




INTRODUCTION
Hallux valgus is a common foot deformity with a high global prevalence, especially among women and the elderly. A recent meta-analysis reported a combined prevalence of approximately 19% in the general population.1 This prevalence is higher in women (≈23.7%) than in men (≈11.4%), and increases with age.2 Other systematic data show a prevalence of ~23% in adults (18–65 years) and ~36% in the elderly (>65 years). Hallux valgus is a significant contributor to clinical burden; in addition to causing bunions and difficulty wearing shoes, this deformity is associated with foot pain, gait disturbances, and risk of falls in the elderly.1 This condition often reduces quality of life, incurs high treatment costs, and causes functional difficulties in daily activities.2
The pathophysiology of hallux valgus is complex and multifactorial. This deformity is characterized by lateral deviation of the proximal phalanx and medial deviation of the first metatarsal head (metatarsus primus varus).3 Muscle force imbalance and foot ligament structure are major factors; for example, tension in the peroneus longus (lateral) and abductor hallucis (medial) muscles normally stabilize the first metatarsal, but high pressure on the first metatarsal head shifts the metatarsal medially and the hallux laterally.3 As a result, the medial MTP I capsule is stretched to the point of rupture, while the lateral structures (adductor hallucis muscle and collateral ligament) exacerbate the deformity.
These biomechanical changes cause the distribution of foot load to shift to the heads of the second to fifth metatarsals (metatarsalgia transfer) and cause deformities in other toes (e.g., hammer toes) and reduce the dorsiflexion function of the big toe.4 Radiologically, hallux valgus is diagnosed if the hallux valgus angle (HVA) exceeds 15° and the intermetatarsal angle (IMA) is greater than normal (±9°),4 often accompanied by hallux pronation and spasm, which affects gait stability and comfort.
Management of hallux valgus ranges from conservative to surgical depending on the degree of deformity and symptoms. For cases requiring surgery, first metatarsal osteotomy is the central procedure. This osteotomy can be performed at three main locations: at the metatarsal base (proximal osteotomy), the metatarsal shaft (e.g., Scarf osteotomy at the diaphysis), or the metatarsal neck (distal osteotomy).3 The most commonly used techniques are distal osteotomy (e.g., Chevron/Austin osteotomy) for mild to moderate cases, and proximal osteotomy (e.g., Mau or Ludloff osteotomy) for correction of large IMA angles and severe cases. Each technique has its own characteristics. For example, the popular distal Chevron osteotomy is reliable with minimal soft tissue trauma, but is not suitable for severe deformities and carries a risk of reducing blood flow to the metatarsal head.4
The advantages of distal osteotomy include faster healing and generally good bone union, while the disadvantages are limited IMA angle correction and the possibility of metatarsal shortening. Conversely, proximal osteotomy allows for greater IMA correction and more significant rotational realignment, but requires a larger incision, complex stabilization, and potential complications such as non-union and joint stiffness. Opening-wedge techniques at the base, for example, can widen the IMA without removing bone, but require implant support or bone grafting and carry a higher risk of non-union. In general, the indication for osteotomy is determined by the degree of deformity: distal osteotomy is preferred for mild to moderate HV (HVA < 30°, IMA < 13–15°), while proximal osteotomy is recommended for moderate to severe cases (HVA > 25–30°, IMA > 13°).3,4
Several clinical studies have compared the outcomes of distal versus proximal osteotomy. In a meta-analysis by Tsikopoulos et al. (2018) involving ~696 moderate to severe cases, no significant differences were found in clinical outcomes (e.g., AOFAS scores, HVA correction angle) between the proximal osteotomy (PMO) and distal osteotomy (DMO) groups.5 Only IMA angle correction was slightly better in the PMO group, but there were no significant differences in functional scores or patient satisfaction.5 Similar results were concluded by several RCTs: a small number showed equivalence of outcomes between the chevron (distal) technique and the proximal technique in mild-to-moderate deformities, although one RCT stated that proximal osteotomy was superior in certain corrections.6 Overall, the existing evidence remains limited and contradictory.5
Several recent meta-reviews emphasize that for mild to moderate deformities, distal techniques (e.g., Chevron or Scarf) provide radiological and clinical correction equivalent to proximal osteotomy.5,6 Given the variety of techniques and heterogeneous results, there is a need to comprehensively analyze the clinical performance of each technique. Previous studies were generally small-scale or did not directly compare each method, and existing meta-analyses show equivalent results between distal and proximal osteotomies but are still influenced by bias and study heterogeneity.5
Therefore, a systematic review and meta-analysis synthesizing the latest primary data is needed to assess the clinical performance (angle correction, foot function, complications, recurrence) of distal versus proximal first metatarsal osteotomy in the correction of hallux valgus. This research gap is important for providing evidence- based recommendations on the selection of the optimal technique based on the degree of deformity and clinical factors, thereby improving the quality of care for HV patients.5,6
METHODS
Research Methods
This study is a systematic review and meta-analysis conducted in accordance with the PRISMA 2020 guidelines. The main objective is to compare the clinical performance of distal osteotomy and proximal osteotomy of the first metatarsal in patients with hallux valgus.
