

Introduction
Hip fractures are among the most common fragility injuries worldwide and are associated with catastrophic individual and socioeconomic consequences.1 FNFs account for approximately 50% of hip fractures and predominantly affect older women, reflecting the higher prevalence of osteoporosis and fall-related injuries in this group.2 Despite decades of research, the optimal management of FNFs, particularly the balance between fixation and arthroplasty in various patient subgroups remains controversial.3,4 Displaced FNFs are typically treated with arthroplasty, in contrast minimally displaced fractures are frequently managed with IF despite evidence of high failure and reoperation rate.5,6 In parallel, advances in arthroplasty, including the adoption of DM designs, the use of larger femoral heads, and refinement of surgical approaches, have aimed to mitigate dislocation and revision risks within this high-risk population.7,8
Mortality rates following FNFs remain alarmingly high, ranging from 5–10% at 30 days to 33–36% at one year, depending on patient comorbidities and fracture type.9,10 These figures highlight the critical importance of timely surgical intervention, judicious implant selection, and coordinated multidisciplinary care pathways. National audits, such as the UK National Hip Fracture Database (NHFD), document over 72,000 hip fractures annually, with associated costs exceeding £2.1 billion.11 In the United States, approximately 300,000 elderly patients sustain fragility hip fractures each year, representing a major contributor to Medicare expenditure.12 Globally, the projected rise in incidence driven by the aging population underscores the urgent need for efficient and evidence-based treatment algorithms.1
Epidemiology of FNFs
The global burden of FNFs reflects an accelerating public health challenge driven by ageing populations and the rising prevalence of osteoporosis. In the United Kingdom (UK), approximately 101,000 cases are recorded annually,11 while worldwide hip fracture incidence is projected to exceed 21 million by 2050.1 In the United States, FNFs account for nearly 300,000 hospitalisations each year, representing a substantial healthcare burden.12 Across high-income regions, incidence rates range from 200 to 400 per 100,000 person-years among individuals older than 80 years.13 Women are consistently over-represented, comprising up to 70% of cases in contemporary series, a disparity attributed to higher rates of osteoporosis and longer life expectancy.2,14
FNFs carry particularly high mortality. One-month postoperative mortality ranges from 5–10%,9 and one-year mortality is consistently around 30–36%.10,15 Comorbid conditions strongly influence survival; for example, patients with dementia have 180-day mortality of 31.8% after surgery versus 45.7% if managed non-operatively.16 Advanced age, male sex, and higher ASA grade are independent predictors of death after FNF.17
Healthcare utilisation associated with femoral neck fractures remains substantial. The mean hospital length of stay (LOS) following arthroplasty for a femoral neck fracture ranges from 11 to 14 days, consistently longer than for elective total hip arthroplasty (THA).18 According to the UK National Hip Fracture Database (NHFD), only around 30% of eligible patients receive THA for displaced fractures, reflecting both resource limitations and concerns regarding procedure-related complications.11 In contrast, registry data from Australia and Sweden report a higher proportion of hemiarthroplasties relative to THA, largely influenced by surgeon preference and healthcare system capacity.19,20
The economic burden is equally significant. In the UK, initial inpatient costs average approximately £6,394 for internal fixation and £7,633 for THA; however, long-term expenditure favours arthroplasty, as fixation failures frequently necessitate costly reoperations.21 Globally, the projected economic impact of femoral neck fractures is expected to exceed $131 billion annually by 2050 if current incidence trends persist.22
Classification Systems
Accurate classification of FNFs is critical to guiding treatment, yet reliability remains a major concern. The Garden classification, first described in 1961, categorises FNFs into four stages based on displacement and alignment.23 Garden I–II fractures (incomplete or nondisplaced) have high union rates, with reported union rates of 100% in Garden I and 93% in Garden III fracture patterns, while Garden IV fractures show union rates as low as 57% due to vascular compromise.24 However, interobserver reliability is limited, with κ values between 0.31 and 0.76 across studies.14,25
The Pauwels classification, which is based on fracture line inclination, categorises fractures into type I (<30°), type II (30–50°) and type III (>50°). It was intended to reflect shear stress and predict fixation failure.26 However, reliability is again poor, with κ values as low as 0.46, and the system has limited prognostic validity in contemporary practice.27
The AO/OTA classification evaluates the fracture location and morphology; however, it is similarly limited by interobserver agreement with a κ value of 0.62.25 Simplification into displaced versus undisplaced categories improves reliability, with κ increasing from 0.31 to 0.51 in some studies.28
Radiographic modifiers including posterior tilt and varus angulation provide more robust prognostic information. Posterior tilt ≥20° on lateral radiographs is consistently associated with increased fixation failure risk.29,30 In international surgeon surveys, more than 69% reported using posterior tilt ≥20° as a threshold for recommending arthroplasty over fixation.31 Similarly, neck-shaft angle >160° and varus malalignment are significant predictors of non-union or failure after fixation.30
