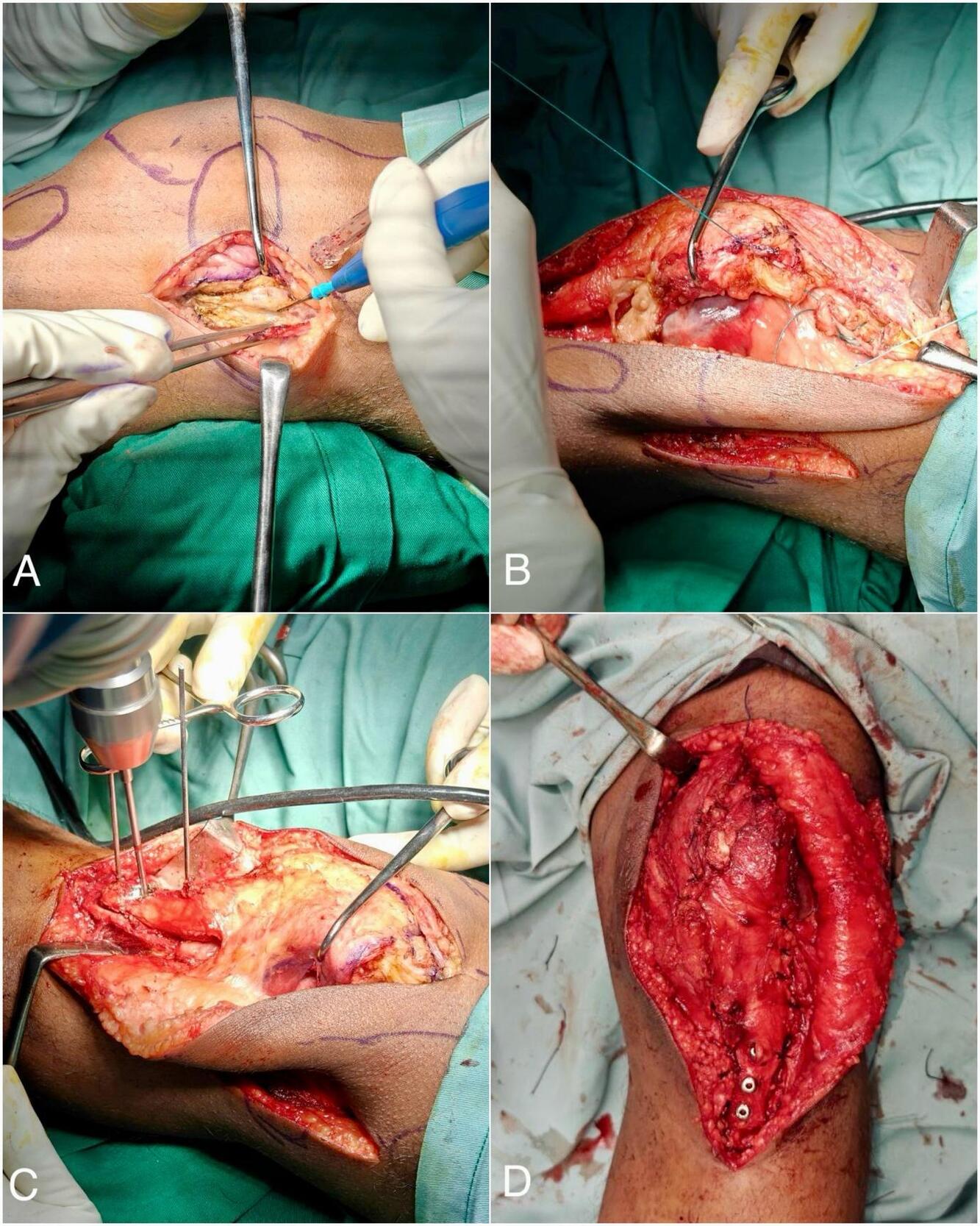
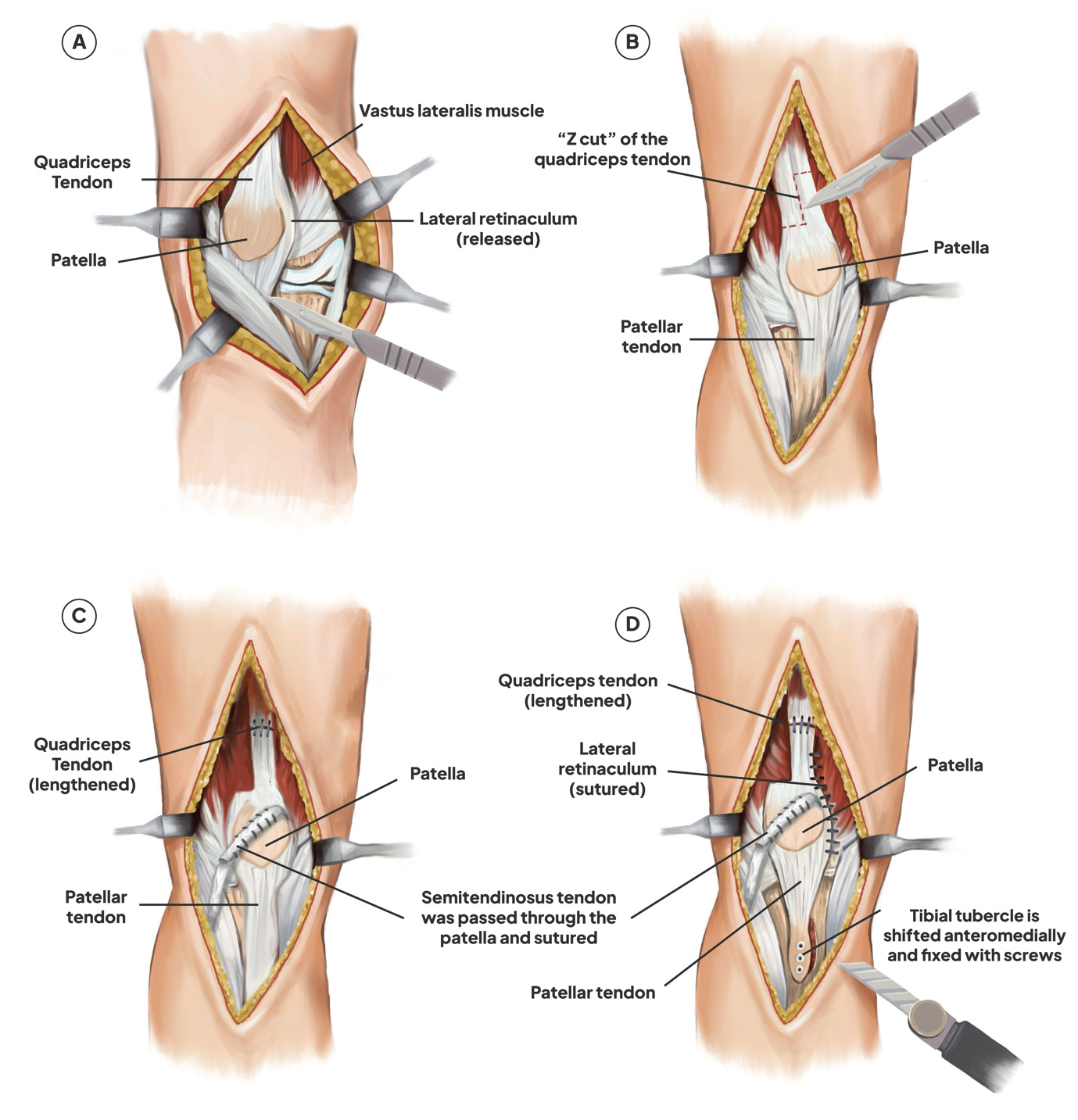
A midline incision was performed to uncover the quadriceps muscle and tibial tubercle, that extend from 5 cm above and 10 cm below the patella. The proximal realignment procedure was initiated (Fig 3A).
