










1. INTRODUCTION
Compartment syndrome of the leg can cause serious and irreversible consequences, including severe deformity, chronic pain, neurological deficit, and limb loss if not decompressed promptly.1,2 While emergency fasciotomy remains the gold standard for the acute phase to release compartment pressure and limit muscle necrosis, diagnostic delays often lead to complex chronic sequelae. These typically manifest as Volkmann’s contracture, equinovarus deformity, and claw toes, posing major challenges for reconstructive surgery. Management of these sequelae must be tailored to severity and duration, ranging from Achilles tendon lengthening and tenolysis to tendon transfers or osteotomies in late stages.3
This article reports a rare case of late sequelae of missed compartment syndrome following open reduction and internal fixation (ORIF) of a tibial plateau fracture, describing a comprehensive reconstructive surgical strategy including the Bridle procedure and evaluating functional outcomes over a 6-year follow-up period.
2. CASE PRESENTATION
2.1. Patient information patient
A 41-year-old female sustained a Schatzker II lateral tibial plateau fracture following a traffic accident. She underwent initial management and ORIF surgery at a private hospital. Postoperatively, the patient reported progressive pain disproportionate to the injury, calf tightness, and paresthesia in the leg and foot but received no further intervention.
2.2. Clinical findings
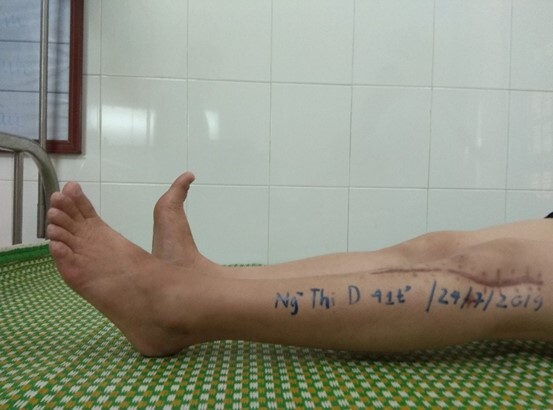
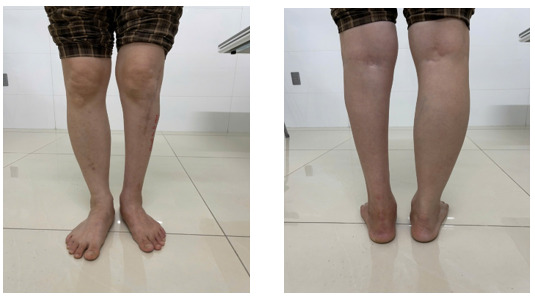
Six months post-ORIF, the patient presented to Thai Binh University of Medicine and Pharmacy Hospital with the following manifestations: Achilles tendon contracture resulting in gait difficulty; inability to perform a heel-to-toe gait; marked ankle stiffness; loss of active foot dorsiflexion; fibrosis of the anterior compartment muscles (palpable as a firm, immobile mass); paresthesia in the anterior leg and dorsum of the foot. Knee range of motion was preserved, and surgical scars were well-healed.
Diagnostic Assessment: Diagnosis was based on history, postoperative tightness, persistent paresthesia, contracture signs, muscle fibrosis, and foot deformity.
Clinical Diagnosis: Chronic sequelae of missed compartment syndrome following ORIF for tibial plateau fracture.
2.3. Timeline
2.4. Diagnostic assessment
The diagnosis was based primarily on patient history, reported postoperative tightness, persistent paresthesia, signs of contracture, muscle fibrosis, and foot deformity. Radiographs at 6 months showed the fracture had healed (Figure 3).
2.5. Therapeutic intervention
2.5.1. Surgical strategy
A combined surgical approach was planned to simultaneously address:
-
Contracture of the Achilles tendon, joint capsule, and flexor muscle group.
-
Neuromuscular imbalance (equinus foot, weak dorsiflexion, sensory disturbance).
-
Restoration of foot alignment and gait function.
2.5.2. Percutaneous achilles tendon lengthening
Three small incisions were made: (1) medial side near the calcaneal insertion (cutting 1/2 of the tendon); (2) lateral side, 2 cm proximal; and (3) medial side, 2 cm proximal to the second incision. Gentle dorsiflexion was applied to lengthen the tendon, and the ankle was immobilised in a neutral position. This technique minimises soft tissue invasion and reduces the risk of sural nerve injury.
2.5.3. Nerve and tendon release
-
Nerve: The common peroneal nerve was released at the fibular neck to improve sensory deficits.
-
Tendons: The flexor digitorum longus and tibialis posterior tendons were released to correct toe contractures and improve foot alignment and balance.