Despite the above classification systems, none reliably predict outcomes across all patient groups. Contemporary management therefore combines classification with patient-specific factors such as age, comorbidity, cognitive status and pre-fracture mobility.32
Surgical Timing and Perioperative Considerations
Timely surgery is widely recognised as one of the most critical modifiable determinants of outcome following femoral neck fractures. Robust evidence demonstrates that early operative intervention, ideally within 24 to 48 hours of admission, significantly reduces morbidity and mortality. In a meta-analysis of more than 190,000 patients, Moja et al. reported a 20% reduction in 30-day mortality when surgery was performed within 48 hours.33 Similarly, Nyholm et al. found that surgical delays beyond 12 hours (p = 0.02), 24 hours (p = 0.02), and 48 hours (p = 0.02) significantly increased 30-day mortality, while delays exceeding 24 hours also increased 90-day mortality rates (p = 0.04) and independently predicted higher complication rates and overall mortality.34 Corroborating evidence from the UK, drawn from a cohort of more than 200,000 patients, demonstrated that each additional 24-hour delay beyond the 48-hour threshold increased 30-day mortality by approximately 8%.35 Despite this compelling body of evidence, the NHFD continues to report that only 69% of patients undergo surgery within the recommended 36-hour window, underscoring the persistent disparity between evidence and clinical practice.11
Concerns regarding surgery performed at night have also been raised in the past, with surgeon fatigue contributing to higher complication rates. However, more recent registry analyses suggest that the absolute timing of surgery within a 24-hour cycle is less relevant than the overall delay duration.36 Optimisation of comorbidities, including anticoagulation reversal or stabilisation of decompensated medical conditions, remains essential, however, consensus guidelines emphasise that such optimisation should not lead to prolonged postponement of definitive surgery.37
Perioperative optimisation plays a pivotal role in improving outcomes following arthroplasty for FNFs. Intraoperative blood loss is consistently greater in arthroplasty performed for FNFs compared with elective THA, averaging 340 mL versus 310 mL, respectively (p < 0.001), contributing to higher transfusion requirements.18 Adjunctive use of tranexamic acid has been shown to reduce perioperative transfusion rates by 30–40% without increasing thromboembolic complications in this cohort.38 Anaesthetic technique is another important determinant of outcome. In a meta-analysis of more than 10,000 patients, Guay et al. reported that spinal anaesthesia was associated with a 14% reduction in 30-day mortality compared with general anaesthesia (p = 0.01) .39 However, results from large, randomised trials, such as the REGAIN study, found no significant differences in survival or functional recovery between the two modalities.40 Postoperative analgesia remains equally vital; multimodal pain management strategies have been shown to reduce the incidence of delirium, affecting 15–25% of patients after hip fracture surgery, while enhancing early mobilisation and functional outcomes.41
Rehabilitation and Nutritional Support
Nutritional optimisation similarly reduces complication rates, shortens hospital stay, and improves both functional recovery and survival outcomes. Vitamin D supplementation has proven effective; in one trial, a 250,000 IU loading dose administered within seven days of surgery reduced falls, improved pain scores, and achieved higher repletion rates. Conversely, anabolic steroids (nandrolone 2 mg/kg weekly for 4 weeks) yielded minimal functional or biochemical benefits, while growth hormone secretagogue mimetics were associated with increased adverse events.42,43
A systematic review evaluating 109 high-quality randomised controlled trials, comprising 39 unique interventions across 56 publications, reported that early ambulation within 48 hours post-surgery improved functional recovery and shortened hospital stays. Patients mobilising on days 1–2 demonstrated higher independence compared with those starting on days 3–4. Intensive physiotherapy, including two additional daily sessions, reduced hospital stay and dependency, though not consistently mobility scores. Outpatient strategies, including telerehabilitation and tailored 12-month home programs with 5–6 physiotherapist visits, significantly improved long-term mobility and balance. Adjunct modalities such as neuromuscular stimulation and pulsed electromagnetic field therapy (daily for 6–12 weeks) enhanced walking speed, postural stability, and pain relief.42,43
Internal Fixation
IF has long constituted the cornerstone of management for undisplaced (Garden I–II) femoral neck fractures, particularly among physiologically younger and more active patients. The theoretical advantages of IF include preservation of the native femoral head, avoidance of arthroplasty-specific complications, reduced soft tissue trauma, and shorter surgical duration.23,24,44 Accumulating evidence, however, has shifted clinical consensus regarding its durability in older populations, with large registry and cohort studies reporting reoperation rates of 10–20% due to fixation failure, non-union, or avascular necrosis.45,46 Consequently, contemporary management increasingly favours primary arthroplasty in elderly patients, even for minimally displaced fractures to optimise functional recovery and minimise the risk of subsequent revision surgery.
