Background
Trigeminal neuralgia (TN) is a chronic and often debilitating facial pain disorder that is marked by recurrent, brief episodes of unilateral, electric shock-like pain within the distribution of the trigeminal nerve.1 The maxillary (V2) and mandibular (V3) divisions are the most frequently affected, with painful episodes lasting seconds to minutes and ranging from zero to over fifty times a day.1 Many patients experience a refractory period between paroxysms that lasts several minutes; however, those with longstanding TN may experience continuous dull pain between these acute paroxysms, further impairing quality of life.1
The pathophysiology of TN is most commonly attributed to the compression of the trigeminal nerve root entry zone, resulting in focal demyelination and subsequent ectopic impulse generation.2 Additionally, structural lesions such as brainstem tumors or demyelinating plaques can contribute to TN when they involve trigeminal pathways.3 Although TN is most frequently associated with neurovascular compression (classic TN), it can also be secondary to underlying conditions such as multiple sclerosis (MS), arteriovenous malformations (AVMs), or it may be idiopathic.
First-line treatment for classic and idiopathic TN typically involves anticonvulsant therapy, most commonly with carbamazepine or oxcarbazepine.1,4,5 For patients who are intolerant to these medications or have contraindications, alternative treatments include lamotrigine, gabapentin, or baclofen, with some benefiting from combination therapy.6 However, antineuralgic drugs are frequently associated with several side effects, including but not limited to megaloblastic anemia, drowsiness, ataxia, and hepatotoxicity.7
Surgical intervention is indicated for patients who are refractory to medical therapy and may be broadly categorized by the anatomic site of intervention. Intracranial procedures include microvascular decompression, which is performed in the posterior fossa, as well as stereotactic radiosurgery such as gamma knife treatment.8,9 Percutaneous central procedures targeting the trigeminal nerve at the skull base include radiofrequency thermocoagulation and various types of rhizotomy.8,9 Peripheral techniques are less invasive and target distal branches of the trigeminal nerve, including the supraorbital, infraorbital, alveolar, and lingual nerves, through approaches such as surgical incision, alcohol injection, radiofrequency thermocoagulation, or cryotherapy.1,9
Cryoneurolysis is a reversible, neuroablative technique that uses nitrous oxide at exceptionally low temperatures (-88 °C) to form ice balls around the targeted nerve, producing a cold zone that degenerates its axon and myelin sheath.10 The reversible degeneration of the axon (Wallerian degeneration) and myelin sheath temporarily blocks nerve conduction, resulting in immediate analgesia for the patient.11 Unlike cryoablation, the temperature is not too extreme to affect the structural components of the nerve (i.e., the epineurium, perineurium, and endoneurium remain intact), which allows the axon to regenerate along its original path at a rate of 1-2 mm per day until nerve signaling is fully restored.11 Depending on the distance from the axon injury site to the target site, the disruption of signaling and pain relief provided from cryoneurolysis can last from weeks to months.10 Currently, cryoneurolysis is clinically indicated for the relief of pain and symptoms associated with osteoarthritis of the knee for up to 90 days, but it is not indicated for the treatment of central nervous system-related pain disorders.10,12
Historically, cryotherapy applied to the peripheral branches of the trigeminal nerve has demonstrated favorable safety and efficacy. In a study comparing treatment options for trigeminal neuralgia, cryotherapy was found to have a low morbidity compared to radiofrequency thermocoagulation, which had resulted in more prolonged sensory loss (88%), anesthesia dolorosa (8%), and eye problems (15%).13 In a long-term prospective study, Bansal et al. treated 49 patients diagnosed with trigeminal neuralgia at several peripheral branches of the trigeminal nerve through cryosurgery using a cryoprobe with nitrous oxide at -98 °C.14 The study found that 96% of patients obtained pain relief for more than three years and 56.8% of patients for more than four years after treatment.14 Utilizing a transmucosal approach, Pradel et al. treated 19 patients using a cryoprobe to freeze branches of the trigeminal nerve at the infraorbital or inferior alveolar nerve.7 While partial restoration of sensory function occurred after 4-8 months, pain relief was maintained for at least 6 months for every patient.7
Case Presentation
Ethical Considerations
Patient-informed consent for publication was obtained from the patient. As the case report is devoid of patient identifiable information, it is exempt from IRB review requirements as per Montefiore Medical Center policy.
A 75-year-old female with a medical history of hypertension, stroke, non-ST-segment elevation myocardial infarction on clopidogrel therapy, and long-standing trigeminal neuralgia presented with refractory left-sided facial pain. The patient described severe burning and clicking pain localized to the left cheek, occurring approximately three to four times per year, with baseline, dull facial pain since adolescence.
