Introduction
Recently, the use of collared femoral stems in total hip arthroplasty (THA) has increased in popularity, rising from 39% to 67% from 2015 to 2025.1 Specifically, these collared femoral stems have demonstrated superior rotational stability, enhanced metaphyseal load sharing, and reduced risks of micromotion and early mechanical failure compared to collarless designs.2–4 Additionally, the use of the collar has been shown to decrease the risk of periprosthetic femur fractures (PFF) compared to collarless stem .4,5
While much of the existing literature has focused on the mechanical advantages of collared stems, the clinical and biomechanical implications of a postoperative gap between the collar and calcar remain underreported. Most studies fail to account for the potential influence of this calcar-collar gap (CCG) on implant stability and load transfer, which may compromise the intended mechanical benefits of the collar. Furthermore, achieving adequate collar seating on the calcar can be difficult due to anatomical variations, differing stem design, differences between broach and implanted component diameter and friction fit, as well as the quality of the femoral neck osteotomy and subsequent calcar planing.6Additionally, although collared stems have been associated with lower overall PFF rates, collared stems have been reported to have higher intraoperative PFF rates at time-zero implantation.5 This finding raises the possibility that forceful broaching to obtain immediate collar–calcar contact may increase early fracture risk.
This scoping review aims to systematically evaluate the existing literature on CCG, with particular focus on incidence, biomechanical and finite element analysis (FEA) findings, implant subsidence, and patterns of calcar resorption and stress shielding associated with collared femoral stems.
Methodology
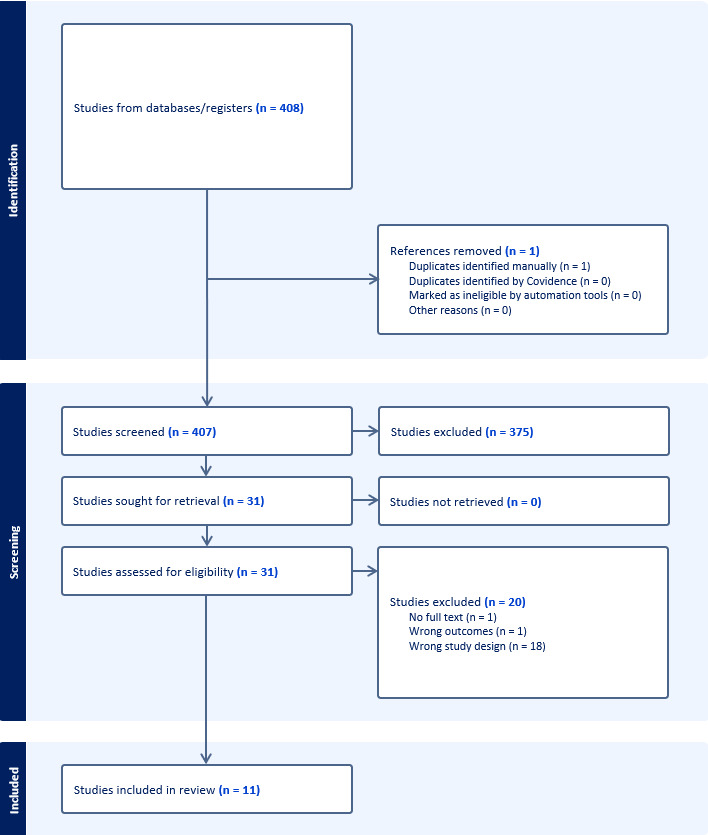
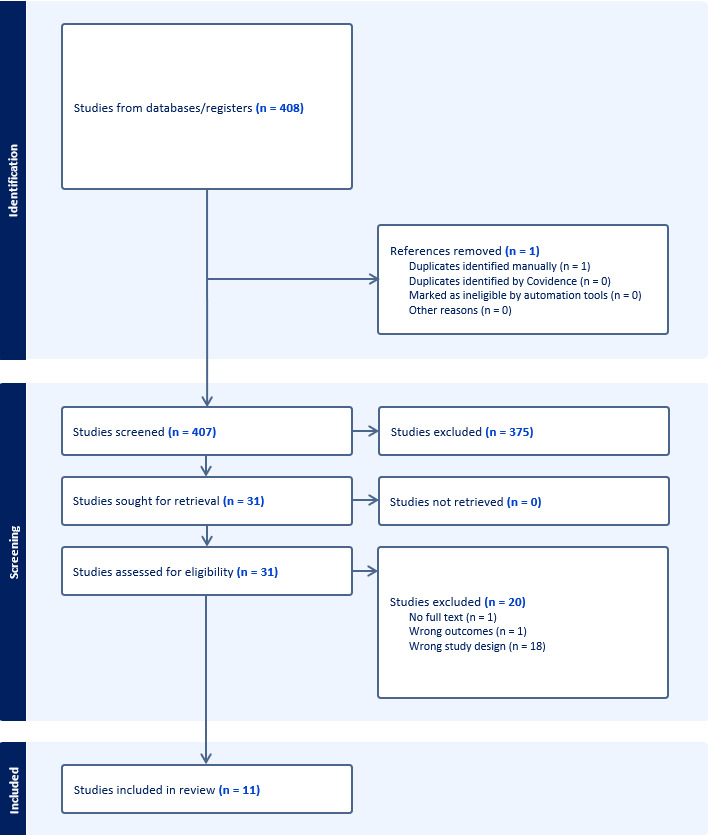
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for scoping reviews, we designed a scoping review to map the key concepts and evidence in the existing literature regarding the incidence, subsidence, biomechanical implications, and calcar resorption associated with CCG in THA. A comprehensive search of several databases was performed in December 2025. No language or date limits were applied to the search. Animal studies were excluded. Databases searched (and their content coverage dates) were Ovid MEDLINE(R) (1946+ including epub ahead of print, in-process, and other nonindexed citations), Ovid Embase (1974+), Ovid Cochrane Central Register of Controlled Trials (1991+), and Scopus via Elsevier (1970+). Search strategies were developed and executed by a medical librarian in collaboration with the study investigators, using controlled vocabulary supplemented with relevant keywords. The full search strategies, including all terms and Boolean operators, are provided in the supplemental material.
