Introduction
Ballistic trauma to the pelvis and acetabulum represents a small but disproportionately resource-intensive subset of orthopaedic injuries.1–3 Civilian gunshot wounds (GSWs) have increased substantially over the past two decades, mirroring national trends in firearm violence.4,5 These injuries require balancing hemodynamic stability, contamination control, visceral integrity, and skeletal reconstruction. Historically, management was derived from military experience with high-velocity (>2,000 ft/s) or blast mechanisms. However, civilian injuries differ fundamentally in projectile velocity (<2,000 ft/s), contamination pattern, and survivability.6
This review consolidates current evidence regarding civilian low-velocity pelvic and acetabular GSWs. Emphasis is placed on epidemiology, fracture morphology, concomitant injuries, antibiotic prophylaxis, outcomes, and special considerations when addressing various ballistic injuries. The objective of this review is to provide an evidence-based framework for modern orthopaedic decision-making and identify areas requiring further research.
Methods
A narrative review was conducted using PubMed, Embase, and Google Scholar from January 2005 through January 2026. Search terms included ballistic, gunshot, pelvis, acetabulum, and outcome. Reference lists of relevant articles were screened manually. Eligible studies comprised English-language clinical research, systematic reviews, and case series/reports concerning pelvic or acetabular GSWs. Three reviewers extracted data on epidemiology, fracture pattern/energy, contamination and associated injuries, management, antibiotics/duration, and outcomes. Study designs were varied and largely retrospective, therefore we opted for qualitative synthesis rather than meta-analysis.
Epidemiology
In 2023, 46,728 people died from gun violence in the United States, and was the leading cause of death for people ages 1-17 years old for the fourth year in a row.4,5 Recent pandemic-era analyses showed overall trauma activations declined while the proportion of penetrating trauma and GSWs increased.7 Pediatric firearm-associated fractures also increased over the last two decades, disproportionately affecting male adolescents in urban settings.8 Musculoskeletal firearm injuries have risen across multiple US datasets, with pelvic involvement representing a significant minority of orthopaedic GSWs.
Pelvic GSWs comprise roughly 10-20% of orthopaedic ballistic injuries, and predominantly low-velocity handgun GSWs at close range in the civilian population. In a national Medicare analysis of 9,765 firearm-related orthopaedic cases, 16.7% involved the pelvis and 6.5% the acetabulum.9 Additionally, these injuries incur among the highest hospital charges of orthopaedic firearm injuries, averaging around $400,000 in both pediatric and adult populations, reflecting the multisystem management, intensive level care, and staged reconstruction typical of these injuries.9,10 Pediatric cases with intra-cavitary organ injury have three to four times greater costs and length of stay (LOS) compared to isolated musculoskeletal injuries.10 Transpelvic trajectories frequently involve bowel, urogenital, and major vessel damage. These associated injuries, more than the osseous pattern itself, drive early morbidity and infection risk.
Osseous Injuries
Pelvic Ring
Low-velocity pelvic GSWs frequently involve the ilium and anterior pelvic ring. Posterior ring involvement is less common but increases the chances of mechanical instability.1,11 In contemporary civilian series, approximately 55-65% of pelvic fractures involve anterior ring structures, whereas posterior ring injuries of the sacrum or sacroiliac joint account for roughly 10-20% of cases. Although less common, posterior ring involvement is disproportionately associated with mechanical instability and a higher likelihood of need for operative fixation.1,11
Most extra-articular, stable fracture patterns can be treated non-operatively if contamination risk is appropriately addressed. Relative indications for operative management include mechanical instability (AO/OTA Type B/C), displacement (>2cm), open wounds requiring debridement, and fractures involving the acetabular articular surface.3 In unstable injuries, damage-control principles prioritize hemorrhage control via binder or sheet application, pelvic packing, and/or external fixation followed by staged definitive fixation. Contemporary posterior stabilization (e.g. percutaneous screw constructs) reduces operative time and fluoroscopy without compromising accuracy in complex posterior-ring patterns.12 High-energy or shotgun ballistic injuries may create sacral comminution or spinopelvic dissociation requiring lumbopelvic fixation, but this is uncommon in civilian ballistic injuries.13,14 Routine orthopaedic debridement is not indicated for extra-articular, low-velocity pelvic ballistic injuries in the absence of gross contamination or devitalized tissue. In a retrospective review of 110 civilian pelvic gunshot fractures, Watters et al. demonstrated no significant difference in acute infection rates between patients who underwent formal debridement and those treated nonoperatively, even in the setting of associated bowel injury. Notably, infections were rare overall and occurred predominantly in cases with intra-articular involvement or extensive soft-tissue compromise. Debridement should therefore be reserved for intra-articular fracture patterns, gross contamination, tissue necrosis, or wounds that fall within the surgical approach of planned fixation.3,15,16
Acetabulum
Across civilian series, acetabular involvement occurs in approximately 25-30% of pelvic GSWs.1,11 Posterior wall and posterior column fractures are the most frequently encountered patterns in civilian ballistic acetabular trauma. This reflects the predominant anterolateral-to-posteromedial projectile trajectories and the common position of the hip at the time of injury. These posterior acetabular fractures are commonly associated with intra-articular bone or projectile debris.1,11 These injuries carry a higher risk of post-traumatic arthritis due to direct chondral injury and synovial contamination, particularly when fragments violate the weight-bearing acetabular dome.