Failure rates following IF in elderly patients remain unacceptably high. In a meta-analysis of 25 studies encompassing more than 4,600 patients, Upadhyay et al. reported failure rates ranging from 20% to 36% for undisplaced FNFs managed with either cancellous cannulated screws or sliding hip screws (p < 0.001) .45 Registry data further substantiates these findings, the Norwegian Hip Fracture Registry documented a 29% reoperation rate at two years following IF, compared with only 4.8% after arthroplasty in patients aged over 70 years (p < 0.001).46 Similarly, In a multicentre trial involving 219 patients aged ≥70 years with nondisplaced femoral neck fractures, Dolatowski et al., reported that the reoperation rate was markedly higher after screw fixation (43%) compared to (6%) in the hemiarthroplasty cohort (p < 0.001).47
The underlying reasons for IF failure are multifactorial and often interrelated. Non-union and avascular necrosis (AVN) remain the predominant contributors, with non-union rates reported as high as 30–45% in displaced femoral neck fractures treated with screws in older adults.48 Radiographic factors also exert a significant influence; a posterior tilt of ≥20° has consistently been associated with a three- to fourfold increase in the risk of fixation failure.29,30 Accordingly, many authors consider such fractures biomechanically comparable to displaced injuries and advocate primary arthroplasty rather than fixation in this context.31
Technical factors are equally critical determinants of fixation success. Among available constructs, cannulated screws remain the most frequently employed; however, biomechanical studies have demonstrated that sliding hip screws (SHS) provide superior resistance to shear and rotational forces, particularly in vertically oriented (Pauwels III) fracture patterns.49,50 Despite this theoretical advantage, clinical outcomes have not mirrored biomechanical expectations as reoperation rates remain high, and no construct has demonstrated clear superiority in comparative studies .50 Various augmentation techniques, including the use of bone grafts or cement, have been explored, yet current evidence fails to show consistent improvements in union rates or overall functional outcomes.51 Collectively, these mechanical and biological limitations underscore why contemporary management has increasingly shifted toward arthroplasty in elderly patients, where fixation reliability is predictably compromised.
Patient age and pre-injury functional status remain pivotal determinants in selecting the optimal treatment strategy for FNFs. In physiologically younger patients, typically under 60 years of age, preservation of the native femoral head is prioritised, given the finite longevity of arthroplasty implants and the increased risk of revision in this age group.52 In contrast, outcomes in older adults strongly favour arthroplasty. Large cohort and registry studies, including those by Dolatowski et al. and Gjertsen et al., have demonstrated markedly higher fixation failure and reoperation rates in patients over 70 years compared with those undergoing arthroplasty (p < 0.001).37,47 These findings have informed changes in treatment algorithms, which now increasingly advocate for arthroplasty, even for minimally displaced fractures in elderly or low-demand patients in order to optimise functional recovery and reduce the burden of revision surgery.
