1. Introduction
Tibial avulsion fractures of the ACL account for approximately 14% of all ACL injuries.1 In contrast, tibial avulsion fractures of the posterior cruciate ligament (PCL) are relatively uncommon. Both injury patterns may result in knee instability and predispose patients to early degenerative changes if not appropriately treated.2
Simultaneous ACL and PCL tibial avulsion fractures in a single knee represent an exceptionally rare injury pattern, most often resulting from high-energy trauma. Only a limited number of cases have been reported in the literature and no consensus has been established regarding the optimal surgical strategy.3–5
This report presents a case of simultaneous tibial avulsion fractures of both cruciate ligaments treated with an all-arthroscopic suture fixation technique combined with a posterior trans-septal approach to enhance visualization of the posterior compartment and facilitate anatomic reduction of the PCL footprint. At 6 months postoperatively, the patient demonstrated excellent radiologic healing and functional recovery
2. Case Presentation
Informed consent
Written informed consent was obtained from the patient for publication of this case report and the accompanying images in accordance with ethical standards.
2.1. Patient information
A 33-year-old woman, previously healthy and without any prior history of knee trauma or pre-existing joint disease, presented with right knee pain and swelling 8 days after a motor vehicle accident. Before presentation to our institution, she had been managed conservatively with rest and analgesics only, without immobilization or invasive intervention.
2.2. Clinical findings and imagings
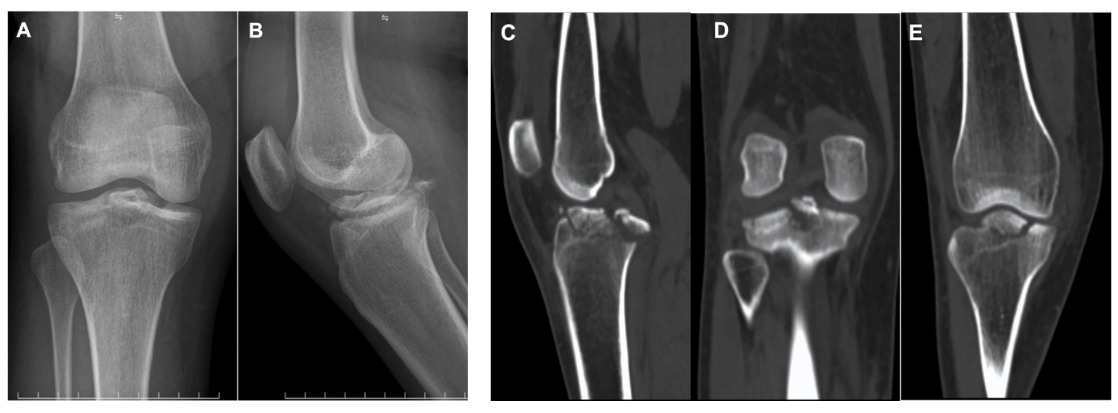
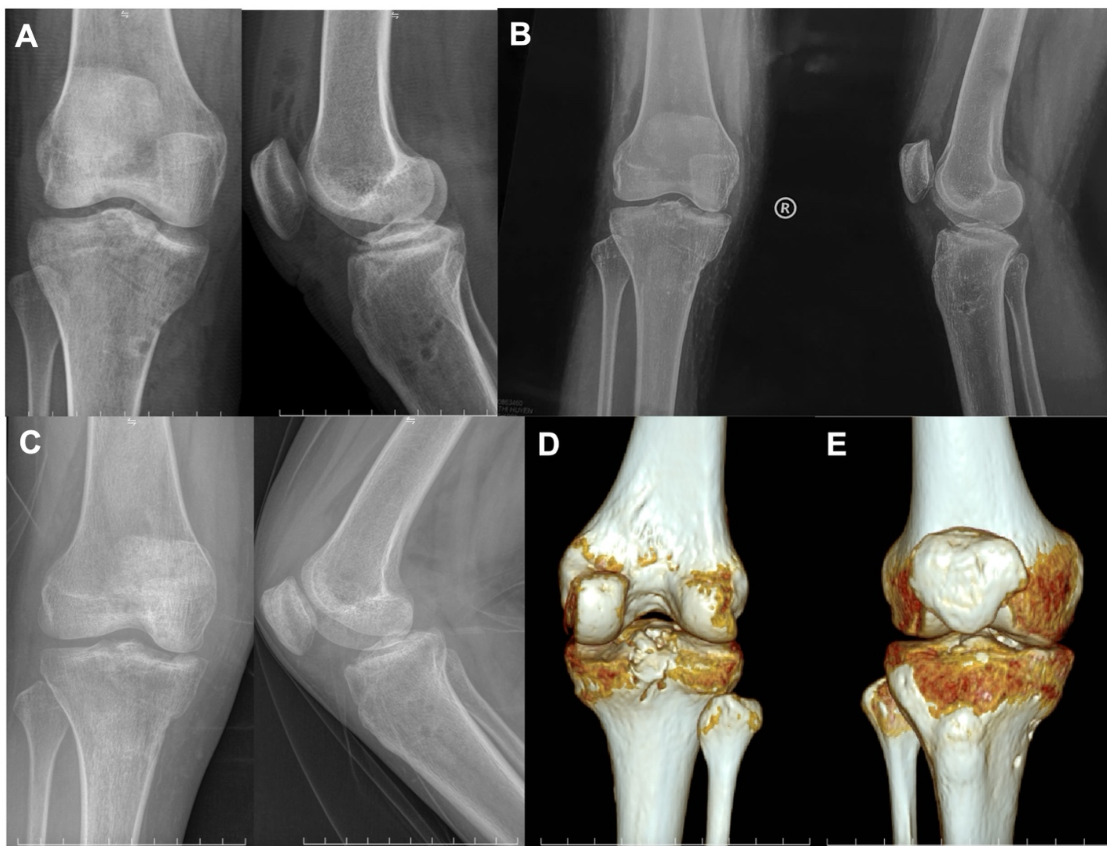
On examination, the right knee demonstrated mild swelling and restricted ROM due to pain. The Lachman’s test and anterior–posterior drawer tests were positive, indicating combined cruciate ligament instability. No associated neurovascular compromise was detected. Radiographic and CT evaluation confirmed completely displaced simultaneous tibial avulsion fractures of the ACL and PCL, with no associated tibial plateau fracture or additional osseous injury (Figure 1). Based on the clinical and radiologic findings, a diagnosis of completely displaced simultaneous ACL and PCL tibial avulsion fractures was established.

