
Introduction
Acetabulum fractures involve the socket of the hip bone where the femur articulates, forming the hip joint.1 These fractures are relatively uncommon (0.3–6%), primarily resulting from high-energy mechanisms such as traffic accidents or falls from height, affecting mainly younger adults due to the force required to break the pelvic ring.2 However, with an aging population, the incidence in older adults due to lower-energy falls is increasing (14%).3 The management of these fracture is crucial as they directly impact the articular surfaces of the hip joint, with outcome significantly influencing patient mobility and quality of life.4
For acetabular fractures, particularly in older adults or those with pre-existing joint conditions, acute total hip arthroplasty (THA) has emerged as an essential treatment option.5 THA provides an immediate solution to the joint damage and instability caused by the fracture.6 It is particularly beneficial in patients where the bone quality is compromised, or the fracture pattern suggests poor outcomes with traditional fixation methods.7 This approach is favored over conservative methods that typically offer suboptimal results in cases with severe comminution or osteoporotic bone where achieving stable fixation is challenging.
It utilizes various surgical approaches to address the complexity and specific nature of each fracture. The primary methods include the posterior, lateral, and anterior approaches. The posterior approach, most commonly used, allows excellent visualization of the hip joint but has a higher risk of dislocation. The direct lateral approach, favoring muscle preservation, offers potentially lower dislocation rates and is suitable for elderly or frail patients, although it may limit visibility of the anterior acetabular wall. The direct anterior approach is noted for its muscle-sparing benefits, promoting faster recovery and less postoperative pains, but require careful neurovascular navigations and is technically demanding.8 Selecting the appropriate approaches depend on the fracture’s specifics, patient anatomy, and the surgeon’s expertise, aiming to minimize complications and optimize functional outcomes. This tailored surgical strategy is crucial for enhancing patient recovery and long-term success of THA in treating acetabulum fractures.
The rationale for selecting THA in acute acetabulum fracture include the immediate restorations of hip function and pain relief. In the elderly, rapid mobilizations post-surgery reduces the risk of complications associated with prolonged immobility, such as deep vein thrombosis, pulmonary embolism, and muscle atrophy.9 Additionally, THA eliminates the prolonged weight-bearing restrictions often necessary after traditional fixation techniques. By replacing the joint, THA also circumvents the post-traumatic arthritis that commonly develops following severe acetabulum fractures, which would potentially require subsequent joint replacement.10
Despite the advantages of THA in managing complex acetabulum fractures, there is a significant gap in comprehensive clinical guidelines that delineate clear indications for choosing THA over fracture fixation in acute settings. Most current research focus on retrospective analysis with limited focus on prospective outcome, particularly concerning long-term function and quality of life post-THA in this patient cohorts.
This study aims to evaluate acute total hip arthroplasty (THA) for acetabulum fractures, detailing indications, patient selection criteria, surgical techniques, and managing intraoperative challenges. It assesses immediate and long-term complications, describes rehabilitation protocols, measures functional recovery with outcome scores, and compares these results to other treatments.
Cases Presentations
Case 1
A 75-year-old female with a medical history of hypertensions, ischemic heart disease, diabetes mellitus, and aortic stenosis present with severe pain and limited mobility in her right hip after an unwitnessed fall. Initial assessments in the emergency department included comprehensive survey and diagnostic imaging. Pelvic X-rays reveal a complex, comminuted fractures of the right acetabulum extending to the superior pubic ramus and other associated fracture, alongside diffuse osteoporosis. A subsequent CT scan identified mildly displaced fracture involving the right anterior and posterior acetabular columns and iliac bone, with additional injuries to the right inferior pubic ramus and ischial bone. The scan also shows a right-sided hematoma affecting the pelvic muscle.
Following orthopedic evaluation, she underwent a combined hip procedure (CHP) six days post-admission, utilizing dual surgical approaches for optimal fracture management. The procedure began with an Extended Smith-Peterson approach to address the anterior wall and column fractures, using a T-plate for stabilization. After repositioning, a Kocher-Langenbeck approach was employed to manage the posterior column. This phase encountered and resolved significant bleeding from the superior gluteal artery. The operation concluded with the placement of a cementless acetabular cup and a femoral stem, ensuring joint stability verified by intraoperative X-rays.