Search Strategy
The search was conducted on November 19, 2025, in the Google Scholar, PubMed, and Scopus databases. The search used a combination of keywords based on PICO: (“hallux valgus” OR “bunion”) AND (“first metatarsal osteotomy” OR “distal osteotomy” OR “proximal osteotomy” OR “chevron” OR “scarf”) AND (“pain” OR “VAS” OR ‘AOFAS’ OR “recurrence” OR “MTP1 angle” OR “HVA” OR “MCA” OR “DMAA” OR “intermetatarsal angle” OR “IMA” OR “early weight bearing” OR “union” OR “union rate” OR “union time” OR “nonunion” OR “malunion” OR “infection”) for articles published between 2015 and 2025. Only human studies and English-language articles were included.
Inclusion and Exclusion Criteria
The studies included in this review were comparative clinical studies, both prospective and retrospective, including cohort studies and randomized controlled trials (RCTs), which compared distal first metatarsal osteotomy with proximal first metatarsal osteotomy in patients with hallux valgus. The study population included adult patients aged ≥18 years with hallux valgus deformity, without restrictions on gender or specific etiology. The interventions analyzed included various distal osteotomy techniques such as distal chevron, scarf, or percutaneous osteotomy, compared with proximal osteotomy techniques such as proximal chevron, closing wedge, or opening wedge osteotomy.
The primary outcomes evaluated included pain (measured using the VAS scale or AOFAS score), hallux valgus recurrence (MTP1 angle), radiological correction (MCA1 angle and intermetatarsal angle 1–2), foot function (bearing capacity or early mobilization), and bone union outcomes (union rate or union time). Complications such as non-union, malunion, and infection were also included as parameters for analysis. All included articles were published between 2015 and 2025, were available in full text, and were written in English.
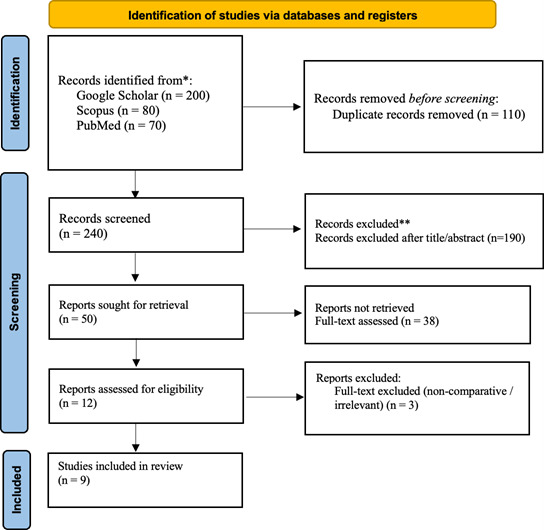
Studies excluded from this review included non-comparative studies, single case reports, editorials, commentaries, or non-systematic review articles. Studies involving pediatric populations (<18 years), animal models, or cadavers were also excluded. Additionally, articles that did not present at least one of the predefined primary outcomes, or that used combined interventions that did not allow for the specific isolation of the effects of distal or proximal osteotomy, were not included. Articles that were not available in full text, had unclear methods, or incomplete data, as well as those published in languages other than English, were also excluded from this review. These inclusion and exclusion criteria were applied to ensure the validity and relevance of the results in evaluating the clinical effectiveness of both osteotomy techniques in the management of hallux valgus (Figure 1).