Pharmacologic management included lamotrigine 125 mg twice daily, oxcarbazepine 600 mg twice daily, and 600 mg gabapentin three times daily. Despite combination therapy, pain relief was incomplete, and the patient experienced medication-related drowsiness. The patient had also received a trigeminal nerve block with 2 ml of 0.5% Marcaine, which provided transient relief but was followed by persistent, dull pain in the left cheek and flare-ups.
Management and Outcomes
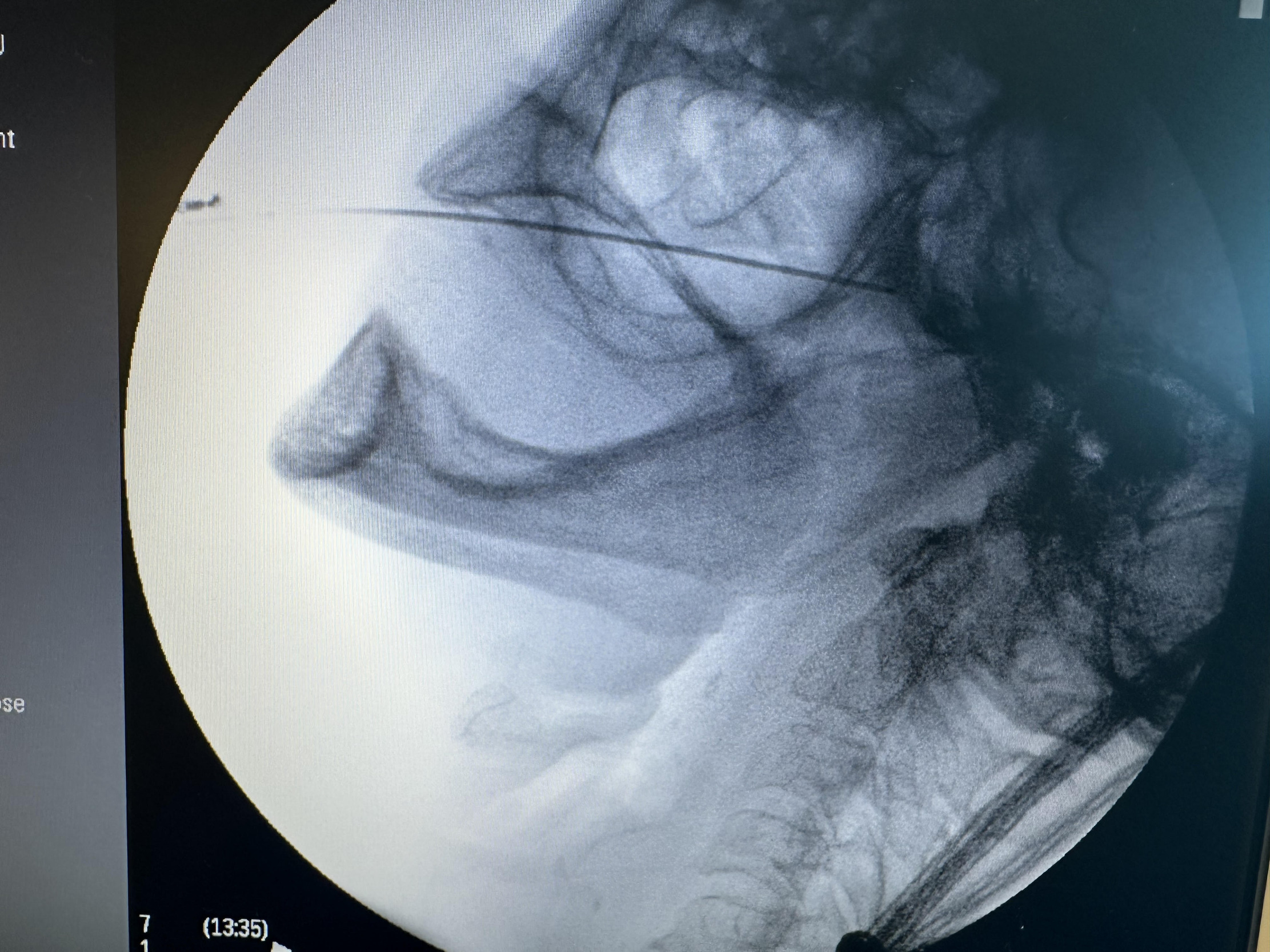
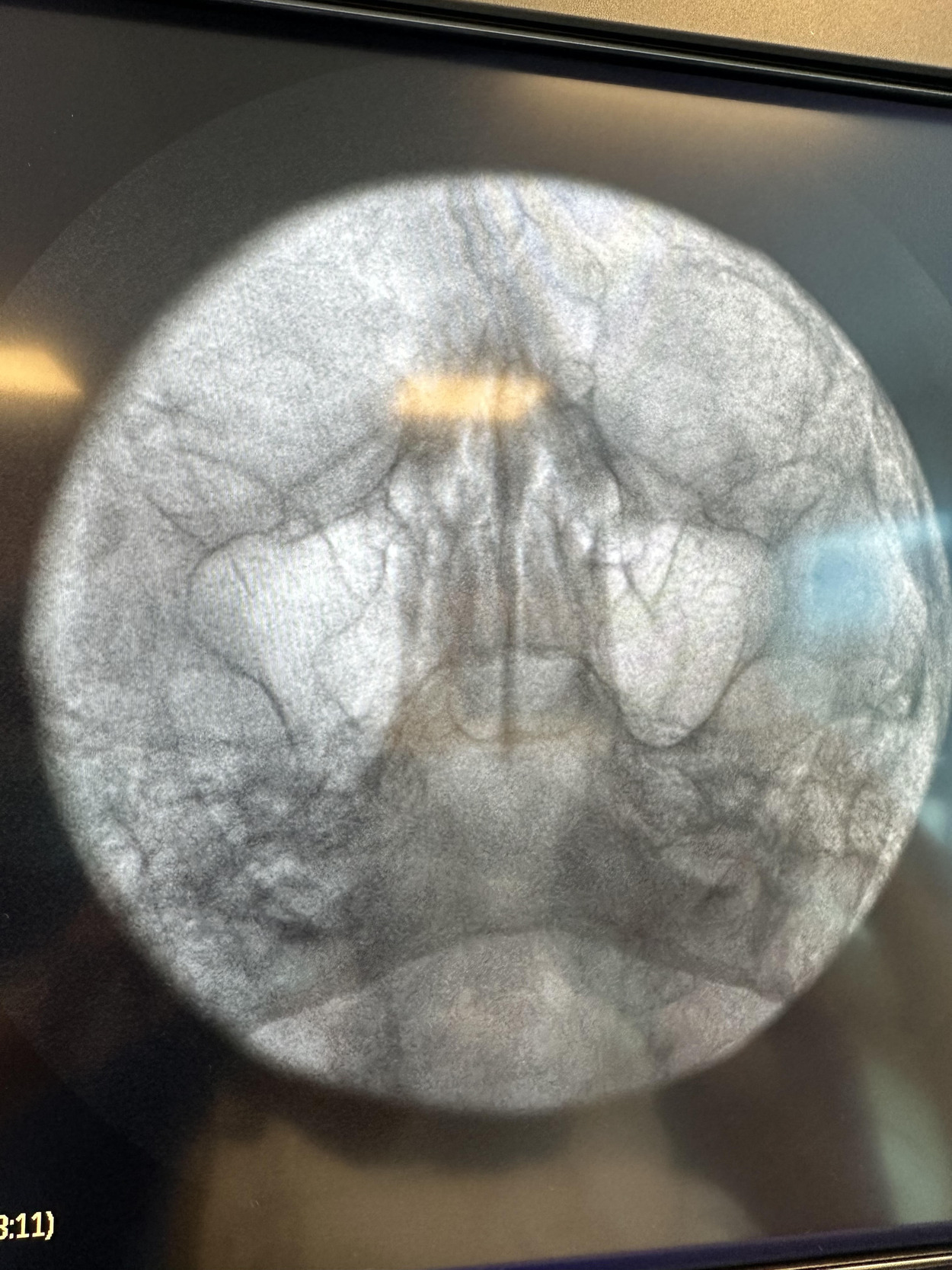
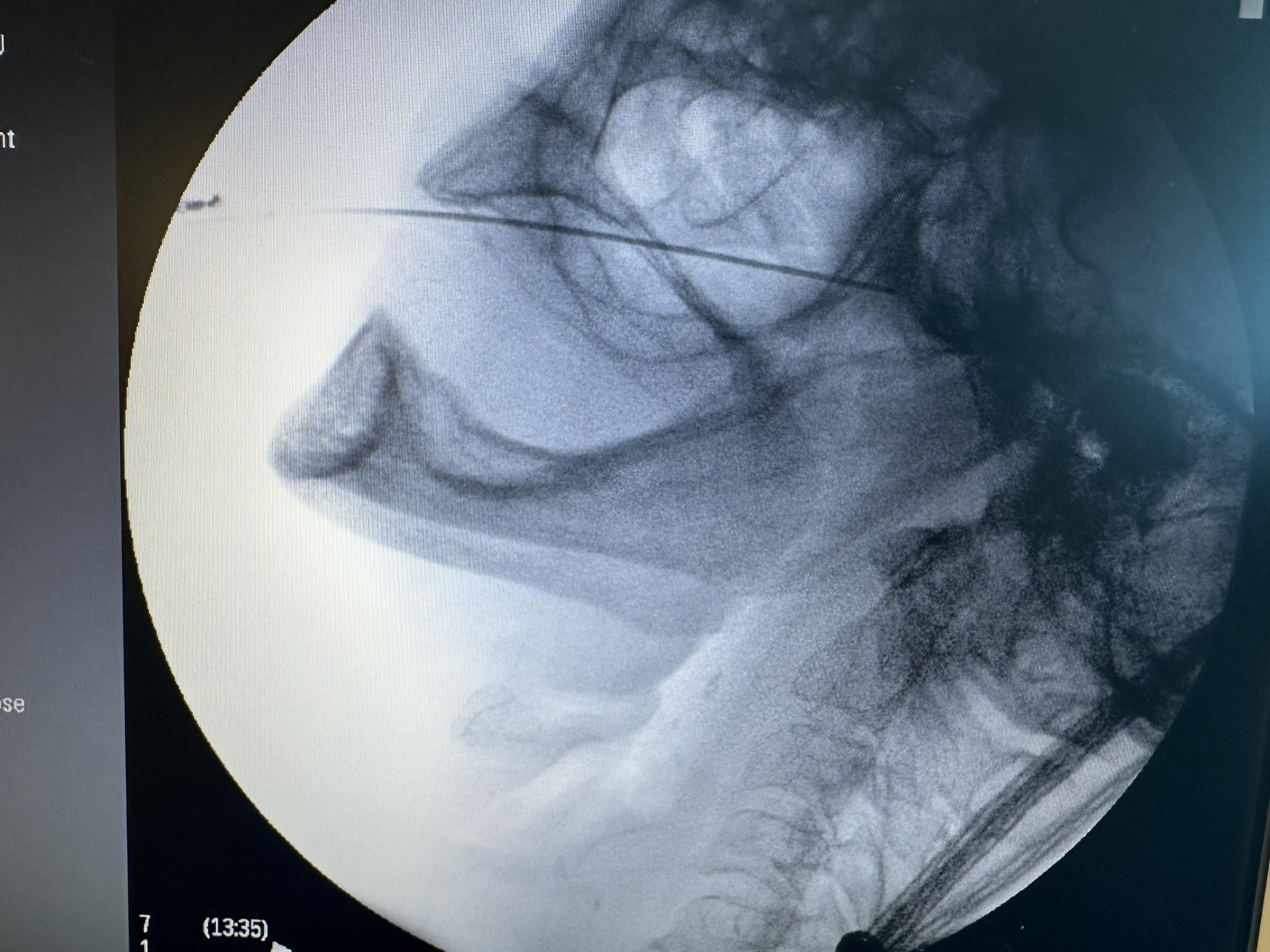
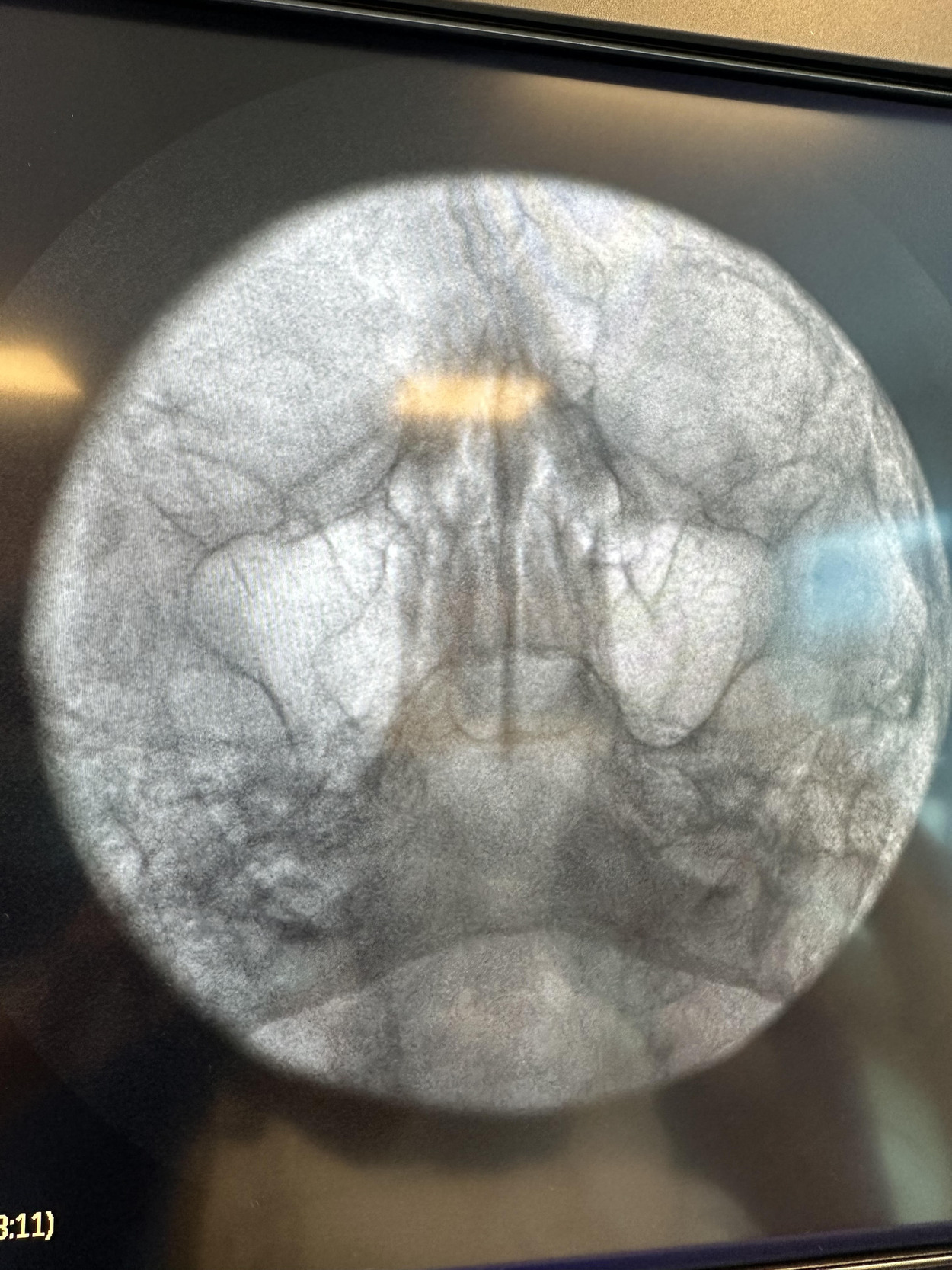
Given the patient’s refractory symptoms, medication intolerance, and elevated surgical risk, percutaneous cryoneurolysis was recommended. In April 