2.3. Operative procedure
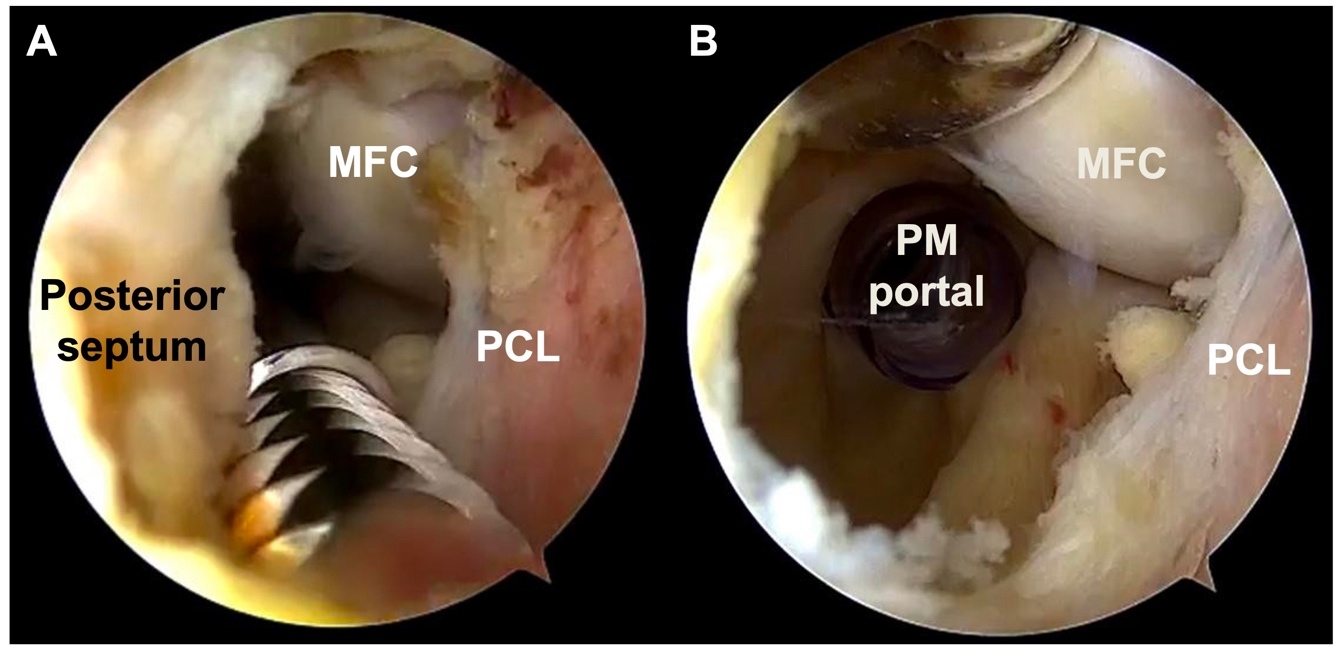
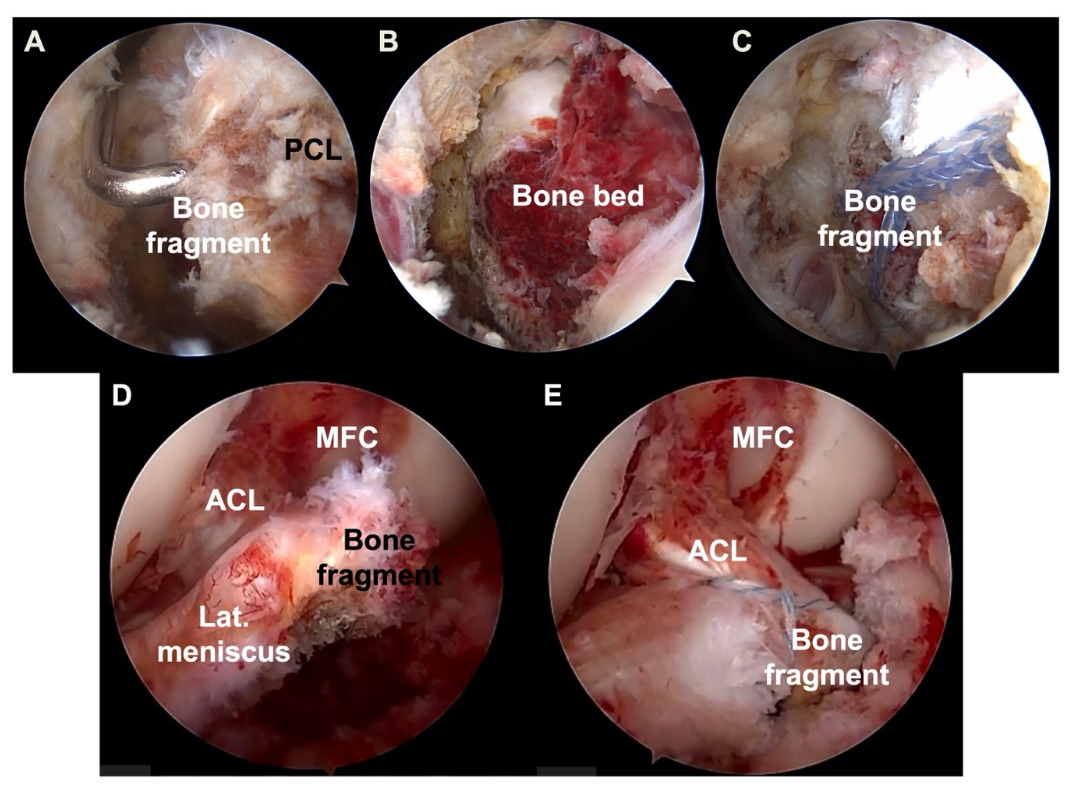
Arthroscopic surgery was performed under spinal anesthesia with the patient in the supine position and a thigh tourniquet applied. Standard anterolateral (AL) and anteromedial (AM) portals were established for initial diagnostic arthroscopy. Intra-articular evaluation confirmed displaced tibial avulsion fractures of both the ACL and PCL. For fixation of the PCL tibial avulsion, FiberTape® (Arthrex, Naples, FL, USA), an ultrahigh-strength 2-mm-wide tape incorporating the FiberWire® structure, was used in combination with a SwiveLock® anchor (Arthrex, Naples, FL, USA). Posteromedial (PM) and posterolateral (PL) portals were created, followed by establishment of a posterior trans-septal portal (Fig 2) to allow direct visualization of the posterior compartment and the PCL tibial footprint (Fig 3A). Hematoma and interposed fibrous tissue were debrided, and the bone bed was prepared to facilitate anatomic reduction (Fig 3B).


