Introduction
Total knee arthroplasty (TKA) is a well-established orthopedic surgery commonly performed to improve pain and function in patients with end-stage osteoarthritis and other degenerative joint diseases.1 Perioperative complications following TKA remain an area of concern with regard to an aging and sicker patient population, specifically with regard to renal complications.
Incidence of postoperative renal failure requiring dialysis, while rare, is a serious complication of TKA and is associated with increased morbidity, mortality, length of stay (LOS), and healthcare costs, as shown in studies of both hip and knee arthroplasty.2 Postoperative renal dysfunction, even in mild or transient forms, has been associated with worsening long-term renal function and longer recovery times.3 Yet, incidence, predictors, and pathophysiologic contributors to postoperative renal failure requiring dialysis following TKA are not well described in orthopedic literature.4
Existing studies of postoperative renal complications have been primarily focused on cardiac and major abdominal surgeries and do not translate well to an orthopedic population.5 In addition, previous work in this area has been limited by small sample sizes, underreporting of renal complications, and lack of perioperative granularity leading to lack of effective risk stratification tools for patients undergoing TKA.6,7
There are a number of potential risk factors for postoperative renal failure requiring dialysis, described in the surgical literature that may apply to patients undergoing primary TKA, including preexisting chronic kidney disease (CKD), diabetes mellitus, congestive heart failure, preoperative use of nephrotoxic agents (NSAIDs, ACE inhibitors, etc.), intraoperative hypotension and prolonged operative time.8 To date, the comparative contributions of these individual factors in primary TKA have not been elucidated in a large, national data set.
The aim of this study is to use the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to develop and validate a predictive model for postoperative renal failure requiring dialysis in the primary TKA population.9 Additionally, we hoped to identify the preoperative and perioperative risk factors with the greatest effect size and model an adjusted risk stratification score for use by clinicians to help with risk stratification, clinical decision making, and preoperative optimization to possibly decrease renal complications and improve outcomes following TKA. As arthroplasty increasingly shifts toward enhanced recovery pathways and outpatient surgery, improved identification of patients at elevated risk for postoperative complications has become increasingly important for perioperative planning and risk stratification
Methodology
Patients undergoing primary total knee arthroplasty were identified in the ACS-NSQIP database using CPT code 27447. Data from 2018-2022 were analyzed. Patients with missing key variables were excluded. The final cohort included 308,121 patients, of whom 442 developed postoperative renal failure requiring dialysis. The outcome of interest, postoperative dialysis, was coded as the dependent variable (yes/no), and potential predictor variables were coded as independent variables. The independent variables were age, sex, body mass index (BMI), operative time, ASA physical status classification, comorbid conditions such as diabetes, pre-existing renal failure, congestive heart failure, and hypertension requiring medication, all of which have been previously identified as established risk factors for postoperative renal dysfunction.10 Multivariable logistic regression was used to assess independent predictors of postoperative dialysis.11 Collinearity was assessed using variance inflation factors. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for all variables. The model performance was assessed using the area under the receiver operating characteristic curve (AUC),12 while model fit was evaluated using likelihood ratio tests. Statistical significance was defined as p < 0.05 for all variables.