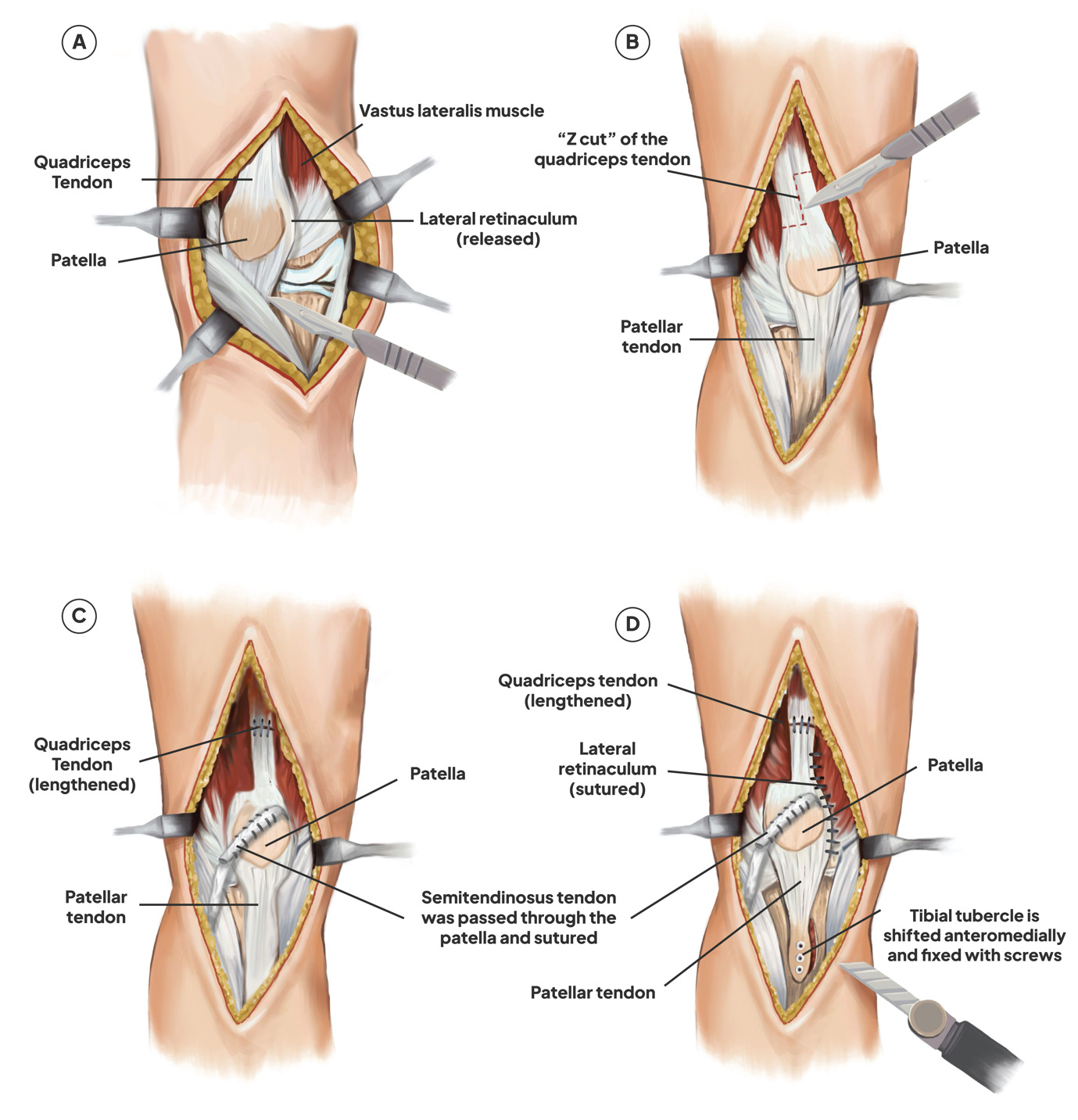
Lateral release along the patellar tendon was performed proximal to the vastus lateralis tendon (Fig 2A). Sections of the vastus lateralis were made near the patella (Fig 3A). The results of the thumb test demonstrated that the patella re-dislocates during full range flexion. Vastus lateralis tendon was released by sectioning it close to the patella. However, the thumb test remained positive, indicating that quadriceps lengthening was necessary.
__quadriceps_.jpg)
A “Z” cut was made to the quadriceps tendon (Fig 2B). The medial quadriceps tendon remained attached to the superomedial patella, whereas the distal portion of the Z was situated at the superolateral face of the patella, extending half the transverse breadth of the quadriceps tendon. The proximal aspect of the Z was medial, while the longitudinal aspect was located in the middle of the tendon. Usually, the tendon was extended by around 2 cm. The distal segment of the vastus lateralis is reattached to the lateral side of the major quadriceps tendon, proximal to the patella, following the repair of the quadriceps tendon with multiple interrupted nonabsorbable sutures, augmented by several interrupted absorbable sutures (Fig 3B).