Hemiarthroplasty (HA)
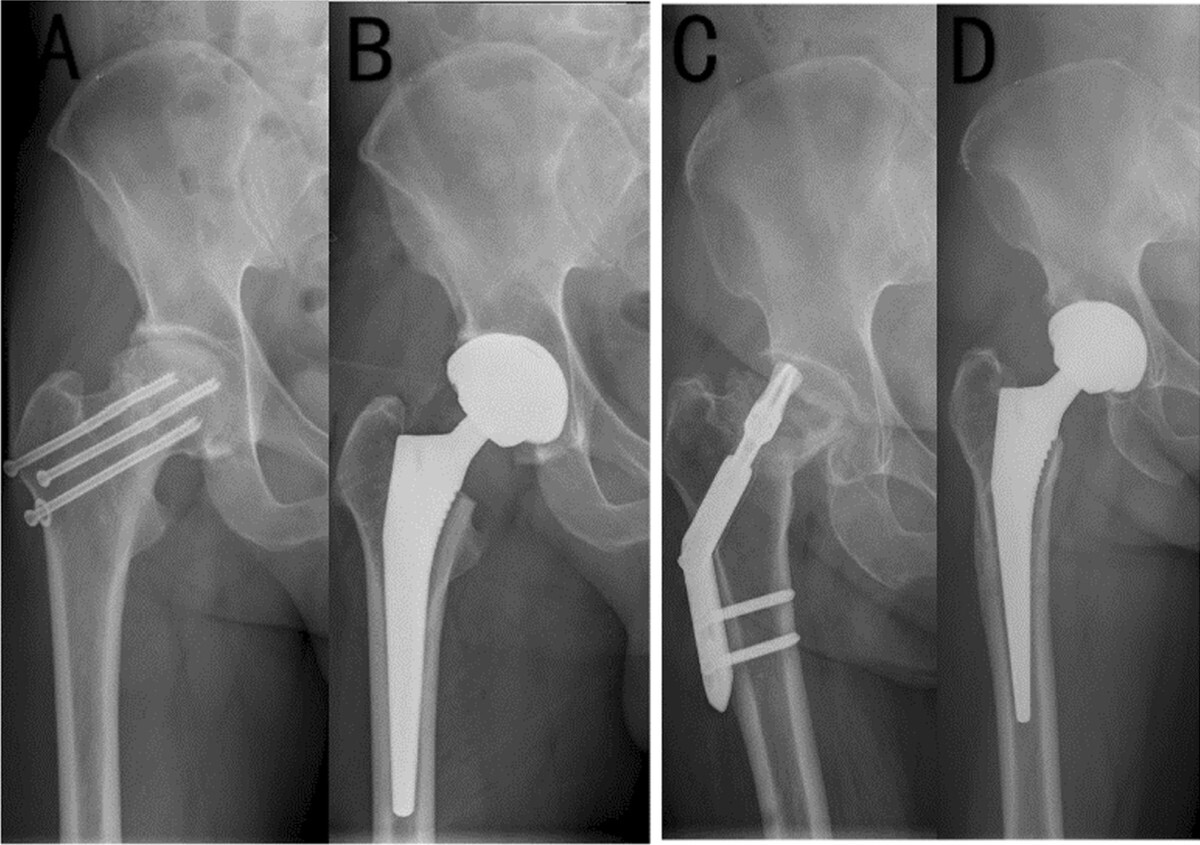
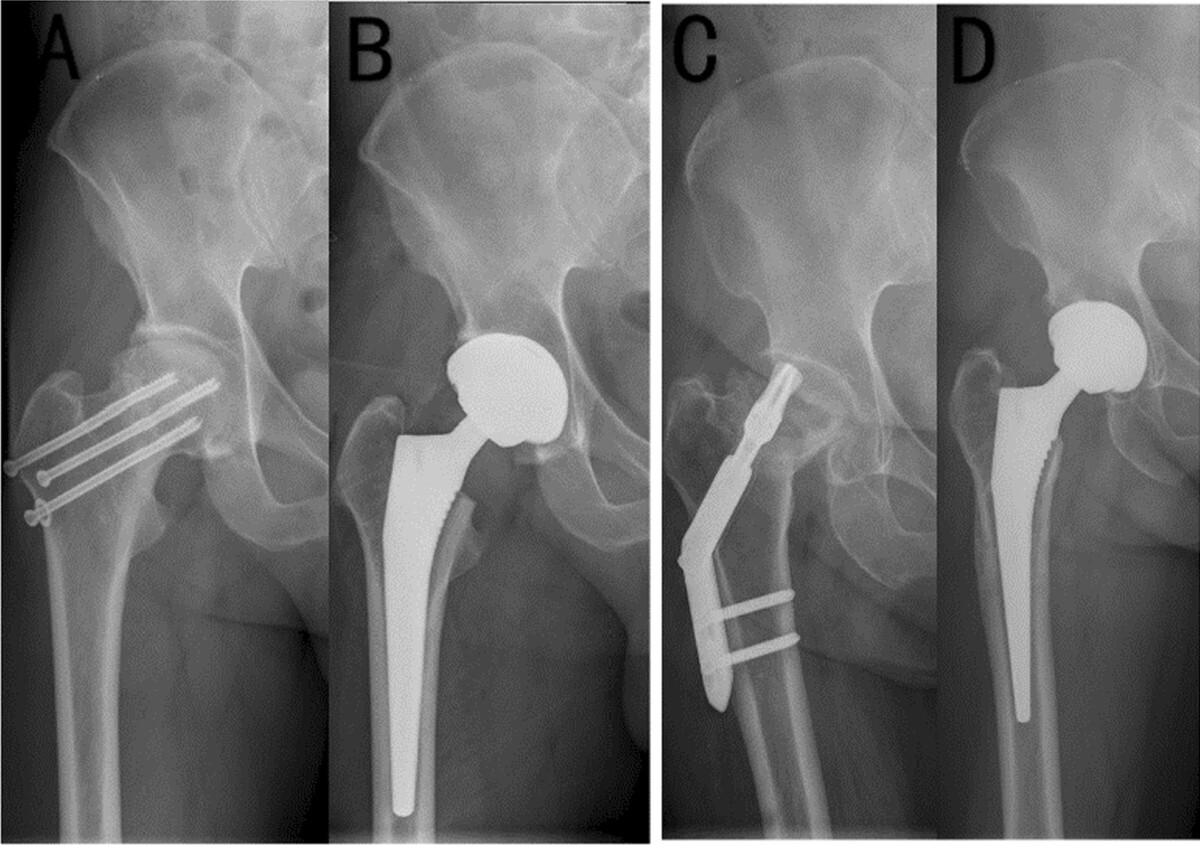
Worldwide, HA remains the most frequently performed procedure for displaced FNFs, particularly in patients over 70 years of age or those with significant medical comorbidities.11,19 (Figure 1) Although technically less demanding and faster to perform than THA, HA offers a lower risk of dislocation and reliably restores mobility in frail, low-demand patients. However, these short-term advantages are counterbalanced by long-term risks, including acetabular erosion, inferior functional outcomes compared with THA, and, in some cases, the subsequent need for conversion to THA.53
_and_pos.jpeg)
The choice between unipolar and bipolar prostheses remains a subject of ongoing debate in the management of displaced FNFs. Bipolar designs were developed to reduce acetabular wear by incorporating an additional inner bearing surface; however, long-term evidence has not demonstrated any meaningful clinical advantage. In a Cochrane meta-analysis of 1,655 patients, Lewis et al. found no significant difference in pain, revision rates, or functional outcomes between unipolar and bipolar HA (p > 0.05).54 Similarly, Leonardsson et al. reported comparable 10-year revision rates of 4–6% for both implant types (p = 0.72).20 Accordingly, prosthesis selection in this context is often driven by cost considerations and surgeon preference rather than proven clinical superiority.
In contrast, the choice between cemented and uncemented fixation carries greater clinical significance. Cemented stems provide superior initial stability, lower risks of periprosthetic fracture (PPF), and improved early mobility.55 The WHISH trial which included 1,125 patients demonstrated a significantly lower PPF rate with cemented HA compared with uncemented stems (p < 0.01) .56 While infrequent, bone cement implantation syndrome (BCIS) remains a recognised intraoperative complication, occurring in approximately 1–2% of frail elderly patients.57 While infrequent, BCIS remains a recognised intraoperative complication, occurring in approximately 1–2% of frail elderly patients.57 In view of this balance of risks and benefits, the overall advantages of cemented fixation particularly its superior implant stability, lower periprosthetic fracture risk, and facilitation of early mobilisation substantially outweigh the potential complications. Accordingly, most national and international guidelines endorse cemented HA as the standard of care for older adults.37