Results
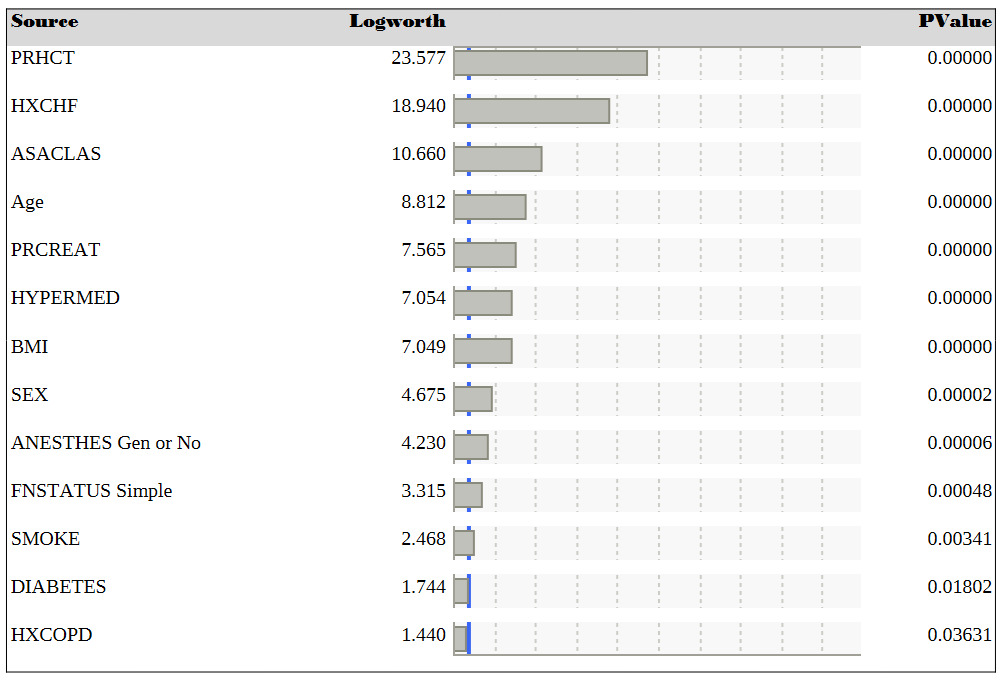
Figure 1 lists the factors most strongly associated with postoperative renal failure requiring dialysis after total knee arthroplasty (TKA). In this table, variables are presented by LogWorth (−log10 p-value), from lowest to highest, indicating the strength of their association with the outcome of interest. The variable at the top of the table is the preoperative hematocrit value. A lower value, potentially representing anemia, is associated with increased risk of postoperative renal failure requiring dialysis. The remaining variables in this table are well-known risk factors for kidney injury or dialysis, including American Society of Anesthesiologists (ASA) physical classification (ASACLAS), advanced age, higher body mass index (BMI), hypertension requiring medication (HYPERMED), prolonged operative time (OPTIME), anesthesia type, smoking (SMOKE), male sex (SEX), preoperative creatinine level (PRCREAT), preoperative renal failure, and diabetes.

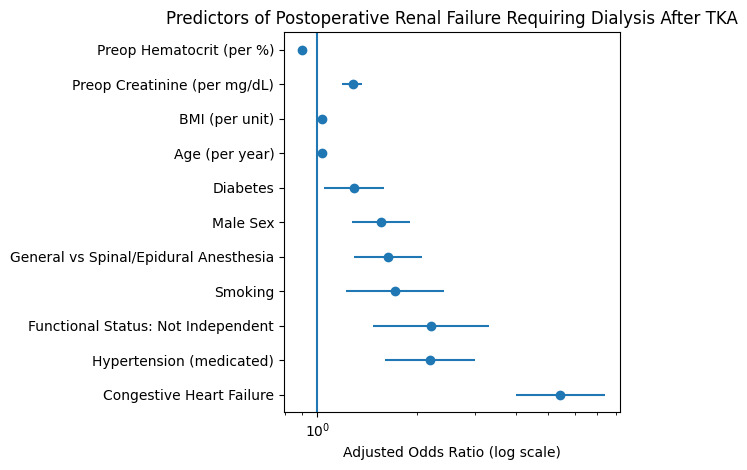
Figure 2 depicts a Forest plot illustrating adjusted odds ratios (ORs) with 95% confidence intervals for independent predictors of postoperative renal failure requiring dialysis following primary total knee arthroplasty, derived from multivariable logistic regression analysis. Variables positioned to the right of the vertical reference line (OR = 1) are associated with increased odds of postoperative dialysis, whereas those to the left represent protective associations.13 Congestive heart failure demonstrated the strongest association with postoperative dialysis, followed by hypertension requiring medication and impaired functional status. Patient-level physiologic factors, including increasing age, higher body mass index, and elevated preoperative creatinine, were also independently associated with increased risk. In contrast, higher preoperative hematocrit was associated with lower odds of postoperative renal failure. Odds ratios are adjusted for all covariates included in the final multivariable model.