The postoperative period included ICU monitoring, where she initially remained stable until developing elevated troponin levels indicative of an NSTEMI on the fourth day, managed effectively with dual antiplatelet therapy and heparin. Her recovery progressed well, and she was discharged on the fourteenth day, satisfied with the surgical outcomes and recuperating under non-weight bearing physiotherapy protocols.
Case 2
An 81-year-old male with a notable medical history of hypertension, dyslipidemia, and benign prostatic hyperplasia presented with severe right hip pain following a fall on slippery ground. Initially evaluated, his imaging revealed a right acetabular fracture involving the anterior and posterior columns, as well as fractures of the superior and inferior pubic rami.
Upon admission, his laboratory investigations indicated a white blood cell count of 15.6, hemoglobin of 141 g/L, platelets of 272 × 10³/μL, and a creatinine level of 194 μmol/L, suggestive of possible acute kidney injury. Lower extremity Doppler studies were negative for deep vein thrombosis. Evaluation also revealed occult gastrointestinal bleeding and, notably, a positive blood culture for Morganella morganii. Physical examination documented pain-limited range of motion in the right hip but no other injuries.
He underwent CHP, open reduction and internal fixation of the right acetabular fracture followed by total hip arthroplasty, without intraoperative complications. Postoperatively, he was admitted to the ICU for close monitoring, later transferred to the floor, and managed for upper gastrointestinal findings of severe reflux esophagitis, gastritis, and peptic ulcers with esomeprazole. Infectious disease consultation led to treatment with meropenem for Morganella morganii and acyclovir for concurrent issues. His renal function stabilized, and physiotherapy was successfully initiated. Discharged in a stable condition.
Case 3
A 75-year-old woman with a complex medical history, including diabetes mellitus, hypertension, dyslipidemia, congestive heart failure, coronary artery disease managed by PCI, and non-small cell lung cancer, admitted after experiencing shortness of breaths and a subsequent fall, resulting in a left acetabular fracture. The fracture, characterize as an anterior column posterior hemi-transverse displaced with dome impactions, caused severe pain and significantly limited mobility. After evaluating both conservatives and surgical options and considering her overall frailty and severe osteopenia, it was determined that surgery was the most viable option to improve her quality of life.
Under general anesthesia, a two-staged surgical approach initiated. The patient was positioned supine for the first stage, which involved fixing the anterior column using a modified Smith-Petersen approach with anterior superior iliac osteotomy. Access was gained through an incision over the iliac crest, allowing for the reduction and stabilization of the fracture using a quadrilateral surface plate and an additional plate. The osteotomy was secured with a screw, and the site was closed in layers.
The patient was then repositioned laterally for the second stage via the Kocher-Langenbeck approach. The posterior column fracture was identified and stabilized with a plate and screws without the need for further reduction. The hip was dislocated, and the acetabulum prepared for a BI-MENTUM cup, which was press-fit and secured with additional pins and a screw. A Corail stem and a +8.5 femoral head were fitted into the femur, establishing stability within a dual mobility cup. Postoperatively, she maintained under strict hip precautions, utilized an abduction pillow, and received a heparin infusion initiated 6 hours after surgery. On the first post-op day, her pain was well-controlled, she remained vitally stable and afebrile with an intact left hip dressing. However, she exhibited a left foot drop with absent dorsiflexion and sensory loss over the dorsal foot. By the third day, despite the clean primary dressing, she reported distal thigh tenderness and ongoing neurological deficits. Physiotherapy with non-weight bearing mobilization and ankle orthosis commenced, leading to stable recovery with no further surgical complaints until discharge.
Case 4
A 60-year-old female with a history of hypertension, COPD, and a previously managed left acetabulum fracture presented with severe pain and restricted movement in her hip after a fall. An X-ray confirmed a right acetabular fracture involving both the anterior column and posterior hemi-transverse area, with notable central migration of the femoral head and significant joint dome impaction. The patient previously had a similar left-side fracture managed with ORIF, leading to protrusion, arthritis, and reduced mobility.