Functional outcomes following HA are favourable in restoring mobility and independence; however, they remain inferior to those achieved with THA. The HEALTH trial demonstrated no significant difference in the primary endpoint of secondary procedures at 24 months when comparing HA with THA (p = 0.79) .58 In contrast, patients undergoing THA exhibited statistically significant improvements in WOMAC and EQ-5D scores (p < 0.05), although these gains did not reach the minimal clinically important difference (MCID).58 Further analyses of healthier patients (≤70 years, ASA I–II) similarly found no clinically meaningful functional advantage of THA over HA, emphasising the critical role of patient selection in optimising outcomes.59
Mortality rates following HA remain a critical outcome measure, with 30-day mortality typically reported between 7–10%, comparable to rates observed after THA.10,60 Major complications are less frequent however clinically significant. Periprosthetic dislocation occurs in approximately 1–2% of cases which is substantially lower than the rates reported following THA for FNFs.61,62 Cemented implants further reduce the risk of PPFF, although the potential for BCIS remains a recognised consideration in frail elderly patients.57
Registry data and health-economic analyses provide valuable context to these clinical outcomes. Data from the Swedish Hip Arthroplasty Registry demonstrate a 10-year revision rate of 5%, with acetabular erosion emerging as the principal indication for revision.20 From an economic standpoint, HA is associated with lower initial inpatient costs, estimated in the UK at approximately £6,394 compared with £7,633 for THA.21; however, its long-term cost-effectiveness is diminished by the higher incidence of acetabular wear and the subsequent need for revision arthroplasty in a subset of patients.
Total Hip Arthroplasty (THA) in FNFs
THA has increasingly been adopted for the management of displaced FNFs in selected patients, particularly those who are younger, higher functioning, and medically fit. Evidence consistently shows that THA offers superior functional outcomes compared to HA, although at the cost of higher complication rates. (Figure 2)

In a comparative analysis, Smith et al. evaluated 864 THAs, including 338 for displaced FNFs and 526 for osteoarthritis (OA).18 FNF patients were significantly older (mean >75 years), more often female (62.4% vs 47.7%), and more likely to receive cemented fixation (72.2% vs 43.0%; p < 0.001). They also required greater perioperative resources, with higher mean blood loss (340 vs 309 mL; p < 0.001), increased transfusion needs (1.54 vs 0.87 units), and longer hospital stays (13.4 vs 11.1 days; p < 0.001). Despite these factors, one-year Harris Hip Scores were equivalent to those of elective OA cases (94.9 vs 96.6; p < 0.001), demonstrating that THA can achieve excellent functional recovery even in higher-risk fracture populations. These results reinforce that, with careful patient selection and optimisation, THA offers outcomes comparable to elective surgery despite the added perioperative burden.