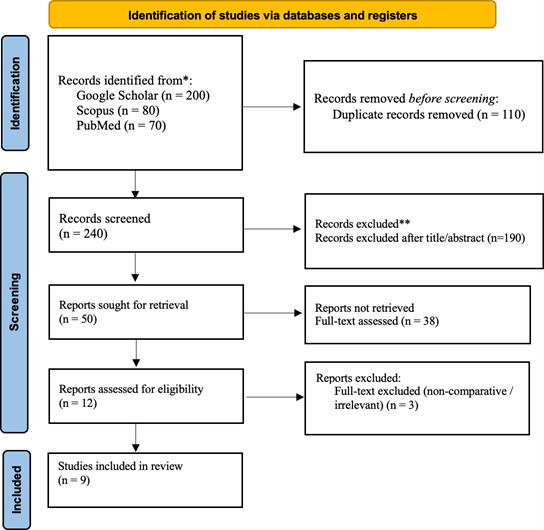
Study Selection Process
Article selection was conducted in three stages. First, the identification stage involved collecting all articles from various databases and then removing duplicates. Second, the screening stage involved reviewing titles and abstracts to assess their relevance to the research topic. Third, the eligibility assessment stage involves reviewing the full text to ensure relevance to the established inclusion criteria. The entire selection process is carried out independently by researchers. Differences in selection results are resolved through discussion to ensure the accuracy of study selection.
Literature Search Results
The initial search yielded nine relevant articles. After screening the titles, abstracts, and full texts, all articles met the inclusion criteria and were included in the final analysis.
RESULTS
Study Selection Process
The literature search was conducted using various electronic databases, including Google Scholar, Scopus, and PubMed. The initial search yielded a total of 350 articles. After initial screening to eliminate duplicates, 240 unique articles remained for further review. The selection stage based on titles and abstracts resulted in the exclusion of 190 articles that were not relevant to the research focus, such as those discussing private insurance claims or unrelated to government hospitals. Thus, 50 articles entered the full-text review stage. At the full-text review stage, 38 articles were excluded because they did not meet the inclusion criteria, including opinions or editorials, reports without empirical data, or articles that were not accessible in full text. A total of 9 articles were found to meet all inclusion criteria and were included in the final analysis of this literature review.
Study Characteristics
The results in Table 1 show that nine studies that met the inclusion criteria were published between 2015 and 2025. The study designs used varied. There were prospective cohorts, retrospective cohorts, systematic reviews, and meta-analyses comparing various metatarsal osteotomy techniques. One study used a randomized clinical trial with long-term follow-up to evaluate the differences in outcomes between the distal osteotomy technique and alternative techniques.
The sample size in each study ranged from 43 to more than 700 cases in the systematic review. Most studies examined adult patients with moderate to severe hallux valgus. The interventions compared included distal chevron osteotomy, proximal chevron osteotomy, scarf osteotomy, lapidus procedure, and variations of minimally invasive techniques. Several studies assessed direct comparisons between distal and proximal osteotomies. Other studies grouped different osteotomy locations to examine the effect of bone cut location on correction angle and clinical outcomes.
Follow-up duration varied between 6 and 24 months in most clinical studies. One study had a follow-up of up to 14 years. All studies reported radiological results. The majority also reported functional scores and complication rates. These results provide a comprehensive overview of the performance differences between distal and proximal techniques in hallux valgus correction (Table 1).
Effectiveness, Outcome (Pain & Function), Fusion/Recovery, and Complications
Table 2 shows that of the nine journals analyzed, each discusses the comparison of distal and proximal first metatarsal osteotomy in hallux valgus patients. The main focus is on surgical techniques, radiological correction (HVA, IMA, MCA/DMAA), pain and function (VAS/AOFAS, early weight bearing), bone union rate and time, and complications (non-union, malunion, infection). In general, both techniques are effective in reducing pain and improving the angle of deformity. Proximal osteotomy tends to provide greater angular correction in severe deformities. Distal osteotomy offers faster functional recovery and different complications depending on technical modifications. Variations in outcomes are primarily related to the severity of the deformity, surgical technique, and duration of follow-up.
VAS
Conclusion: 0.03 [95% CI: −0.33 to 0.39], with I² = 6.8%, indicates that the combined effect of the two studies is very small and shows no difference in VAS between groups. The confidence interval crossing zero indicates no significant difference, and the low I² value indicates minimal variation between studies, so the results of both studies remain stable (Table 3).

AOFAS
Conclusion: 0.06 [95% CI: −0.28 to 0.39], with I² = 0%, indicates that the combined effect of the two studies is very small and does not show a significant difference between the distal and proximal groups. The confidence interval crossing zero indicates no statistical difference, and the I² value of zero indicates no heterogeneity, meaning that the results of the two studies are consistent and stable (Table 4).