Given her medical history and the complex nature of the new fracture, a decision was made to perform open reduction and primary total hip replacement using a posterior approach. This strategy aimed to improve her mobility beyond the outcome of her prior left-sided ORIF, which had resulted in protrusion and arthritis.
During the procedure, the patient was placed in the lateral decubitus position and prepared using the Kocher-Langenbeck approach. After dislocating the hip and excising the femoral neck, the femoral head was processed into bone graft chips. Initially, the posterior column did not appear displaced; hence, an Avantage cup was attempted but proved unstable due to posterior column displacement and comminution. Consequently, the column was reduced and stabilized with a plate, and a Biomet cage was successfully secured with screws and a hook for enhanced stability.
A cemented polyethylene tri-polar cup sized at 50 millimeters was then inserted, ensuring correct abduction and anteversion. Stability was achieved with a cemented Accolade size 1 stem, following the instability of an initial uncemented stem trial. The surgery concluded with thorough irrigation, reattachment of the capsule and rotators, and skin closure using staples.
Postoperatively, the patient was stable with effective pain management and no complications. Physiotherapy began on day four, and by day five, despite noticing some swelling, a Doppler ultrasound ruled out DVT. The patient was discharged with satisfactory mobility, able to move from bed to chair, and expressed contentment with her surgical outcome.
Case 5
A 56-year-old male with no significant medical history presented to the Emergency Department following a fall down stairs, reporting severe pain, swelling, and tenderness in his left hip, alongside external rotation and abduction deformity but no skin bruising. Imaging revealed a displaced distal