Although THA may yield marginally superior functional scores compared with HA, the clinical relevance of this difference remains limited. Evidence from the HEALTH trial indicates that these functional gains rarely exceed the minimal clinically important difference, and are most evident in highly functional, independent older adults.58,59 Accordingly, the decision to perform THA should prioritise physiological fitness and pre-injury functional status rather than chronological age alone.
Complications remain the principal limitation of THA in fracture populations. Berry et al. reported on 217 THAs performed for displaced FNFs at the Mayo Clinic, demonstrating a 5-year cumulative revision rate of 8%, substantially higher than the 2–4% revision rate typically observed at 10 years for elective THA (p < 0.01).63 PPFFs accounted for the majority of revisions (7% at 5 years), underscoring the biomechanical vulnerability of osteoporotic bone. Dislocation risk was strongly approach-dependent, with all dislocations occurring following the posterior approach (p < 0.001).63 The 5-year incidence of periprosthetic joint infection (PJI) was also higher than in elective THA (3% vs 1.5%; p < 0.05).63
Surgical exposure influences early recovery and complication rates. In a randomised controlled trial, Blomfeldt et al. compared the direct anterior (DAA) and direct lateral approach (DLA) in 130 FNF patients and found no significant difference in Timed Up-and-Go scores at six weeks (p = 0.41).64 However, Forgotten Joint Scores (FJS) were significantly higher with DAA during the first 12 weeks (p < 0.05), with outcomes converging by one year. Trendelenburg gait developed in seven patients following DLA but in none treated with DAA.64 Registry analyses corroborate these findings, demonstrating higher dislocation rates with posterior exposures compared to anterior-based approaches.63
Despite the elevated perioperative risk profile, registry data confirm the long-term durability of THA for FNFs. The Swedish Hip Arthroplasty Registery reports 10-year implant survival exceeding 90%, albeit slightly lower than that observed for OA cohorts (p < 0.05).20 Patient-reported outcome measures (PROMs) further support THA’s advantage over HA, demonstrating consistently higher patient satisfaction and functional scores, even when absolute differences remain modest.58
Dual Mobility (DM) Arthroplasty
Instability remains the most common complication of THA after FNF, and DM constructs have emerged as a strategy to mitigate this risk. The design incorporates a mobile polyethylene liner within a fixed metal shell, creating two articulating surfaces and increasing jump distance.
Registry data strongly support the stability advantage of DM. The Swedish Hip Arthroplasty Register, analysing >10,000 THAs performed for FNFs, found that dislocation rates were significantly lower with DM compared to conventional THA (1.3% vs 2.2% at two years when posterior approach was used).65 A multicentre French registry reported similar findings, with dislocation incidence reduced by 50–70% in elderly fracture populations when DM was employed.66
Randomised controlled trial data remain limited, but observational cohorts are consistent. In a large matched study, DM reduced dislocation rates without increasing revision for other causes.67 However, infection remains a leading cause of DM revision, with cumulative rates of 2–3% at five years, which is similar to conventional THA in this setting.63,66 Some series suggest higher heterotopic ossification with DM, though this has not been associated with poorer PROMs.68
Concerns about long-term polyethylene wear and intraprosthetic dislocation persist. However, modern highly crosslinked polyethylene has significantly reduced this risk, with 10-year survival of DM constructs exceeding 95% in fracture cohorts.69 The additional cost of DM implants has been offset in several economic models by reductions in revision and reoperation rates secondary to dislocation.70
Overall, DM THA is increasingly considered the implant of choice for displaced FNFs in active elderly patients at high risk of dislocation, particularly those requiring posterior approach exposure.65–67
Comparative Outcomes: IF vs HA vs THA
The comparative evidence base between IF, HA and THA has expanded significantly in the last decade.