Extra-articular fractures are typically amenable to nonoperative care with protected weight-bearing. Greater than 2mm of articular displacement, intra-articular debris, instability, or incarcerated fragments warrant surgical intervention. In elderly patients with comminution or osteoporotic bone, acute arthroplasty for fracture with limited fixation is a reasonable alternative to anatomic open reduction internal fixation to mitigate avascular necrosis and allow early mobilization.17 Intra-articular bullets and fragments should be removed due to the risk of synovitis, septic arthritis, secondary arthropathy, and plumbism. Extra-articular fragments can generally be observed unless they produce mechanical symptoms or threaten neurovascular structures. Monitoring serum lead levels is appropriate in symptomatic patients or when intra-articular retention is suspected.18,19
Hip arthroscopy allows for minimally invasive extraction of bullets and evaluation of associated labral or osteochondral injuries following ballistic trauma. A systematic review by Niroopan et al. identified indications for hip arthroscopy in orthopaedic trauma including bullet extraction, removal of intra-articular loose bodies, arthroscopic-assisted fracture fixation, and treatment of concomitant labral injuries.20 Hip arthroscopy can be both technically and logistically challenging in ballistic injuries as visualization can be impaired by hemarthrosis or contamination, and fluid extravasation through capsular disruption can lead to serious complications. Abdominal compartment syndrome has been reported following hip arthroscopy for gunshot-related acetabular injuries, underscoring the need for low pump pressures, limited operative time, and a low threshold for conversion to open arthrotomy when visualization or joint stability is compromised.7,18,21
Associated Injuries
Bowel Injuries
Transpelvic trajectories often entail visceral involvement, with concomitant gastrointestinal injuries described in 24% to 59% of civilian cases.1,3,15,22 Across civilian series, bowel/rectal involvement strongly predicts fracture-related infection (FRI) and drives the need for additional anaerobic antibiotic coverage and coordinated care with general surgery. Computed tomography (CT) with contrast and selective sigmoidoscopy improves detection of rectal injuries when the trajectory or physical exam raises concern as missed rectal injury increases chances of deep infection.23–25 Pelvic ballistic fractures are notably at a higher risk of infection compared to extremity gunshot fractures.26–28 Diversion is individualized, and orthopaedic intervention should not precede contamination control. Najibi et al. discusses diverting colostomy as a key factor in reducing infection rates in patients with acetabular gunshot wounds complicated by bowel injury, concluding that the successful treatment of bowel injury directly correlated with infection control. Specifically, the presence of a bowel injury with primary anastomosis of the bowel was a significant predictor of deep infection, while diverting colostomy was associated with a reduction in the infection rate in select cases.29,30 Some studies have suggested that diverting colostomy offers limited benefit in reducing local pelvic infection complications overall, while acknowledging that diversion may have a role in cases with concomitant perineal or posterior wounds or extensive soft tissue injury. Some key factors that influence the decision to perform fecal diversion in patients with open pelvic fractures include location of soft tissue injury, presence of rectal or perineal wounds, extent of soft tissue injury, and timing of fecal diversion (within 48 hours of injury).31–33
Urogenital Injuries
Penetrating bladder injuries occur in 8% to 13% of pelvic fractures.1,11 In female patients, there is a significant association between anterior pelvic ring involvement and a high rate of uterine (50%) and vaginal (25%) injuries.11 CT cystography with retrograde contrast delineates extraperitoneal versus intraperitoneal injury. Suprapubic catheter diversion is indicated for complex extraperitoneal or intraperitoneal injuries. Urethral injuries warrant fluoroscopic urethrography, early urologic involvement, and special attention to foley catheter insertion to avoid worsening partial tears.34–37 Early communication between the orthopaedic and urologic teams is essential to optimize management of associated bladder injuries, so catheter choice/location and approach options are chosen in a manner suitable for both services.