radius fracture and a left acetabular fracture characterized by a displaced posterior wall, near dislocation of the femoral head, significant femoral head impaction, and posterior wall bed impaction with extensive callus formation, indicating prolonged weight-bearing on a neglected fracture.
Given the complex injuries, the decision was made to perform total hip replacement and fixation of the distal radius fracture. Under general anesthesia, using the Kocher-Langenbeck approach, dissection through fibrous tissues revealed the expected extensive damage. A femoral neck osteotomy was performed, and the damaged posterior wall was meticulously managed with the repositioning and stabilization using two lag screws and a buttress plate. A defect at the posterior wall base was addressed with a strut graft from the femoral head, secured with screws.
The acetabulum was prepared for a Bi-Mentum cup size 57, achieving press-fit stability enhanced by pegs and additional screws. The femoral canal was prepared, and an 11 mm Corail stem with a plus 5 femoral head was inserted, ensuring stable fixation and optimal leg length.
The surgery concluded with thorough irrigation, reattachment of the capsule, and closure of the fascia, subcutaneous layers, and skin. The patient began physiotherapy on postoperative day one and was initially stable. However, by day three, he developed atelectasis in the left lower lobe, necessitating intensive spirometry. Following management, he stabilized and was discharged in good condition.
Case 6
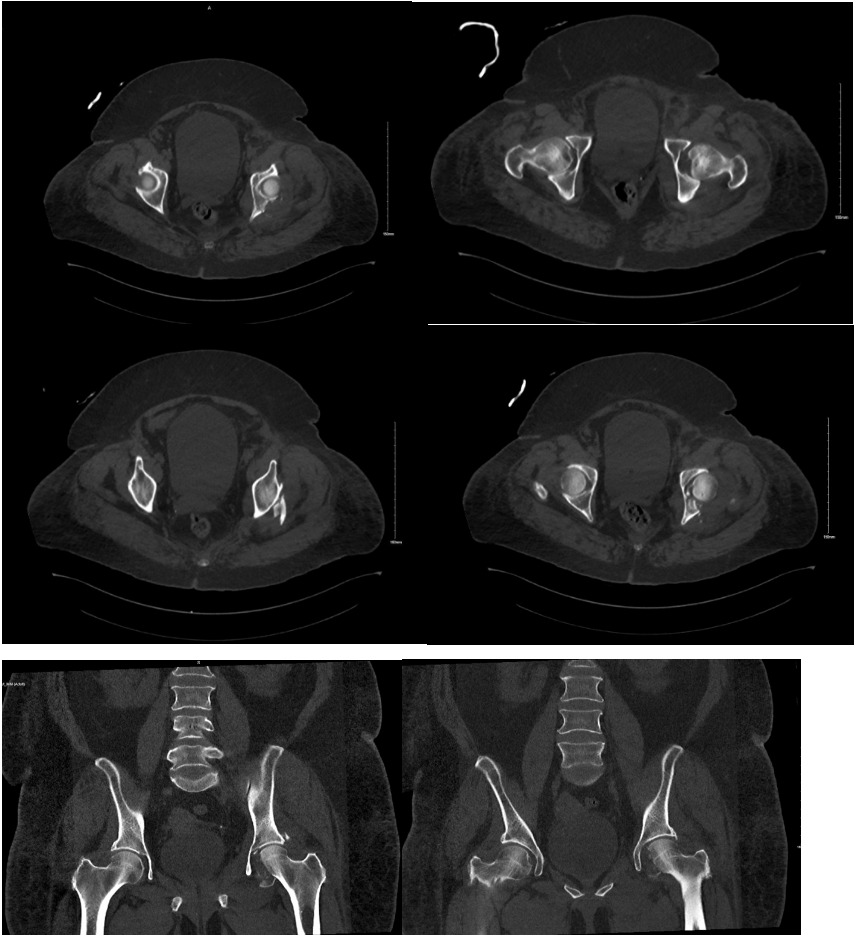
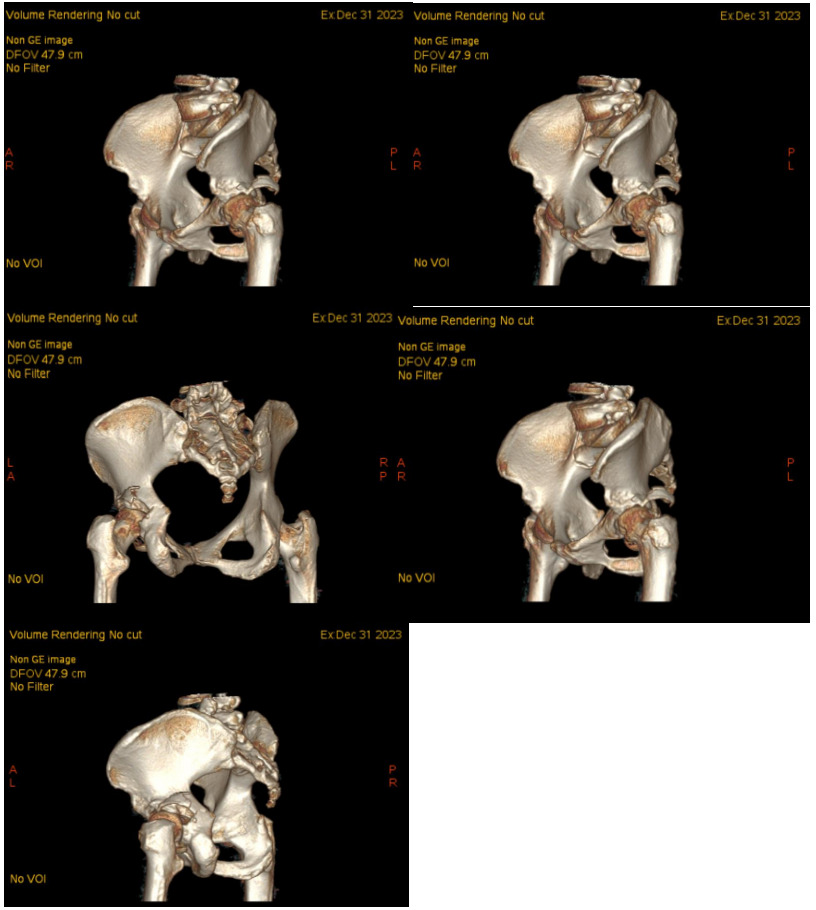
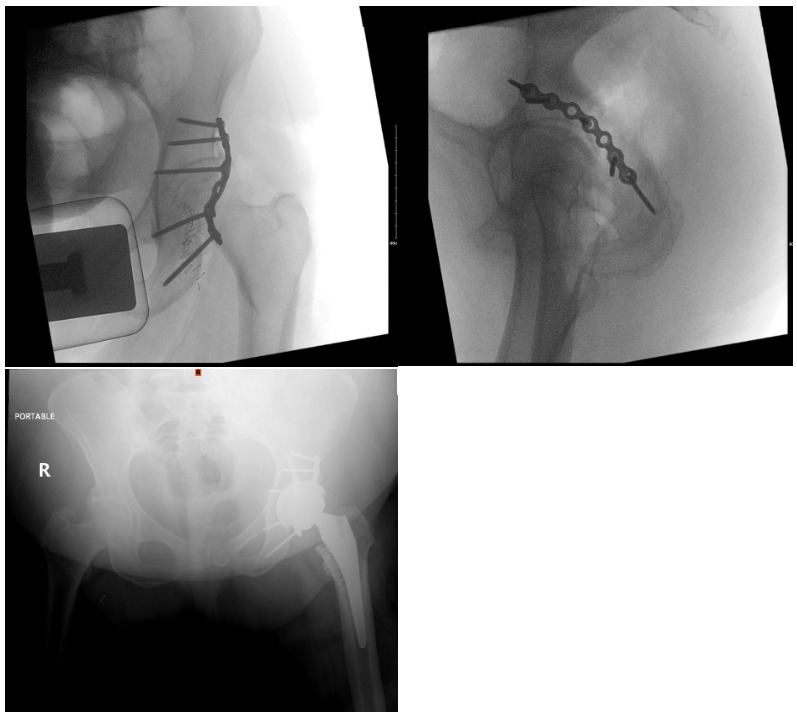
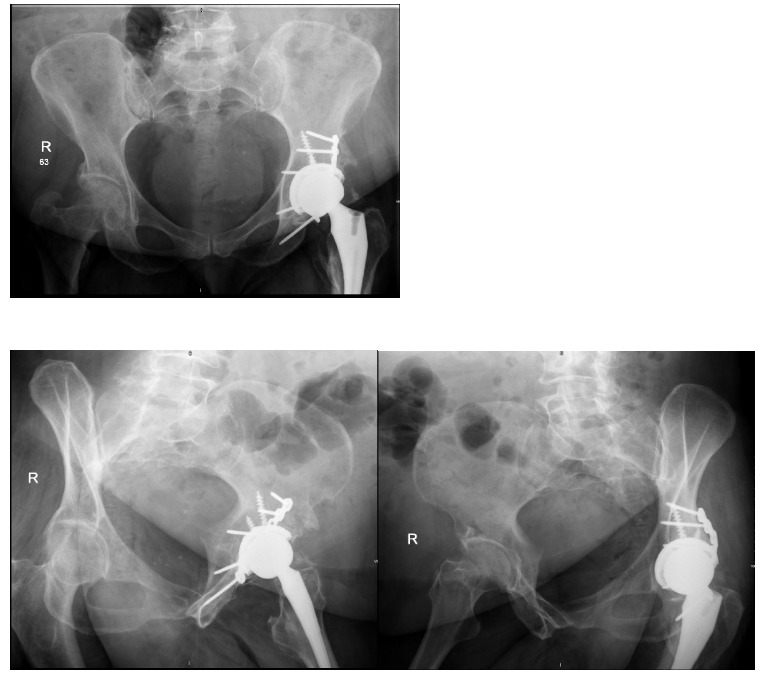
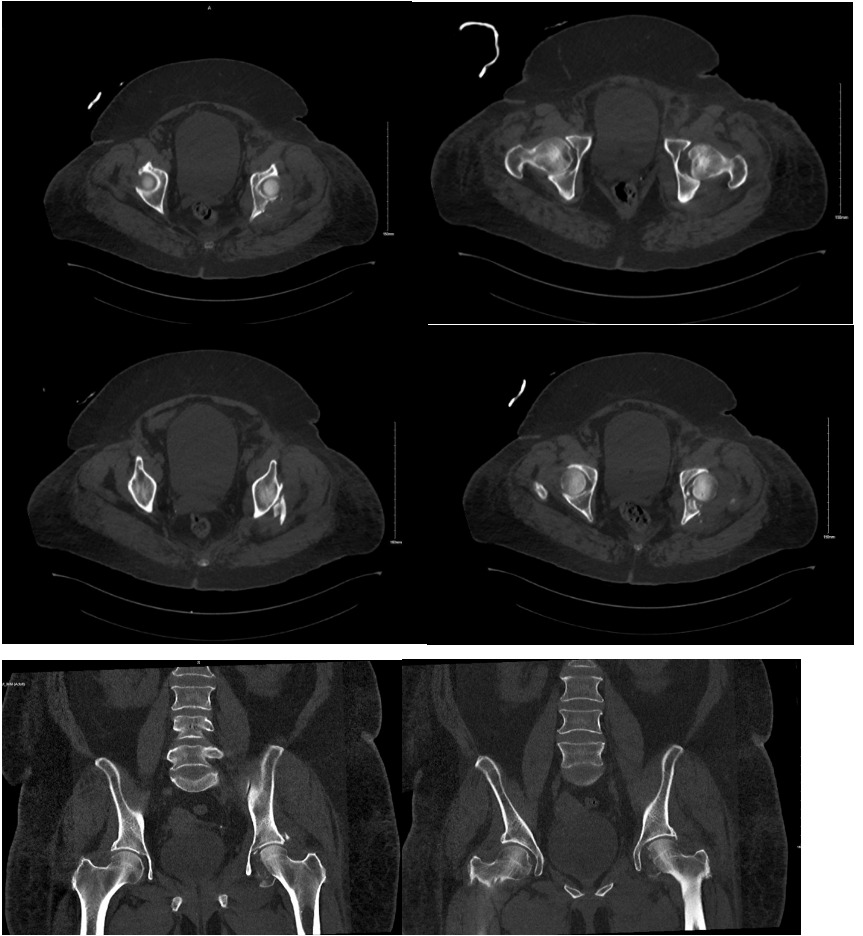
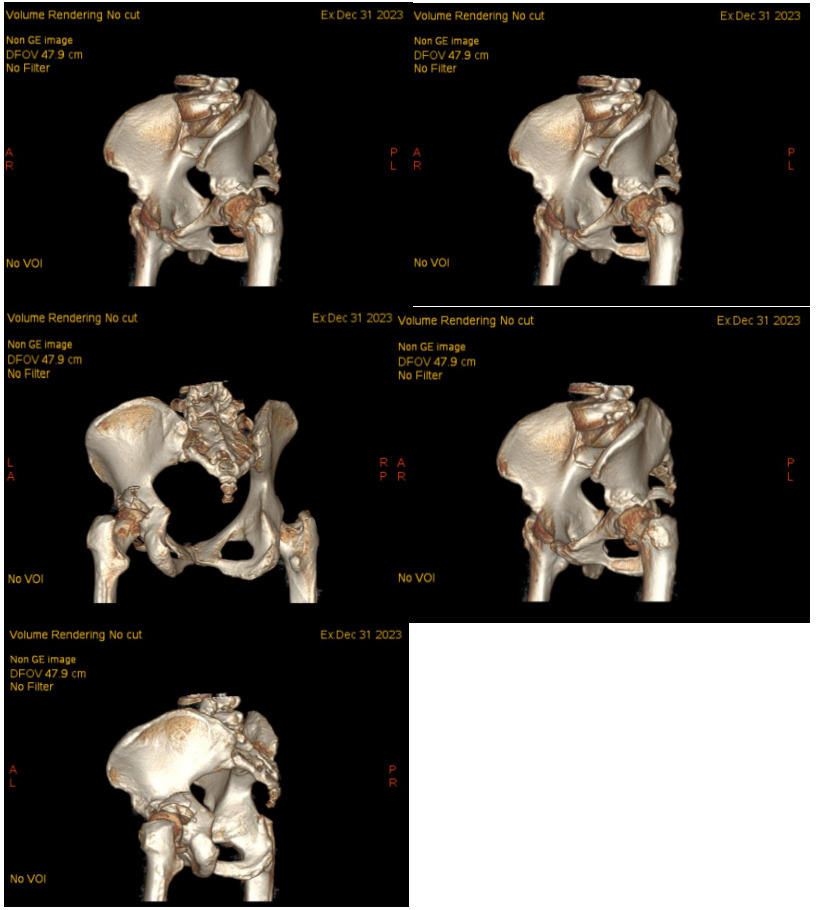