2024, cryoneurolysis was performed at the ipsilateral foramen ovale targeting the V2 and V3 branches of the trigeminal nerve using a handheld cryotherapy device (iovera°, Pacira BioSciences, Inc., Brisbane, CA, USA). The procedure was performed under fluoroscopic guidance to confirm probe depth and alignment with the foramen ovale (Figures 1 and 2), and the patient tolerated the procedure well with no complications.
The patient reported an immediate reduction in pain from 7/10 to 2/10 following treatment. At one-month follow-up via telemedicine, she reported complete resolution of pain (0/10).
Conclusion
Currently, the use of a cryoneurolysis device is FDA-cleared for treating neuropathic pain associated with osteoarthritis and knee replacement surgery, but not specifically for trigeminal neuralgia.10 In this patient with idiopathic trigeminal neuralgia refractory to pharmacotherapy and nerve block, percutaneous cryoneurolysis targeting the V2 and V3 divisions resulted in rapid pain reduction and complete symptom resolution at a one-month follow-up without complications.
Unlike earlier cryotherapy techniques described in the literature that require surgical exposure of peripheral trigeminal branches, the approach utilized in this case was performed percutaneously under fluoroscopic guidance. This minimally invasive technique may be particularly useful for patients with significant medical comorbidities who are poor candidates for open surgical intervention.
While long-term outcomes and recurrence rates require further study, this case demonstrates that percutaneous cryoneurolysis can be a safe and effective treatment option for selected patients with refractory trigeminal neuralgia.
Authors’ Contributions
All authors contributed equally to the development, writing, editing, and submission of this manuscript.
Conflict of Interest Disclosures
Dr. Gritsenko reports the following conflicts of interest:
Consultant - Pacira
Advisory Board - Vertex
Further Information
No external funding was received.
A version of this work was previously presented as a poster at the 13th Annual New York & New Jersey Pain Medicine Congress (Jersey City, NJ; November 7–10, 2024) and at the ASRA Pain Medicine 24th Annual Pain Medicine Meeting (Austin, TX; November 13–15, 2025). The full manuscript has not been published elsewhere.