Vascular Injuries
Early mortality in pelvic trauma is driven by hemorrhage, accounting for approximately 40-60% of deaths, with most occurring within the first 24 hours of injury.38,39 Although the majority of pelvic hemorrhage arises from venous plexuses and cancellous bone surfaces, penetrating mechanisms such as GSWs carry a higher incidence of arterial injury which is disproportionately associated with hemodynamic instability and mortality. The most commonly injured arteries include branches of the internal iliac system, namely the superior gluteal, internal pudendal, and obturator arteries. Less common are injuries to the external iliac or common femoral vessels; however, injury to these vessels confer a markedly higher risk of exsanguination.1,38 Early pelvic binder application, rapid hemorrhage control, angiography/embolization, and resuscitative endovascular balloon occlusion of the aorta (REBOA) are the current tools for battling vascular shock, with protocolized massive transfusion and hypotensive resuscitation strategies shown to improve survival.38
Spine Injuries
Thoracolumbar fractures are reported in approximately one-third of pelvic fractures in large trauma registries and are associated with higher injury severity scores, increased intensive care utilization, and greater mortality.40 Although these data derive predominantly from blunt trauma populations, the anatomic proximity of the pelvis to the lumbosacral spine renders these findings clinically relevant to pelvic GSWs, particularly in transpelvic trajectories.41 In ballistic pelvic trauma, spinal involvement more commonly reflects direct missile passage, bone-fragment retropulsion, or cavitation effects rather than axial loading mechanisms typical of blunt injury.42,43
Gunshot-related spine injuries most frequently involve the lumbar spine and sacrum and are often accompanied by neurologic deficits, including lumbosacral plexopathy or radiculopathy.44 Neurologic injury may occur even in the absence of overt vertebral instability. Outcomes are generally more favorable than in blunt spinal trauma, with partial neurologic recovery reported in approximately 50-70% of incomplete injuries.13,43 Accordingly, routine CT evaluation of the lumbosacral junction is recommended in pelvic GSWs when neurologic symptoms, midline tenderness, or high-risk trajectories are present, with early rehabilitation and neuropathic pain management playing a central role in recovery.40,41
Prophylactic Antibiotic Recommendations
Contemporary civilian data support short-course antibiotic prophylaxis with multiple series reporting no reduction of FRI with intravenous antibiotics >24-48 hours compared with ≤24-48 hours, including cohorts with abdominal hollow-viscus injury communicating with pelvic fractures.45,46 Rehman et al. evaluated 84 patients with low-velocity pelvic GSWs, including 59% with bowel involvement, and found no infections in extra-articular fractures, even in the presence of intestinal spillage.3 Dehne et al. analyzed 125 abdominal GSWs communicating pelvic or spinal fractures and compared short (≤48 h) and long (>48 h) prophylactic antibiotic courses. Infection rates, including osteomyelitis, meningitis, and Clostridioides difficile colitis were similar.45 Marecek et al. surveyed 220 Orthopaedic Trauma Association surgeons and found that 86% routinely prescribe antibiotics for low-velocity ballistic fractures, yet only 26% have institutional protocols. Most respondents provide 24-48 hours of coverage, generally guided by open fracture principles rather than ballistic-specific data.47 Additionally, a scoping review of FRIs following ballistic injuries conducted by Alt et al. found that antibiotic prophylaxis should be ≤48 hours as longer courses do not provide additional benefit and may even increase infection risk. They also found that retained bullet fragments are a key risk factor for FRI, and their removal during internal fixation, when safely feasible, can significantly reduce infection rates.48 Overall, there is broad variability in practice across institutions, which highlights the need for standardized guidelines tailored to ballistic injury mechanisms.