The semitendinosus autograft was selected for MPFL reconstruction. After harvesting the semitendinosus tendon, an oblique patellar tunnel was formed, extending from the inferomedial to the superolateral aspect of the patella. Once the graft was in the tunnel, it was sutured to the patella’s periosteum and, if there is enough length, to itself (Fig 3C).
The anteromedial tibial tubercle transfer technique was used to start the distal patellar realignment. The osteotomy site was well defined. Next, three K-wires were positioned obliquely (at a 45° angle) parallel to the proximal part of the tibia. The osteotomy was then carefully finished with a half-inch osteotome. Approximately 10 mm of medialization could be measured with a ruler. Proper tracking position was verified and the degree of antero-medialization was attained and maintained by temporary K-wires (Fig 3C). Then, for improved fixation, three screws were inserted into the tibial tubercle and verified by the C-arm (Fig 2D).
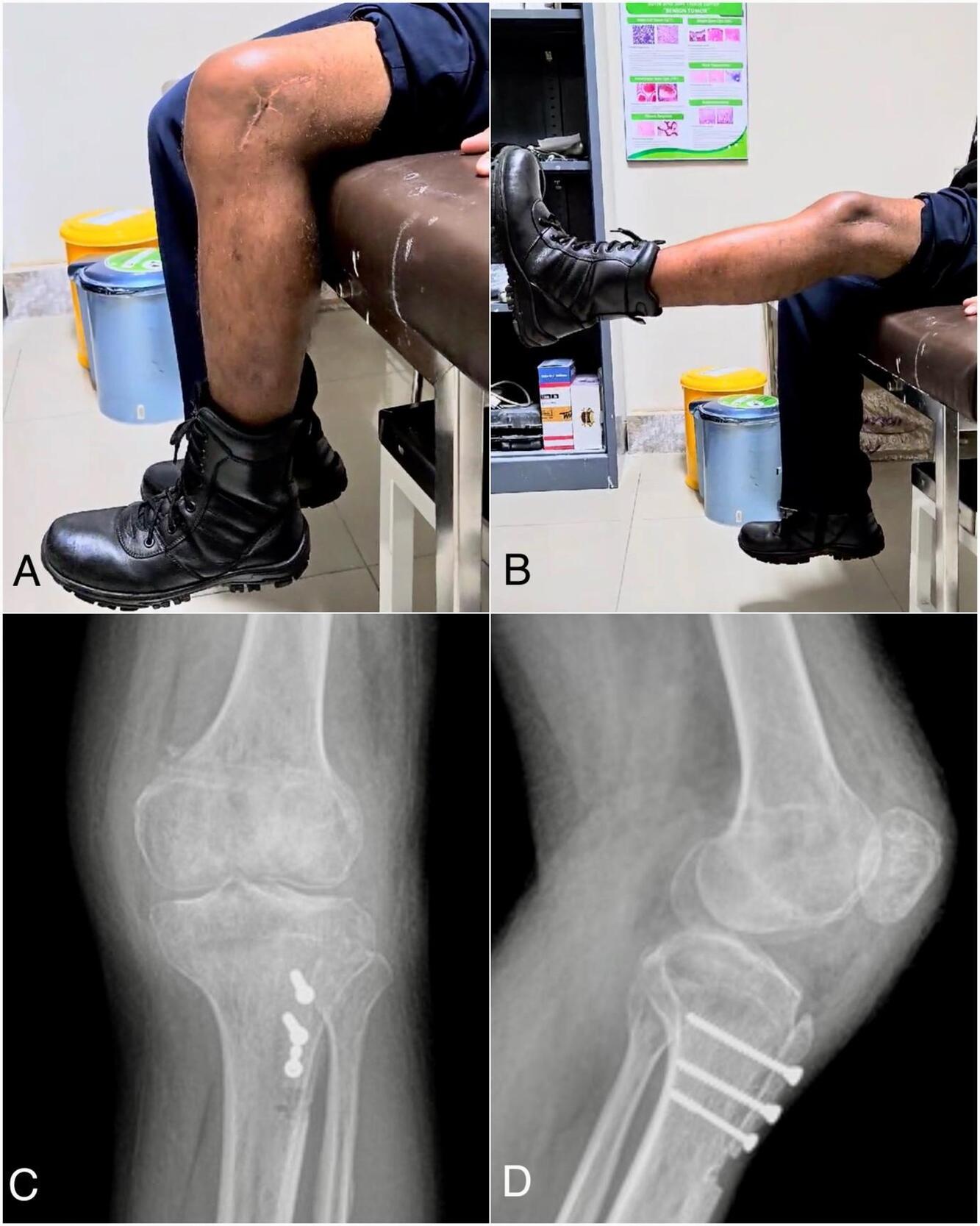
Following proximal and distal realignment, knee flexion-extension was performed to ensure optimal patellofemoral tracking. The surgery was completed (Fig 3D) and finalized with soft tissue and skin closure. After treatment, a knee brace was used to immobilize the patient’s knee for six weeks, at which point the rehabilitation procedure began. The patellar position then was confirmed by knee x-ray following the procedure (Fig 4), and it was supported by the Insall-Salvati ratio of 1.2 and the Caton-Deschamps ratio of 0.8.