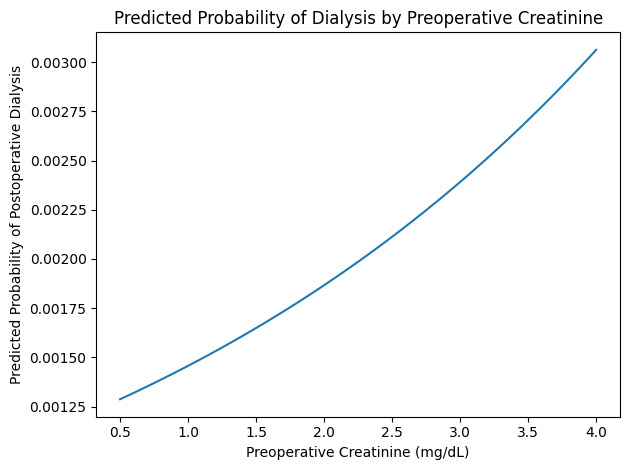
Preoperative creatinine (PRCREAT) has an odds ratio of 1.47, meaning that each 1 mg/dL increase in preoperative creatinine was associated with a 47% increase in odds of postoperative dialysis. This finding is consistent with the fact that creatinine is a known marker of kidney function.14 Figure 3 depicts the predicted probability curve illustrating the relationship between preoperative serum creatinine and the risk of postoperative renal failure requiring dialysis following primary total knee arthroplasty. The curve was derived from the multivariable logistic regression model and reflects the adjusted effect of creatinine while holding other model covariates constant. Increasing preoperative creatinine is associated with progressively higher predicted risk of postoperative dialysis. Although the absolute risk remains low due to the rarity of this complication, the relative increase in risk highlights the importance of preoperative renal function in perioperative risk stratification.

Body mass index (BMI) also had an odds ratio greater than 1, making it a potential risk factor for kidney injury. The other predictors with ORs greater than 1 were age and operative time. It is likely that these variables are risk factors due to greater physiological stress. Preoperative hematocrit (PRHCT) had an odds ratio less than 1, indicating that higher hematocrit levels are associated with lower odds of postoperative kidney injury or dialysis.

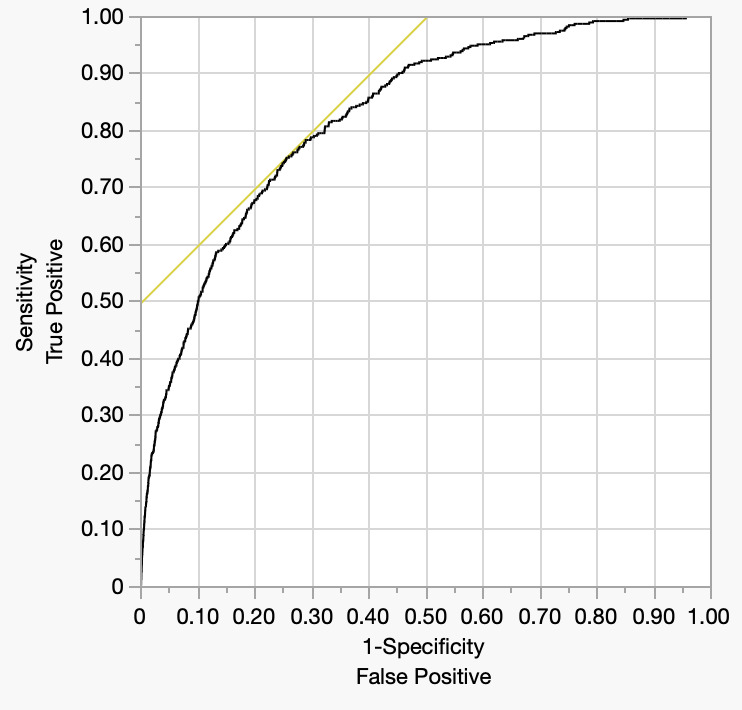
Figure 4 depicts the Receiver Operating Characteristic curve (ROC curve) from the logistic regression model. The ROC curve is a graphical representation of a statistical model’s diagnostic ability. The ROC curve plots the sensitivity or true positive rate on the y-axis versus 1-specificity or false positive rate on the x-axis at every possible cut-point for the data used to classify a new observation.15 As can be seen, the curve increases rapidly towards the upper left corner, suggesting that the model has good discriminative ability. The AUC (area under the curve) for the outcome of postoperative dialysis was 0.82601. This would be considered very good predictive performance. These findings indicate that the preoperative and perioperative variables selected for this study are effective in identifying those at increased risk for postoperative renal failure requiring dialysis.