HVA
Conclusion: 0.14 [95% CI: −0.86 to 1.15], with I² = 87.3%, indicates that the combined effect of the two studies shows no significant difference between the distal and proximal groups. The very wide confidence interval that crosses zero indicates no clear effect, and the high I² value indicates substantial heterogeneity, meaning that the results of the two studies are inconsistent and the findings between studies are unstable (Table 5).

IMA
The combined effect showed an SMD of 0.51 (95% CI –0.19 to 1.21) with high heterogeneity (I² = 73.4%), indicating no significant difference between distal and proximal osteotomy in IMA correction based on the two studies (Table 6).

DMAA
The results showed an SMD of –0.72 (95% CI –1.30 to –0.13), indicating that distal osteotomy provides better DMAA correction than proximal osteotomy. Since there was only one study, heterogeneity could not be calculated (Table 7).

Primary Outcome: Function and Pain
Based on various studies reviewed, all osteotomy techniques, whether distal, proximal, Scarf, Chevron, Lapidus, or minimally invasive (MIS), consistently show significant improvement in pain and postoperative function. Almost all studies report a significant reduction in pain, usually indicated by a decrease in VAS scores, as well as improved leg function as reflected by increased AOFAS scores or other function scales.
In both distal and proximal techniques, Lee KB et al. noted that both approaches provided relatively equivalent improvements in pain and function.7 The MIS study (Choi JY et al.) also noted good pain reduction and functional improvement, indicating that the minimally invasive approach still provides strong clinical benefits despite some technical challenges.8 Meta-analyses and systematic reviews, such as those by Tsikopoulos and Zipagan, reinforce these findings, namely that improvements in function and reductions in pain occur consistently across techniques without significant differences between methods.5,9
In long-term studies (Jeuken and Thomas), improvements in function and reductions in pain were found to be stable over longer follow-up periods, indicating the sustainability of the benefits of the techniques used.10,11 Even with specific techniques such as Lapidus or Scarf, despite each having unique characteristics in angle correction, clinical outcomes related to pain and function still showed a similar trend of improvement.
Overall, the available evidence indicates that pain and function improvement are the most consistent and stable outcomes across all variations of osteotomy techniques, with very few reports showing a clinical advantage of one technique over another for these outcomes.
Secondary Outcomes: Angle and Complications
Correction of deformity angles is one of the main focuses in evaluating the results of various osteotomy techniques. Almost all studies report improvements in radiological parameters such as HVA, IMA, and in some studies also DMAA. Both distal and proximal techniques studied by Lee KB et al.7 show similar angle corrections. These results are consistent with the findings of Choi JY et al. on minimally invasive techniques, which also provided improvements in HVA, IMA, and DMAA with relatively comparable results between groups.8 A systematic review by Tsikopoulos and a report by Zipagan confirm that angle correction does occur in all techniques, although the extent may vary between studies due to variations in methods, indications, and procedural modifications.9
Some techniques have specific characteristics in angle correction. Lapidus, as described by Yammine,12 offers stronger IMA correction, especially in cases with tarsometatarsal instability, while Scarf can provide better HVA correction in certain contexts, as reported by Brodén.13 However, overall, there is no consistent pattern showing the absolute superiority of one technique in angle correction in all patient groups.
Regarding complications, most studies report low complication rates and no significant differences between the techniques compared. Lee KB et al.7 stated that complications were relatively few and did not show significant differences. Similar findings were seen in Tsikopoulos’ study,5 which noted no significant differences in the incidence of infection or non-union. In minimally invasive techniques, Choi JY et al.8 found some technical problems related to the operator’s learning curve. The Lapidus technique has the potential for fusion complications, as reported by Yammine.12 However, in long-term studies such as Jeuken and Thomas, chronic complications are relatively rare and recurrence rates are low.10,11
Overall, the correction of osteotomy angles showed a consistent pattern of improvement, although the magnitude varied between techniques. The complication profile remained at an acceptable level and did not show significant differences between most of the methods used.
Synthesis of Results
A synthesis of the results from 9 journals shows that all osteotomy techniques provide consistent improvement in pain and function, with no clinically significant differences between techniques. Angular correction was also achieved in all procedures, although the extent of correction varied according to patient characteristics and the surgical approach used. Reported complications were generally low and did not show significant differences between techniques. Overall, the evidence from these 9 journals indicates that each technique is effective and safe, so the choice of procedure should be tailored to clinical indications and the operator’s experience.