_and_extension_(b)_occurs._good_.jpg)
Follow up
Follow-up conducted at six months and twenty months. The patient’s anterior based patellar position well-maintained. The physical examination indicated a flexion range of 100 degrees improve into 115 degrees and an extension maintain range of 0 degrees from the horizontal axis (Fig 4). Evaluation with clinical scoring showed an improvement, as indicated by the Tegner Lysholm score of 85 and the IKDC score of 80.5 (Table 1). Patient was satisfied with the results and able to go back to his regular activities with no recurrence dislocations.
Discussion
In adult patients, obligatory patellar dislocation is rare and typically persistent, characterized by chronic maltracking, soft tissue formation, shortening of lateral structures, and complex biomechanical modifications.6 Unlike pediatric cases, adult obligatory patellar dislocation is frequently associated with established chondral degeneration and reduced soft-tissue elasticity, which limits remodeling potential and necessitates definitive mechanical correction rather than growth-guided realignment.7 Therefore, its management often requires a more comprehensive reconstructive strategy
Medial soft-tissue insufficiency and contracture of the lateral structures and, less commonly, the quadriceps are the primary pathological causes of ODP.1 Quadriceps contracture compromises the extensor mechanism, reducing its length and excursion and preventing full knee flexion with the patella properly centered. The patella becomes laterally displaced along a shortened extensor trajectory, allowing flexion only when positioned laterally.8 Due to the complexity of the condition, no specific surgical method can provide optimal results in treating obligatory patellar dislocation.3 Proximal realignment alone may be inadequate in many reported adult ODP cases, and combining proximal and distal reconstructive techniques is therefore recommended,1 as found in our cases. Proximal procedures typically include MPFL repair, lateral release, and quadricepsplasty, while distal realignment involves tibial tuberosity transfer and partial medialization of the patellar ligament.9 The underlying pathology is primarily proximal, these procedures are generally performed before distal correction.3 These considerations guided the selection of the surgical combination in this case.
Lateral retinacular release has been a commonly performed procedure. It was once considered the standard treatment for anterior knee pain and patellofemoral instability due to its initially satisfactory outcomes.10 Currently, isolated lateral release is indicated only when excessive tension of the lateral retinaculum causes extensor mechanism imbalance during quadriceps contraction.11 Its purpose is to relax tight lateral tissues that pull the patella laterally, allowing proper tracking within the trochlear groove. However, isolated lateral release is no longer regarded as a definitive treatment, as it has shown poor long-term results with recurrent patellar dislocation.12,13
Short quadriceps muscles are associated with obligatory patellar dislocation, and it should be mentioned that the procedure necessitates tendon lengthening to keep the patella in its lower position after realignment. If the thumb test continues to be positive and the patella is laterally displaced during deep flexion following the release of the vastus lateralis, quadriceps tendon lengthening is required.10 Around 37% of patients required quadriceps tendon lengthening and noted that it was necessary in certain situations.3,14 The further advantages of the approach outlined above are as follows: It provides adequate elongation with a reduced risk of iatrogenic overlengthening, which may lead to extension lag. This approach enhances the balance between the medial and lateral soft tissues while adhering to the planes of dissection and innervation.14
In chronic cases, the MPFL is often absent or severely compromised. Therefore, semitendinosus-plasty is recommended to reduce lateral patellar displacement.15 The semitendinosus tendon assists in aligning the quadriceps mechanism with the femur’s intercondylar notch,14 effectively shifting the patellar tendon’s vector medially and providing a stabilizing medial tether¹⁹, Although evaluation criteria vary among studies, semitendinosus tenodesis has demonstrated good clinical outcomes, with success rates ranging from 62% to 88%.16