Discussion
The results of the current analysis suggest physiologic reserve, as evidenced by renal and hematologic reserve, was the strongest predictor of postoperative dialysis following TKA. Preoperative creatinine is a significant risk factor and hematocrit was a significant protective factor. The findings are not surprising as renal clearance, and hematologic parameters are critical determinants of end-organ perfusion.16 Our data are also in alignment with previous studies indicating renal insufficiency represents a high independent risk factor for perioperative morbidity and mortality in even low-risk and elective surgeries.17 This contrasts with single variables like demographics or comorbidity burden which represent a step removed from the physiologic basis of renal injury. If this hypothesis is correct, then preoperative optimization of fluid status and avoidance of nephrotoxic medications may have a more meaningful impact than conventional population-wide risk assessment.18 There are also data from anesthetic literature that suggest intraoperative maintenance of hemodynamic parameters, especially renal perfusion pressure, may reduce the development of acute tubular injury and decrease dialysis risk. This suggests that the combination of renal and hematologic parameters may be the foundation for a more physiologic and individualized risk stratification process which incorporates both filtration and oxygen-carrying capacity.19 The protective effect of higher hematocrit also emphasizes the importance of prevention of renal ischemic damage and the ability to facilitate tissue recovery. These findings suggest physiologic laboratory parameters may outperform traditional administrative risk metrics such as ASA classification in predicting renal complications.20 Demographic and surgical factors such as age, BMI, and length of procedure were significant in the multivariate model but did not have as strong independent risk profiles. As the above discussion addressed, these likely represent a surrogate or parallel stressors that are more markers of frailty, changes in metabolism, or extended exposure to anesthetics than direct physiologic factors causing renal insult and injury.21 The AUC of the model was excellent and in line with the hypothesis that development of postoperative dialysis following TKA was not a random event but has a physiologic basis. The ability to identify these patients before surgery may allow for interventions that specifically target physiologic deficits including judicious perioperative hydration, and renal-protective anesthetic techniques.
Clinicians can apply the results of this study in their practice to identify high-risk patients for dialysis after TKA and optimize their care accordingly. Patients with risk factors such as pre-existing renal failure, diabetes, or ASA status of three or greater, can be identified preoperatively and closely monitored to prevent postoperative dialysis. Age and sex have also been identified as important demographic factors influencing the risk of postoperative acute kidney injury, highlighting the need for individualized perioperative monitoring strategies.22 Careful attention to renal perfusion and volume status can be implemented to prevent worsening renal function [23].
Limitations
This study has several limitations. First, the ACS-NSQIP database does not capture mild or transient acute kidney injury and only records severe renal failure requiring dialysis. Second, the database lacks detailed intraoperative variables such as hemodynamic parameters, fluid administration, and anesthetic technique. Third, residual confounding may exist despite multivariable adjustment. Finally, because this was a retrospective observational analysis, causal relationships cannot be inferred.
Conclusions
The current analysis supports increased attention to renal complications in arthroplasty. The contributions of this work include the development and validation of a predictive model for postoperative dialysis in TKA using a national database with thousands of cases, and the determination of a shortlist of risk factors for prioritization in interventions, risk stratification, and improvement efforts. Additionally, randomized trials or QI initiatives to mitigate the risk factors identified as most important in this study could further define the clinical pathways and patient management approaches that lead to improved outcomes.