Through the AM portal, a grasper was utilized to pass both limbs of the FiberTape along the medial and lateral margins of the PCL.The sutures were retrieved through the PM and PL portals, effectively looping around the PCL root from anterior to posterior. With visualization from the PL portal, a tibial tunnel locator for PCL reconstruction (Smith & Nephew, Andover, MA, USA) was introduced through the PM portal. Two 2.4-mm transtibial tunnels were sequentially drilled from the medial aspect of the proximal tibia to the medial and lateral margins of the bone bed, approximately 2–3 mm distal to the fragment edge. Shuttle sutures were then passed through each tunnel to retrieve the FiberTape limbs from the posteromedial and posterolateral portals, respectively. The sutures were crossed anterior to the avulsed fragment in a figure-of-eight configuration (Fig 3C). An anterior drawer force was applied to achieve anatomic reduction of the PCL avulsion fragment. The FiberTape limbs were tensioned and secured over the tibial bone bridge, with supplemental fixation achieved using a SwiveLock® anchor.
For fixation of the ACL tibial avulsion, high-strength sutures (Smith & Nephew, Andover, MA, USA) were utilized. Following meticulous preparation of the bone bed (Fig 3D), a 45° angled suture hook (Smith & Nephew, Andover, MA, USA) was introduced through the AM portal and used to penetrate the ACL near its tibial insertion. A shuttle suture was passed through the ligament base and exchanged for high-strength sutures to secure the avulsed fragment. A tibial tunnel locator for ACL reconstruction (Smith & Nephew, Andover, MA, USA) was used to create two 2.4-mm transtibial tunnels from the anteromedial aspect of the proximal tibia to the anteromedial and anterolateral margins of the fracture bed, ensuring that these tunnels did not converge with the previously created tunnels. Shuttle sutures were sequentially passed through each tunnel into the joint to retrieve the high-strength suture limbs from the ACL base. The sutures were crossed anterior to the avulsed fragment in a figure-of-eight configuration (Fig 3E). Anatomic reduction was achieved, and the sutures were tensioned and tied securely over the anterior tibial cortex with the knee positioned at 20°–30° of flexion.
Postoperatively, the knee was immobilized in a cast for 4 weeks. Following cast removal, a supervised rehabilitation protocol was commenced, emphasizing progressive ROM recovery and strengthening of the quadriceps and surrounding musculature.