For minimally displaced FNFs, IF remains widely used, however failure rates are high. Dolatowski et al performed a randomised control trial demonstrating a reoperation rate of 43% after screw fixation compared with only 6% after HA.47 Posterior tilt ≥20° was the strongest predictor of fixation failure, leading many surgeons to treat these fractures as functionally displaced and recommend arthroplasty.29–31
For displaced FNFs, the choice between HA and THA is more nuanced. The HEALTH trial showed no difference in reoperation rates between THA and HA at 24 months, but small functional advantages for THA that did not exceed MCID.58 Mortality outcomes were equivalent, with 30-day rates of 7–10% in both groups.10,60 Registry data from Sweden and Norway confirm higher reoperation rates after HA due to acetabular erosion, but also higher early complication rates after THA, particularly dislocation and PPFF.20,46
Yu et al. in a meta-analysis reported that THA provides better hip function and quality of life compared with HA, albeit at the expense of longer operative times by approximately 20–30 minutes and greater intraoperative blood loss (p < 0.05) .71 Dislocation rates also remain higher following THA (2–5%) than HA (1–2%).61,71 Over the medium to long term, revision rates at 5–10 years tend to converge, as HA patients develop acetabular wear necessitating conversion to THA, while THA patients are predominantly revised for instability or PPFF.20,63
Economic analyses suggest that HA offers short-term cost savings, whereas THA becomes more cost-effective over time in active patients with a life expectancy exceeding five years.21,70 For medically vulnerable or low-demand patients, HA remains the more pragmatic option. Conversely, in highly active older adults, THA particularly with DM articulation provides the optimal balance between function, stability, and long-term value.58,65,70
Complications
Complications after treatment of FNFs remain a major determinant of both short- and long-term outcomes, with the spectrum of complications differing between IF, HA and THA.
Non-union and AVN are specific to fixation strategies. Non-union rates after IF vary between 20–45% in elderly displaced FNFs,48 while AVN occurs in 15–33% depending on fracture displacement and vascular compromise.72 These complications almost invariably necessitate revision to arthroplasty with the associated dire clinical and economic attrition conversion arthroplasty.
Dislocation is the hallmark complication of THA in fracture populations. Rates of 2–5% are consistently reported, compared with 1–2% for HA.61 Approach and implant selection influence risk, with the PA carrying a 2–3 times higher dislocation rate than anterior or lateral based approaches,63,64 while DM constructs have shown a 50% reduction in dislocation risk comparable to conventional THA designs.65–67
PPFF has emerged as a leading mode of THA failure in FNF. In a Mayo Clinic cohort of 217 fracture THAs, the 5-year cumulative incidence of PPFF was 7%, a dramatic increase on the <1% incidence observed in elective THA.63 This risk is particularly pronounced with uncemented stems, leading many guidelines to recommend cemented fixation in older adults.55,56
Infection risk is also greater in fracture populations, reflecting the emergency nature of surgery, higher patient frailty, and increased transfusion rates. The 5-year cumulative incidence of PJI after THA for FNF is reported at 3%, nearly double that of elective THA cohorts.63 Infection rates after HA are comparable at 1–2%.62
Perioperative morbidity extends beyond surgical complications and encompasses medical events such as thromboembolic disease, pneumonia, and delirium. Jameson et al. reported that venous thromboembolism occurs in 3–5% of patients despite appropriate prophylaxis,73 while Wang et al. found postoperative pneumonia in up to 10% of frail elderly individuals following hip fracture surgery.74 Marcantonio et al. similarly demonstrated that delirium affects 15–25% of patients, prolonging hospital stay and nearly doubling the risk of institutionalisation.41
Mortality remains the ultimate complication. Thirty-day mortality averages 7–10% across both HA and THA cohorts,10,60 while one-year mortality remains consistently high at 30–36%.10,70 The risk is greatest among patients with dementia, advanced frailty, or American Society of Anaesthesiologists (ASA) grade IV status.16,17
Functional Outcomes
Functional outcomes are the key differentiator between fixation, HA, and THA.
After IF, outcomes are highly variable. Patients with successful union can achieve excellent function, but up to one-third will require revision, which delays rehabilitation and diminishes long-term quality of life.45–48 Posterior tilt ≥20° predicts poorer function and higher rates of revision, emphasising the need for careful selection.29,30
HA provides reliable restoration of ambulation, but lower long-term function compared to THA. In the HEALTH trial, WOMAC scores at 24 months were higher in THA patients, although the differences did not exceed the MCID.58 EQ-5D and SF-12 scores showed similar trends, suggesting small quality-of-life advantages for THA.58
Registry data corroborate these findings with the Swedish registry PROMs consistently reporting higher satisfaction and functional scores after THA compared with HA.20 Conversion of HA to THA for acetabular erosion restores function but carries higher revision and complication rates than primary THA.75 (Figure 3)
Smith et al. directly compared outcomes between THA performed for FNFs and elective THA for OA, demonstrating that despite older age and greater frailty fracture patients can achieve nearly equivalent one-year functional results.18 In their 864-patient series, one-year Harris Hip Scores were 94.9 for FNF-THA versus 96.6 for OA-THA (p < 0.001), reinforcing the capacity of current arthroplasty practices to achieve near-normal function even in higher-risk fracture populations.