2.5.4. Bridle tendon transfer
To restore active dorsiflexion:
-
The tibialis posterior (TP) tendon was detached from its insertion at the navicular, routed behind the tibia, and passed through the interosseous membrane to the anterior compartment.
-
The peroneus longus (PL) tendon was sectioned at the distal third of the leg; its proximal end was sutured to the peroneus brevis (PB).
-
The distal end of the TP tendon was passed under the extensor retinaculum and fixed to the medial cuneiform with the ankle in neutral position, tensioned to approximately 80% of the tendon excursion.
-
Postoperative immobilization was achieved with a short leg cast for 6 weeks
3. MANAGEMENT AND OUTCOMES
3.1. Clinical results at 11 months follow-up
The patient had 0° of active ankle dorsiflexion, marked improvement in sensory disturbance, walked with a heel-to-toe gait, and had normal knee flexion/extension. Squatting was slightly difficult due to ankle stiffness.
3.2. Clinical Results at 6 Years Follow-up
-
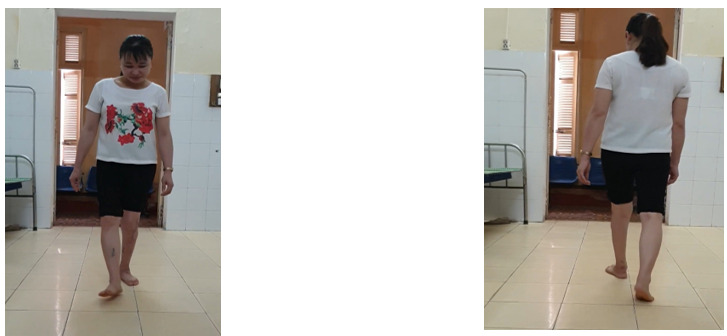
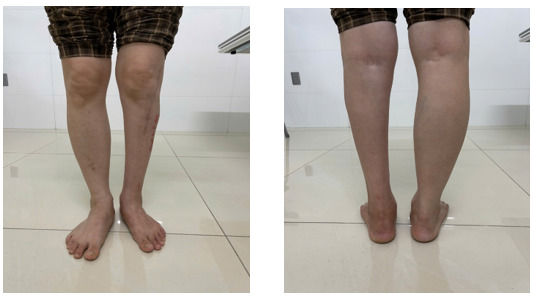
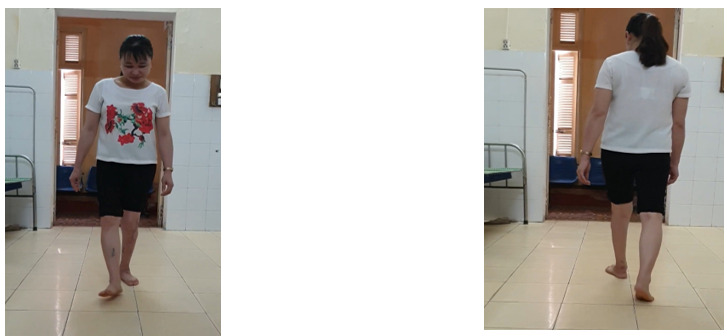
Active ankle dorsiflexion achieved approximately 5°, plantar flexion approximately 8°; knee flexion 0-120°. The patient could perform a single-leg heel raise, though reduced compared to the uninjured side.
-
No residual paresthesia. Ambulation was normal with a plantigrade foot, no foot drop, and no hindfoot malalignment.
-
Functional Assessment: The AOFAS Ankle-Hindfoot Scale score was 73/100, indicating fair-to-good functional recovery, with the patient maintaining daily activities and a relatively good gait.
4. DISCUSSION
Leg compartment syndrome is a clear orthopedic emergency that can lead to irreversible muscle necrosis, permanent nerve damage, and amputation if not decompressed promptly. While the presentation and management of acute compartment syndrome are widely described in the literature, missed or delayed diagnoses following internal fixation remain underreported and present major diagnostic and therapeutic challenges, particularly in proximal tibial fractures with significant soft tissue compromise, such as tibial plateau fractures.1,2 This case illustrates a rare but clinically significant scenario: chronic sequelae of unrecognized compartment syndrome following ORIF, successfully treated with a late reconstruction strategy yielding long-term functional results.