2.4. Follow up
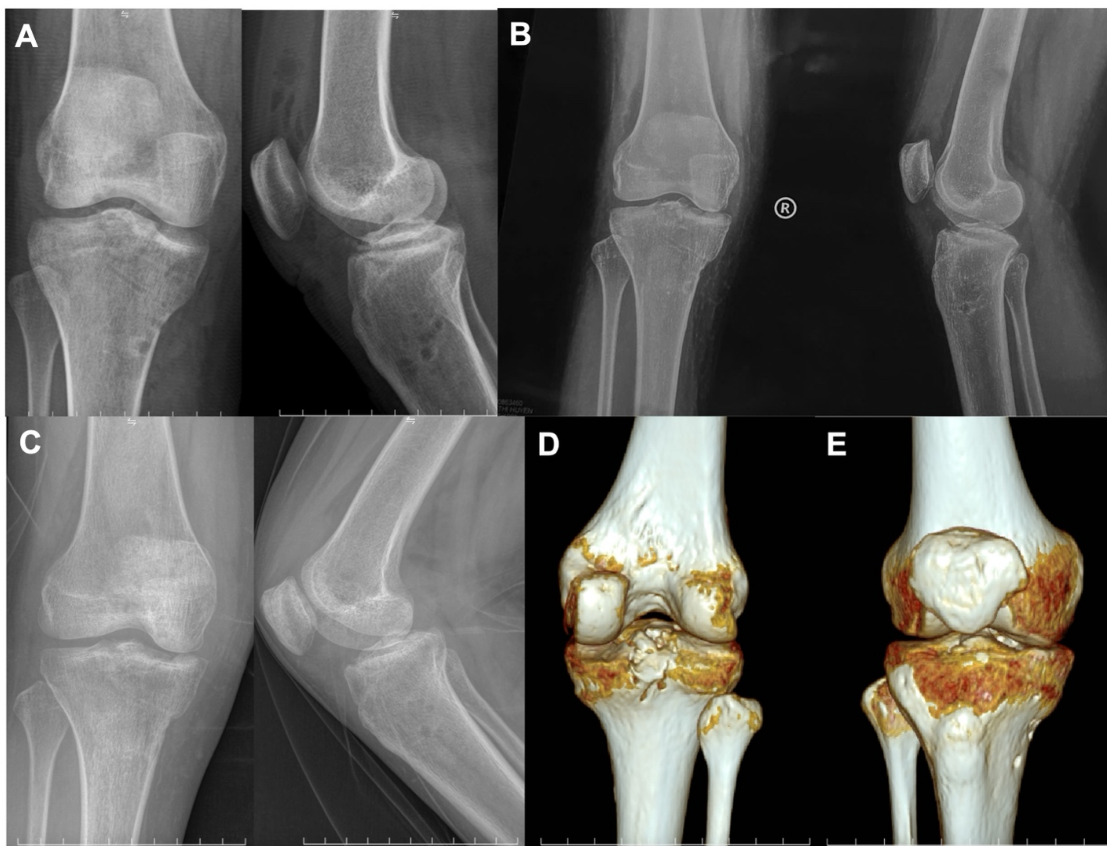
Immediate postoperative radiographs demonstrated anatomic reduction of the avulsed fragments (Fig 4A). Follow-up imaging at 1 month confirmed maintenance of stable fixation (Fig 4B). Radiographs and CT at 3 months revealed complete osseous union with preservation of anatomic alignment (Fig 4C, D, E). At 6 months postoperatively, the patient achieved a knee range of motion from 0° to 150°, with negative Lachman’s test and anterior–posterior drawer tests. Functional evaluation demonstrated an objective IKDC grade A, a subjective IKDC score of 100, and a Lysholm score of 100. The patient returned to normal daily activities without pain or residual instability.
3. Discussion
Simultaneous tibial avulsion fractures of both cruciate ligaments in adults represent a rare injury pattern. Although isolated ACL or PCL avulsion fractures are well documented,6,7 combined involvement of both ligamentous attachments has been reported only in a limited number of cases (Table 1).3–5,8–12
Regarding the mechanism of injury, most reported cases in the literature are associated with high-energy trauma, including motor vehicle accidents or falls from height.3–5,11,12 A combined hyperextension force with anterior–posterior shear stress is believed to contribute to simultaneous avulsion of both cruciate ligament attachments.13,14 The mechanism in our patient aligns with those previously reported.
The choice of fixation method for tibial avulsion fractures remains controversial, with options including cannulated screw fixation and transosseous high-strength suture fixation.15,16 Screw fixation is generally preferred for large, intact bony fragments. In contrast, transosseous high-strength suture fixation allow more force distribution and are particularly advantageous for smaller or comminuted fragments, while avoiding the need for hardware removal.16 In the present case, the ACL avulsion was fixed using high-strength sutures alone, consistent with previously reported techniques.4,5,8,12 For the PCL avulsion, a 2-mm high-strength suture tape was selected instead of conventional round sutures. The broader tape configuration helps reduce the risk of fragment cut-through, increases the contact surface area, and enhances compressive force across the fracture bed. Additionally, after tying the sutures over the tibial cortex, supplemental fixation with a SwiveLock® anchor was applied as a secondary reinforcement to minimize suture elasticity and further stabilize the construct.