A 64-year-old female with diabetes, hypertension, and dyslipidemia was involved in a motor vehicle accident, resulting in significant injuries. She presented to the Emergency Department via Medivac and underwent a comprehensive trauma assessment. Orthopedic evaluations reveal a fractures dislocation of the left acetabulum with a posterior wall fracture and a femoral head fracture (Figure 1. Figure 2, Figure 3). Additionally, a minimally displaced fractures of the left tibial plafond was identified. Due to the complexity of her injuries and considering her age, a surgical plan was formulated for fixations of the acetabular and femoral head fractures, along with total hip replacements on the left side, and fixations of the tibial plafond fractures. After induction of general anesthesia and regional block, the patient was positioned in lateral decubitus for the hip procedures. Utilizing the Kocher-Langenbeck approach, the posterior wall fracture was stabilized with lag screws and a buttress plate (Figure 4A, 4B). The hip was then dislocated, the femoral neck cut, and the acetabulum reamed. A Stryker Trident cup size 46 was inserted for a press-fit, augmented with three screws, and a metal liner for dual mobility was added. Subsequently, the femur was broached, and an Accolade stem size 2 with a double head was implanted, ensuring excellent stability and appropriate legs length (Figure 4C). The operation concluded with thorough irrigation and closure in layers. The patient was then repositioned supine to address the tibial plafond fracture, which was stabilized with a single medial plate, followed by application of a dry dressing and a below-knee backslabs. Postoperatively, the patient experienced mild pain but was otherwise stable. Dressings on the left hip and ankle were intact, with ankle motion preserved and a palpable dorsalis pedis pulse. She began mobilization with physiotherapy from day one and showed no active complaints throughout her recovery, proceeding smoothly until discharge (Figure 5).