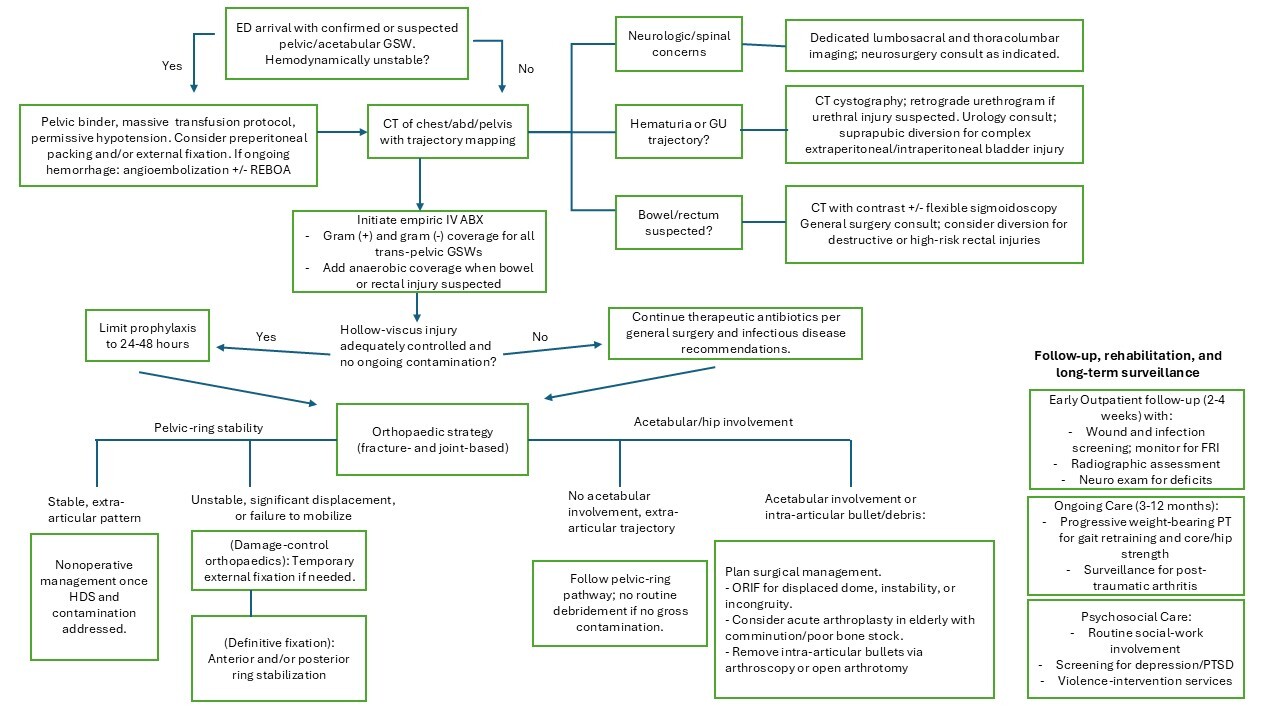
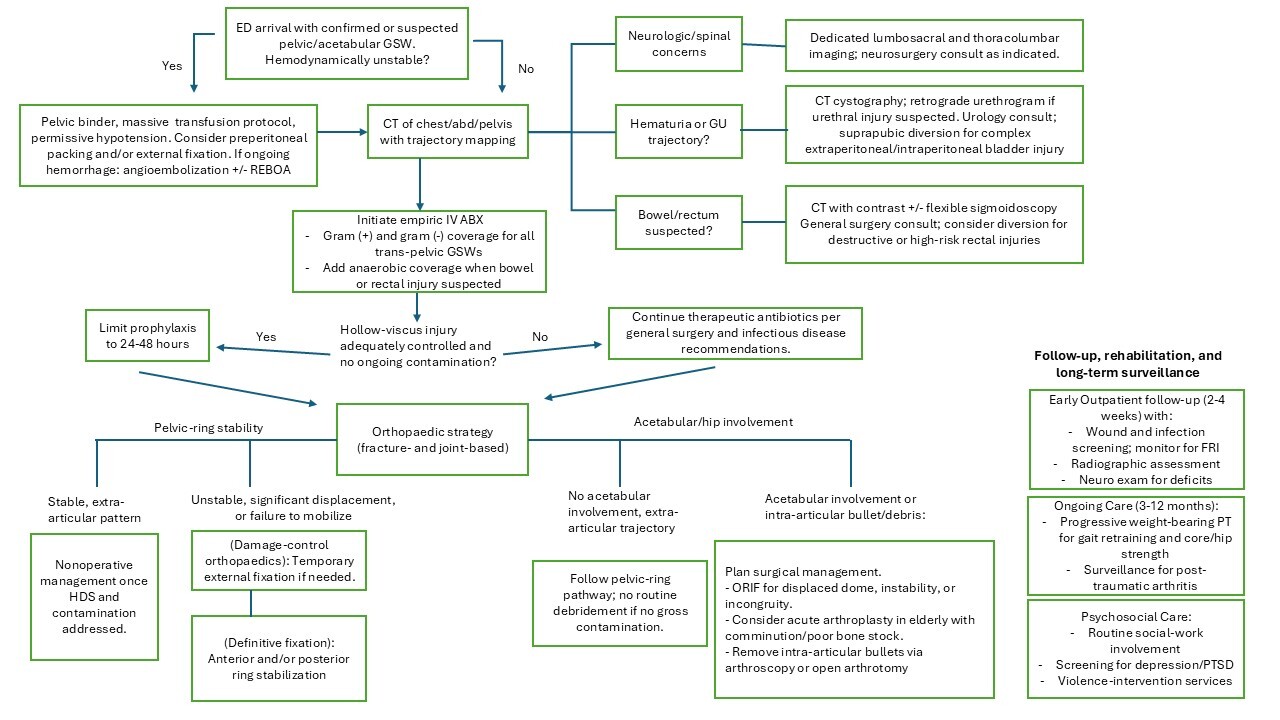
Collectively, these studies support short-course prophylactic systemic antibiotic use following civilian pelvic gunshot trauma. Empiric coverage should include gram-positive and gram-negative organisms with addition of anerobic coverage when bowel injury is suspected. Survey data indicated that cefazolin, often combined with an aminoglycoside, is the most common empiric regimen in civilian ballistic fractures, while metronidazole or a beta-lactam/beta-lactamase inhibitor may be added when bowel injury or gross contamination is suspected.3,45,47 Institutional flora and patient-specific risks may justify adding agents targeting resistant gram-positive organisms in select cases.49 A summary of treatment recommendations based on current literature is demonstrated in Figure 1.
Outcomes
FRI after civilian ballistic pelvic or acetabular injury remains relatively uncommon with appropriate initial management, with reported rates ranging from 3-9% across modern civilian cohorts.3,15,46,50 Infections occur mostly in patients with bowel or hollow-viscus involvement. Rehman et al. reported just one infection out of 84 low-velocity pelvic gunshot injuries, despite 59% with bowel involvement, with the single infection being an intra-articular hip injury with a retained bullet.3 Similarly, Watters et al. demonstrated no difference in infection rate between patients treated with and without formal operative debridement, and Dehne et al. found no benefit to extending antibiotic prophylaxis beyond 48 hours in abdominal gunshot wounds with pelvic or spinal involvement.15,45 In the largest civilian series to date, Coleman et al. analyzed 242 pelvic GSWs and reported an overall FRI rate of 4.5%, all in patients with bowel injury. However, trajectory through bowel was not independently predictive of infection.46 Microbiologic data further emphasizes the importance of early broad-spectrum coverage, as Ghali et al. demonstrated that gram-positive organisms accounted for 72% of infections (including 31% methicillin-resistant Staphylococcus aureus), while gram-negative bacteria comprised 31%, and anaerobes 19%.49 Collectively, these data indicate that infection risk in civilian pelvic gunshot trauma is driven by contamination rather than duration of prophylaxis or routine debridement.