Tibial plateau fractures, especially in high-energy trauma, are often accompanied by severe soft tissue injury and prolonged edema. Even in the absence of classic signs of acute compartment syndrome, prolonged elevated compartment pressure can occur after ORIF due to factors such as extensive surgical exposure, periosteal stripping, prolonged tourniquet use, and rigid fixation. Studies on tibial plateau fractures have noted that the rate of compartment syndrome is not as low as previously thought, and the risk increases in severe injuries and comminuted fractures. Predictive models and studies also show the need for early vigilance in high-risk groups.4,5 In addition to the initial trauma mechanism, after ORIF, prolonged compartment pressure may also be contributed to through extensive surgical exposure, soft tissue dissection, tourniquet use, and changes in microcirculation in crushed tissue, causing some cases to not show “typical” symptoms but still progress to ischemia and muscle necrosis over time.3,4
A key challenge in late-diagnosed compartment syndrome is that symptoms may be more “silent” than in the acute phase. Manifestations often include disproportionate persistent pain, increasing analgesic requirements, pain on passive stretch, progressive sensory disturbance, firmness of the compartments, and reduced active motion. In our patient, early postoperative pain and paresthesia were not reassessed in a timely manner, leading to fibrosis, contracture, and muscle imbalance. Reviews on post-compartment syndrome sequelae emphasize that once fibrosis and deformity are established, simple compartment release is often insufficient.2,3
Therefore, treatment of chronic sequelae requires a comprehensive reconstruction strategy aimed at creating a plantigrade foot, improving alignment, balancing forces, and restoring gait function. Recommendations suggest that flexible deformities are suitable for tendon lengthening, release, and transfer, while rigid deformities may require more complex osteotomies or arthrodesis.2,3,6 In this case, we combined procedures to: (1) correct equinus via Achilles lengthening; (2) release contracted structures (flexors, tibialis posterior); (3) decompress the common peroneal nerve to address chronic neural symptoms; and (4) restore active dorsiflexion using the Bridle procedure.2,3,7
Restoring active dorsiflexion is crucial. The transfer of the tibialis posterior through the interosseous membrane is a classic technique, creating a “bridle” that distributes force and increases balance; it has been reported to improve gait and allow many patients to discontinue orthotics, even if strength does not fully return to normal.7,8 Our patient’s results are consistent with the literature: achieving a stable plantigrade foot, improved gait, reduced sensory symptoms, and maintained outcomes over 6 years.
Clinical lessons
This case provides important lessons in prevention and postoperative monitoring in patients with ORIF tibial plateau fractures. Surgeons need to carefully assess the soft tissue condition when planning bone fixation, consider phased surgery in the context of significant edema, avoid excessive periosteal dissection, and limit tourniquet duration. Postoperatively, compression bandages around the limb should be avoided, and close monitoring is necessary to detect early signs suggestive of compartment syndrome. Prolonged or progressively increasing pain, increasing need for analgesia, pain on passive extension, and progressive sensory disturbances should not be attributed simply to typical postoperative pain but should be re-evaluated promptly.4,5
The novelty of this report lies in the combination of compartment syndrome missed after ORIF tibial plateau fractures, the application of a multimodal late reconstruction strategy, and the recording of long-term functional outcomes with a follow-up period of up to 6 years. Such long-term follow-up data following late intervention are rarely reported and provide further evidence that significant functional improvement can still be achieved even in chronic cases, when appropriate regenerative principles are applied.2,3,7
Limitations: Several limitations of this report must be acknowledged. First, this is a single case report. Second, objective assessments such as intracompartmental pressure monitoring, electromyography, or advanced imaging modalities to quantify muscle and nerve damage were not available. However, the detailed clinical documentation combined with long-term follow-up reinforces the value of this case, highlighting key issues in both the prevention and treatment of missed compartment syndrome.2,3
This case highlights several important practical considerations for surgeons performing ORIF for tibial plateau fractures, particularly in the context of high-energy trauma with complex soft tissue injury. Surgeons must adhere to the principle of respecting soft tissue condition, carefully consider the fixation strategy in cases of significant edema, limit excessive periosteal dissection, control tourniquet duration, and thoroughly assess compartment tension before closing the incision. It is crucial to emphasize that successful fixation does not eliminate the risk of compartment syndrome; therefore, postoperative monitoring, including avoiding occlusive dressings and early identification of warning signs such as disproportionate pain or prolonged paresthesia, is just as important as the fixation technique itself. Ultimately, maintaining an early threshold for suspected compartment syndrome, increased monitoring, or early fasciotomy when postoperative pain is disproportionate to the extent of injury is important, but even if the diagnosis is missed, late sequelae can still be significantly rehabilitated if the correct reconstruction strategy is applied.
5. CONCLUSION
Missed or late-diagnosed compartment syndrome after ORIF of tibial plateau fractures can cause deformity and long-term functional impairment. Close postoperative monitoring and clinical awareness are essential for prevention. In chronic cases, a comprehensive and individualized reconstruction strategy combining percutaneous Achilles lengthening, nerve release, tendon release, and Bridle tendon transfer can provide meaningful functional improvement, even years after the injury.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.

.jpg)







_compared_to_the_uninjured_side.jpg)