_showing_fracture_fixation_prior_to_tha._(c)_show.png)
_pelvis_x-ray_showing_stable_fixation_of_left_acetabulum_fracture_with_.png)
Discussion
Acute total hip arthroplasty (THA) for acetabular fractures presents a complex decision-making process impacted by patient-specific factors, fracture characteristics, and potential complications.11 The analysis of six distinct cases within our study provides a foundation to evaluate our surgical approaches, outcomes, and their alignment or deviation from existing literature. This discussion will explore how our techniques compare with broader clinical practices and the implications of our findings.
Notably, the literature supports the use of acute THA for managing acetabular fractures, particularly in the elderly, where the risks of post-traumatic arthritis and prolonged immobility are significant concerns.12 According to Judet and Letournel’s classification, the complexity of acetabular fractures can vary greatly, yet our approach has been to proceed with THA irrespective of the fracture pattern. This aligns with studies (Zhang et al. 2021) suggesting that immediate THA can be beneficial, especially when managing complex fracture patterns where traditional osteosynthesis may not offer stability or promote early mobilization.6
In our case series, each patient underwent a THA with variations in the surgical approach tailored to the specific fracture characteristics and individual patient anatomy. Notably, the use of dual surgical approaches (Extended Smith-Peterson for anterior structures and Kocher-Langenbeck for posterior structures) in Case 1 and similar strategic adaptations in other cases provided comprehensive access and effective management of both columns of the acetabulum. This diverges somewhat from standard protocols that may prefer a single approach, reflecting our aim to enhance fracture exposure and component positioning, which