Union after civilian pelvic and acetabular gunshot injury is generally reliable when fracture stability and contamination control are achieved. Reported nonunion and malunion rates remain below 5% and are more commonly associated with infection, severe comminution, or delayed stabilization.1,51 Persistent pain is more often due to heterotopic ossification (HO), nerve injury, or retained intraarticular fragments rather than nonunion. HO occurs in approximately 15–30% of acetabular gunshot injuries, particularly after surgical fixation or retained intra-articular fragments.51,52
Functional recovery is largely determined by neurologic integrity and associated visceral trauma rather than by the osseous injury pattern alone.51,53 Patients without neurologic deficit typically regain independent ambulation within 6–12 weeks, whereas those with lumbosacral plexus involvement require prolonged rehabilitation and assistive devices.53 In a modern civilian series, roughly 60–70% of survivors achieved preinjury functional independence by six months when early mobilization and multidisciplinary rehabilitation were implemented.53 Acetabular involvement carries a greater risk of long-term disability due to post-traumatic arthritis (PTA). Displaced or intra-articular fractures develop radiographic degeneration in 30–50% of cases and progress to total hip arthroplasty in up to 20% within 5–10 years, particularly when the projectile or bone debris violates the joint surface.51 Retained intra-articular fragments should therefore be removed to prevent secondary chondrolysis, lead arthropathy, chronic pain, and chronic infection.54
Neurologic complications are frequent with variable long-term sequelae. Lumbosacral plexopathy, sciatic neuropathy, and peroneal palsy occur in 10–30% of ballistic pelvic injuries, most commonly from direct missile injury, bone-fragment impingement, or ischemia.1,13,51 Clinical manifestations include foot drop, saddle paresthesia, and neuropathic pain. Prognosis correlates with injury completeness: neuropraxic injuries recover partially or fully in 60–70% of cases, whereas neurotmetic injuries carry poor prognosis.13,14 Electrodiagnostic studies may be obtained several weeks after injury to help distinguish injury severity, though prognostic assessment is typically most reliable after 6-12 weeks.42,43 Early multidisciplinary rehabilitation emphasizing gait retraining, spasticity control, and neuropathic-pain management with gabapentinoids or tricyclic antidepressants is essential.53 Persistent neuropathic pain remains a leading cause of long-term disability. Integration of pain specialists and orthotic support (e.g., ankle–foot orthoses, functional electrical stimulation units) improves ambulation and quality of life.55
Mortality in civilian pelvic gunshot injuries ranges from 4-10%, predominantly due to exsanguination and multisystem injury.38–40,56 Vitale et al. reported 5% mortality in pediatric pelvic fractures. Mohs et al. found mortality doubled (9.5% vs 4.3%) when thoracolumbar fractures accompanied pelvic injury.56 Davis et al. noted 3-5% mortality in low-velocity civilian cohorts compared to 26% in combat injuries, underscoring ballistic velocity dependence.38 Most deaths occur within 24 hours of vascular or visceral related injuries; late mortality from orthopaedic infections is rare.15,46
Gunshot recidivism occurs in roughly one in seven patients within five years and is closely linked to untreated mental-health conditions, unemployment, and unstable housing. Integrating psychosocial screening and social-work referral into orthopaedic after-care may be useful to reduce reinjury and improve functional recovery.53,55
Conclusion
Civilian pelvic and acetabular ballistic injuries represent a growing and resource-intensive challenge for modern trauma systems. Early mortality is largely driven by hemorrhage from arterial injuries, necessitating rapid intervention. A short course of prophylactic antibiotics (24-48 hours) is sufficient for most cases, even in the presence of bowel injury, provided definitive contamination control is achieved. Surgical intervention is indicated for mechanical instability, displaced weight-bearing structures, or to remove intra-articular debris to prevent long-term arthropathy and lead toxicity. Long-term functional outcomes are heavily influenced by neurologic integrity and multidisciplinary rehabilitation. Standardized, evidence-based guidelines are necessary to optimize these complex, multisystem injuries and improve the quality of life for survivors in urban trauma settings.
Authors’ contributions
Brian Kye: Substantial contributions to the acquisition, analysis, interpretation of the data; drafting and reviewing the content; final approval of submitted version; and agreement to be accountable for all aspects of the work.
Cameron Foster: Substantial contributions to the acquisition, analysis, interpretation of the data; drafting and reviewing the content; final approval of submitted version; and agreement to be accountable for all aspects of the work.
Porter Young: Substantial contributions to the acquisition, analysis, interpretation of the data; drafting and reviewing the content; final approval of submitted version; and agreement to be accountable for all aspects of the work.
Disclosures
The authors have no financial disclosures or potential other conflicts of interest.
This work has not been previously presented or published.