Due to the rarity of this injury pattern, no standardized surgical algorithm has been established. The reported techniques can be grouped into several major categories.
First, open reduction has been employed in certain cases, particularly in earlier reports when arthroscopic techniques were less developed, in complex injury patterns, or in the presence of large fracture fragments. Surgical exposure was typically achieved through a medial parapatellar approach or via the Burks approach to access the PCL tibial avulsion fragment.9–11 Second, a combined approach has been described, consisting of arthroscopic ACL fixation through standard anterior portals and open posterior PCL fixation, typically using the Burks approach. This strategy frequently requires intraoperative patient repositioning.5,12 Third, all-arthroscopic approaches utilizing standard anterior portals, supplemented by accessory medial or central portal when necessary, have been described. Fixation constructs in these reports have included transosseous sutures, suture anchors, and cortical button suspension systems.4,8 Finally, some authors have described an arthroscopic approach using standard anterior portals combined with posteromedial portals to directly access the posterior compartment. This approach facilitates direct visualization of the PCL tibial insertion, allowing precise reduction and stable fixation entirely arthroscopically, thereby avoiding posterior open exposure.
While the benefits of arthroscopic fixation for cruciate ligament avulsion fractures have been well documented, the technique applied in our case presents several distinct technical refinements.
First, we utilized a posterior trans-septal (TS) technique with both posteromedial and posterolateral portals, combined with posterior septum resection to establish communication between the two posterior compartments. This approach enables comprehensive visualization of the posterior knee compartment and significantly improves access to the PCL tibial footprint, allowing controlled reduction and accurate fixation that would be technically challenging through anterior portals alone. These advantages have been highlighted in previous reports.17 In addition, the all-arthroscopic technique may shorten operative time by avoiding intraoperative repositioning of the patient.
Second, fixation of the PCL avulsion was prioritized before addressing the ACL. From a biomechanical standpoint, in PCL tibial avulsion fractures, the bony fragment is typically displaced superiorly and anteriorly, while the tibial plateau tends to translate posteriorly relative to the femoral condyle.18 Therefore, reduction of the PCL avulsion fragment requires restoration of anterior tibial translation to counteract posterior sagging of the tibia. During PCL fixation, a maximal anterior drawer maneuver was applied to translate the tibia anteriorly and achieve anatomic reduction. Delaying ACL fixation at this stage permitted unrestricted anterior tibial translation, thereby facilitating precise reduction and stable fixation of the PCL avulsed fragment.
Finally, during ACL fixation, particular care must be taken to avoid interposition of the meniscofemoral ligament or the anterior horn of the medial meniscus within the bone bed. Entrapment of these structures may compromise fracture healing and lead to persistent postoperative knee pain if not promptly recognized and addressed.19
Postoperatively, the patient achieved complete osseous union on CT at 3 months and demonstrated excellent functional recovery at 6 months, with an objective IKDC grade A, a subjective IKDC score of 100, and a Lysholm score of 100. These outcomes are comparable to those reported in previous cases of similar injury patterns.3–5 These findings suggest that, when anatomic reduction and stable fixation are achieved, simultaneous arthroscopic fixation of both cruciate ligament avulsion fragments can result in optimal functional recovery.
4. Conclusion
Simultaneous tibial avulsion fractures of both cruciate ligaments in adults represent a rare injury pattern and may result in significant knee instability if not appropriately managed. Accurate diagnosis based on thorough clinical examination combined with appropriate imaging studies is essential for optimal treatment planning. Our case demonstrates that an all-arthroscopic approach incorporating a posterior trans-septal technique and figure-of-eight suture fixation can achieve anatomic reduction and excellent functional recovery. This report contributes additional clinical experience to guide surgical decision-making in managing this uncommon injury.
Acknowledgments
None.
Authors’ Contributions
Dr. Dung Nguyen Quoc: Conceptualization, Writing - Review & Editing, Supervision.
Dr. Thuan Mai Duc: Conceptualization, Writing - Review & Editing, Supervision.
Dr. Trung Do Duc: Surgery, Writing - Review & Editing, Supervision
Dr. Vu Le Quang: Surgery, Writing - Review & Editing, Supervision
All authors approved the final manuscript.
Conflict of interest
The authors declare no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.