is pivotal in reducing postoperative complications like dislocation and improving functional outcomes. Paksoy et al. (2019 shows that anterior surgical approaches provide satisfactory outcomes in appropriate fracture types.13 Moreover, Anderson et al. (2023) shows that the anterior approach for acetabular fractures lowers dislocation risks compared to the posterior approach, but both can lead to nerve damage, blood loss, and infection.14
Notably, the outcomes of our surgical interventions reveal significant insights. The prompt and tailored approach led to satisfactory functional recovery in most cases, aligning with literature that underscores the importance of early mobilization in reducing complications such as deep vein thrombosis (DVT) and pulmonary embolism (PE). Similarly, Chatsis et al. (2018) shows that early mobilization reduces DVT and PE risks by enhancing blood flow and preventing venous stasis. Studies confirm it is safe and can relieve pain in anticoagulated patients.9 Despite the complex and varied nature of the injuries, the majority of our patients achieved early mobility, with a noted reduction in hospital length of stay (LOS) compared to typical recovery periods cited in current studies. Similarly, Nicol et al. (2023) shows that there was shorter stay in acute THA groups. However, ORIF delayed THA significantly increased total hospital stay.15
Interestingly, our approach diverged in the preference for cementless implants over cemented options, influenced by the literature supporting better long-term outcomes with cementless technology due to enhanced osseointegration. Corten et al. (2010) did a Kaplan-Meier survivorship analysis that showed cemented THA had a lower survival rates compared to cementless THA.16 This choice reflects our anticipation of improved patient outcomes and reduced revision rates, an essential consideration given the aging population.