DISCUSSION
Overall Effectiveness and Interpretation of Findings
Nine studies show that both techniques, distal and proximal first metatarsal osteotomy, provide consistent clinical improvement in patients with hallux valgus. All studies report a reduction in pain, improved function, and significant angle correction after surgery. No technique has been proven to be superior for all conditions. The best outcomes are achieved when the technique is selected based on the degree of deformity. Distal osteotomy is suitable for mild to moderate deformities. Proximal osteotomy is more appropriate for severe deformities or when IMA correction and medial stabilization are required.14,15 A comprehensive analysis of the nine studies confirms that effectiveness depends on selecting the technique appropriate to the patient’s characteristics, not on the technique itself.
Outcome (Pain)
All studies show a clear reduction in pain after surgery. VAS scores dropped from a range of 7 to around 2. The differences between techniques were small and not clinically significant. Several studies using MIS techniques reported faster pain reduction in the early phase, but long-term results remained comparable. Data from Lee, Choi, Jeuken, and Yammine show that both techniques provide good pain control.7,8,12 The practical message is that patients can expect significant pain reduction regardless of the technique used.
Outcome (Function)
AOFAS scores improved in all studies. The range of improvement was between 25 and 35 points. No technique showed a significant advantage in improving function. Studies by Fukushi, Zipagan, and Yammine showed similar patterns of improvement.6,9,12 Factors that more strongly influenced function were the degree of initial deformity, medial structural stability, and rehabilitation compliance. Findings were consistent that both techniques provided good and stable functional results.
Angle
Angular correction occurred throughout the study. Proximal osteotomy showed greater HVA and IMA correction in patients with severe deformities. Zipagan and Thomas reported better IMA correction with the proximal technique due to stronger medial column control.9,11 Distal osteotomies such as chevron and scarf provide adequate correction for mild to moderate deformities. Some studies show that scarf provides slightly better HVA correction than chevron. Choi and Fukushi noted that changes in DMAA and MCA depend on the technique and its modifications.6,8 Technique selection should follow preoperative HVA and IMA values to achieve optimal correction results.
Complications
Low complication rates in most studies. The difference between distal and proximal osteotomies is small and not significant. Proximal osteotomy has a slightly higher risk of non-union due to the larger nature of the procedure. Distal osteotomy is more commonly associated with metatarsalgia transfer or hardware irritation. Findings from Lee, Fukushi, Thomas, and Yammine show a consistent pattern that complications can be controlled with good surgical technique and appropriate rehabilitation protocols.6,7,11,12 Practically, physicians need to assess the risk profile based on deformity and correction needs before selecting a technique.
Research Gap and Recommendations
Most studies only assess radiographic results and short-term functional scores. Few studies assess quality of life, long-term functional burden, or patient satisfaction with standard instruments. No studies have assessed the cost effectiveness between distal and proximal procedures. The choice of technique still depends heavily on the operator’s preference. Some studies use small samples and do not perform robust subgroup analyses, especially for severe deformities. Research on minimally invasive techniques shows promising initial results, but long-term data is insufficient to draw conclusions. There is considerable variation in surgical techniques. Distal and proximal techniques have many modifications, making it difficult to determine which technique is most effective for various degrees of deformity.
Conclusion
Distal and proximal first metatarsal osteotomy techniques are equally effective in improving pain, function, angle deformity, and providing low complication rates.
Pain and function improvement appeared consistently across all studies. The HVA and IMA angles improved significantly with both techniques. Distal osteotomy tends to provide faster recovery, while proximal osteotomy provides greater angle correction in moderate to severe deformities. There were no significant differences in complications between the two approaches. The choice of technique is more appropriate when tailored to the degree of deformity, correction needs, and the operator’s experience.
Author Contribution
Rudiansyah Harahap conceptualized the study, developed the methodology, performed statistical analysis, and drafted the manuscript. Pamudji Utomo conducted the literature search, performed study screening, extracted data, and contributed to manuscript revision. Paramasari Dirgahayu assisted in literature search, data extraction and verification, and reviewed and edited the manuscript. Eti Poncorini provided supervision, critically reviewed the methodology and results, and approved the final manuscript. Dono Indarto provided supervision, critically reviewed and edited the manuscript. Rieva Ermawan provided assist in correcting and reviewed the manuscript. Ratih Dewi Yudhani performed extraction data, reviewed and edited the manuscript.