DM constructs further improve functional recovery by reducing dislocation risk, thereby avoiding instability-related revision that negatively impact PROMS.65–67 FJS are consistently higher with DM compared to conventional THA at early follow-up, reflecting greater stability and confidence in mobility.68
Special Populations
Patients with dementia
Individuals with dementia experience particularly poor outcomes. Olofsson et al. conducted a population-based study reporting a 180-day mortality of 31.8% after surgery compared with 45.7% in those managed non-operatively, confirming the survival benefit of surgical intervention even in cognitively impaired cohorts.16 Functional recovery, however, remains limited, and many patients require long-term institutional care postoperatively, as shown by Seitz et al.76
Younger patients (<60 years)
This group represents the opposite end of the spectrum. In these patients, preservation of the femoral head through IF remains the preferred approach, given the limited lifespan of arthroplasty implants. Although reoperation rates are high, long-term survivorship of the native hip often justifies the initial choice of fixation.52
Patients with severe osteoporosis
Those with advanced osteoporosis face increased risks of fixation failure and PPFF. For these patients, cemented stems are recommended during arthroplasty to enhance fixation stability and reduce fracture risk.55,56
Patients with inflammatory arthritis or immunosuppression
Individuals with inflammatory arthritis or chronic immunosuppression have a higher incidence of postoperative infection following arthroplasty. Registry data indicate infection rates approaching 5% in this subgroup, warranting aggressive perioperative optimisation and, in select cases, favouring HA to minimise operative time.77
HIV-positive patients
Particularly relevant in sub-Saharan Africa, HIV-positive individuals achieve comparable functional outcomes but demonstrate a slightly higher risk of early infection and revision after THA. These findings underscore the need for tailored antibiotic prophylaxis, vigilant postoperative surveillance, and multidisciplinary follow-up.78
Health Economics
The economic burden of FNFs is substantial, with costs driven by surgical intervention, hospital stay, rehabilitation and long-term institutional care.
In the UK, the mean initial inpatient costs are estimated at £6,394 for IF, £6,394 for HA, and £7,633 for THA.21 However, IF is associated with substantially higher reoperation rates, leading to significantly greater long-term expenditure (p < 0.01)46,47 Notably, conversion arthroplasty following failed IF has been shown to cost up to three times more than primary arthroplasty.79
Cost-effectiveness analyses favour THA in active patients with life expectancy >5 years, as functional gains and lower long-term revision rates offset higher upfront costs.21,70 In lower demand patients with limited life expectancy, HA remains more cost-effective due to lower perioperative resource use and reduced operative complexity.21
Globally, the financial impact is immense. In the USA, hip fracture-related hospitalisations exceed $20 billion annually, with projections suggesting a worldwide burden of $131 billion by 2050 if incidence trends persist.22 Implementation of enhanced recovery and fracture liaison services has been shown to reduce readmissions and downstream costs by 10–15%.80
Future Directions
Research continues to refine treatment strategies for FNFs. Several ongoing randomised trials are comparing DM versus conventional THA specifically in fracture populations to provide higher-level evidence for dislocation prevention.81 Further investigation into the role of cementless fixation in select patients is also underway, although current data strongly favour cemented stems in the elderly.55,56
Technological advances, including robotic-assisted arthroplasty, may improve implant positioning accuracy in FNF patients, however evidence remains limited to elective cohorts.82 Biologic augmentation of IF, including stem cell grafts and bone morphogenetic proteins (BMP), has shown promise in preclinical studies but lacks robust clinical validation.51
Global initiatives are focusing on prevention through osteoporosis screening, fall reduction programmes, and optimisation of frail elderly pathways. The International Fragility Fracture Network has emphasised the need for universal hip fracture registries to benchmark care and outcomes across countries.83
Conclusion
FNFs remain a global health challenge, associated with a high mortality, morbidity, and economic burden. IF retains a role in younger patients and undisplaced fractures, but failure rates in the elderly are unacceptably high, particularly when posterior tilt exceeds 20°. Hemiarthroplasty provides reliable pain relief and ambulation for frailer populations, with cemented stems demonstrating clear superiority. THA offers superior functional outcomes in active older adults but carries higher risks of dislocation, PPFF, and PJI. DM constructs mitigate instability and are increasingly favoured in high-risk populations.
Despite improvements, outcomes remain poor for cognitively impaired and frail populations, and one-year mortality continues to approach one-third of all patients. The economic impact is staggering and will rise with the ageing population. Future strategies should integrate surgical advances with system-level interventions in fracture prevention, rapid optimisation, early surgery, and multidisciplinary rehabilitation. Only through combined surgical innovation and holistic care can outcomes for this vulnerable population be substantially improved.