Furthermore, the complications encountered, such as the NSTEMI in Case 1 and atelectasis in Case 5, underscore the need for vigilant postoperative monitoring. These complications align with literature findings that suggest a higher incidence of cardiac and pulmonary events post major orthopedic surgery, particularly in patients with pre-existing comorbidities17 (Urban et al., 2021). Moreover, the presence of Morganella morganii in blood cultures of case 2 is a rare but significant finding, as this gram-negative bacillus is often associated with nosocomial infections, particularly in immunocompromised individuals. Previous literature by Anagnostakos et al. (2021) indicates that M. morganii bloodstream infections typically arise from urinary or gastrointestinal sources, requiring broad-spectrum antibiotics such as carbapenems.18 Grade IV reflux esophagitis and peptic ulcers have been linked to prolonged NSAID use and H. pylori infection, necessitating aggressive proton pump inhibitor therapy. Acute kidney injury (AKI) is commonly associated with sepsis or nephrotoxic medications, with studies (Hobson et al. 2018) emphasizing early nephrology consultation and fluid resuscitation to improve renal recovery and prevent long-term complications.19
Implementing acute THA offers several advantages. Firstly, it circumvents the long-term complications associated with post-traumatic arthritis, commonly observed with ORIF techniques. Similarly, Current literature supports this strategic shift, noting that the rates of post-traumatic arthritis can range from 25–50%, significantly impacting life quality.20 Choudhary et al. (2024) show THA as an effective intervention for PTHA, improving pain, function, and quality of life, while emphasizing the need for ongoing research and innovation.21 Secondly, by facilitating earlier weight-bearing and mobility, acute THA can substantially reduce LOS and associated healthcare costs, echoing findings from multiple studies which emphasize the economic and functional benefits of this approach (Liang et al., 2023).22
Conclusion
Our approach to managing acetabular fractures with acute THA aligns well with contemporary orthopedic principles, emphasizing patient-specific strategies, the use of advanced surgical techniques, and the importance of early mobilization. The evidence from our cases supports the broader literature, indicating that while the approach to acetabular fractures remains complex and multifaceted, the strategic use of THA can offer substantial benefits in terms of recovery times, functional outcomes, and overall patient satisfaction. As such, our findings contribute valuable real-world data to the ongoing discussion about optimal strategies for acetabular fracture management in diverse patient populations.
Declarations
This study was approved by King Abdullah International Medical Research Center (KAIMRC). Institutional review board number NRR24/012/5. The requirement for informed consent was waived due to the retrospective nature of this study.
Consent for publication
Not applicable.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Competing interests
The authors declare that they have no competing interests.
Funding
No funding was obtained for this research.
Authors’ contributions
AZ, GH, RA and ZJ developed the idea and designed the methods. AG, and AQ collected the data. AG, ZJ, RA and AZ analyzed, interpreted, and presented the results. All authors wrote the manuscript. AZ, GH, AQ, and ZJ critically revised the manuscript for content and finalization. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Acknowledgements
Not Applicable.