Persistent maltracking commonly causes lateral and inferior patellar cartilage lesions. Anteromedial tibial tubercle osteotomy reduces patellofemoral contact pressure, improves the extensor mechanism by lengthening its lever arm, unloads the lateral and inferior patellar facets, and corrects maltracking.17 Distal realignment of the patellofemoral mechanism through tibial tubercle anteromedial transfer has been extensively described for correcting patellar instability, patellofemoral malalignment with chondral lesions, and patella alta.1,17 In patients with increased tibial tubercle–trochlear groove (TT–TG) distance, patella alta, and patellofemoral cartilage damage from maltracking, this procedure also helps reduce the Q-angle and normalize the TT–TG distance.17,18
Utilizing the evaluation, we calculate the Insall-Salvati Ratio and Caton-Deschamps, which yield postoperative results of 1.2 and 0.8, confirm that the postoperative patellar height is within the normal range. This radiological outcome suggests that the combination of the surgical procedures used produced excellent results17,19. Although effective, this combined approach carries risks, including medial overconstraint, extension lag following quadriceps lengthening, and complications related to tibial tubercle osteotomy.20 However, none were observed in the present case.
Numerous studies have reported generally positive outcomes for various surgical methods used to treat obligatory patellar dislocation. However, no single technique has been established as the “gold standard”. Combination strategies have been described in several publications. Combined lateral release, anteromedial tibial tubercle transfer, and medial retinacular advancement, achieving good functional outcomes in most patients, though 12% experienced patellofemoral discomfort related to degenerative changes during long-term follow-up.1 Utilized patellar tendon transfer, semitendinosus tenodesis, lateral release, and proximal “tube” realignment, maintaining proper patellar tracking in all cases without the need for quadriceps tendon lengthening. They recommended early surgical intervention to facilitate trochlear groove development through improved patellar centering.16
A 4-in-1 quadricepsplasty involving quadriceps slide lengthening, lateral retinacular release and lengthening, and a modified Roux-Goldthwait patellar tendon hemi-transfer combined with Insall’s proximal “tube” realignment. This technique allows a single midline incision without the need for implants, intraoperative fluoroscopy, or grafts.2 A similar combined approach and, at a minimum 2-year follow-up, reported satisfactory patient outcomes, reliable patellar stability, and a 17.6% re-dislocation rate.21 Combined distal realignment via Roux-Goldthwait tendon split, medial plication using an overstretched capsule to cover the realigned patella, and extensive lateral release with proximal subperiosteal quadriceps realignment.22 Their study demonstrated improved patellar stability, range of motion, and quality of life in pediatric patients with congenital or obligatory patellar dislocation.2,21,22
The complexity of obligatory patellar dislocation suggested by most authors combines proximal reconstruction such as MPFL repair or grafting, lateral release, quadricepsplasty, and selective tendon lengthening with distal realignment techniques like tibial tubercle anteromedial transfer or partial medialization to correct maltracking, reduce patellofemoral pressure, and address patella alta or increased TT–TG distance. Quadriceps lengthening is often required when contracture persists, while semitendinosus tenodesis provides a medial tether in chronic cases. Reported outcomes across studies are generally positive, though no single technique is considered a gold standard. In our case, this combined approach restored normal patellar height (Insall–Salvati 1.2; Caton–Deschamps 0.8) and aligns with evidence supporting multicomponent surgical reconstruction for durable stability and function. Additionally, this procedure may offer a viewpoint on treating obligatory patellar dislocation in adults. A comprehensive clinical trial and long-term monitoring are required to evaluate the benefits, drawbacks, and long-term effects of this combination of methods.
Conclusion
This case illustrates that adult obligatory patellar dislocation requires a comprehensive, individualized surgical strategy. The combined approach of lateral release, quadriceps tendon lengthening, semitendinosus tenodesis reconstruction, and anteromedial tibial tubercle transfer was essential for correcting soft-tissue imbalance, restoring patellar tracking, and achieving stable alignment. While the favorable outcome supports the effectiveness of this single-stage technique, the report is limited by its single-patient design and the inherent inability of a case study to establish comparative effectiveness. Nonetheless, this case adds valuable insight into the reconstructive options for this rare and complex condition.