Four hundred and eight articles were identified and screened independently by two authors (S.Y., R.A.). Studies excluded by both reviewers were removed and disagreements were resolved by including a third reviewer to act as a tiebreaker. Inclusion criteria consisted of studies (clinical, cadaveric, finite element analysis, or sawbone models) reporting quantitative data on CCG incidence, subsidence rates, calcar resorption, biomechanical testing of load transfer, micromotion, or stability related to CCG in collared femoral stems during THA. Exclusion criteria included ongoing/unpublished clinical trials, editorials, commentaries, textbook chapters, isolated surgical technique descriptions, and prior systematic/scoping reviews or meta-analyses on the topic, to ensure focus on primary evidence addressing the review objectives. Eleven studies were ultimately included in this study (Figure 1).
Data Collection
Working independently using an extraction form, data was collected from each study on the study design, population, and outcomes measures including evaluation of CCG incidence, quantitative measurements of gap distance, stem subsidence rates, and biomechanical testing results.
Quality Assessment
Two independent reviewers (S.Y. and R.A) assessed the methodological quality of eligible studies using the Newcastle-Ottawa Scale (NOS),7 a widely validated instrument specifically designed for evaluating the quality of non-randomized observational studies (Table 1). Assessments covered key domains including representativeness of the exposed and non-exposed cohorts, ascertainment of exposure, comparability between cohorts on basis of design or analysis, integrity against outcome assessment biases, and adequacy of follow-up duration and completeness. Any discrepancies between reviewers were resolved through discussion to achieve consensus. Biomechanical studies were excluded from formal quality assessment, as their in vitro nature precludes applicability of clinical observational study quality tools like the NOS, focusing instead on standardized experimental protocols.
Results
Calcar-Collar Incidence (gap/contact frequency and time course)
Six studies reported quantitative data on the incidence of CCG presence with studies ranging from 1988 to 2025 (Table 2). All studies were retrospective observational studies that utilized radiographic assessment to evaluate the presence and distance of gaps between femoral calcar and the prosthetic collar of a femoral stem (range: 94-592 stems).8–13 For all studies, CCG was defined as a binary value of radiolucency or radiographic visualization of complete separation between the undersurface of the collar and the most medial portion of the femur. Ohashi et al.11 specifically measured the presence of a medial CCG and lateral CCG documenting each independently for all stems. A complete description of each studies methodology for CCG is present in Table 2. Imaging time frames ranged from immediate postoperative to 5-year follow-up. Following surgery, the initial postoperative radiographs demonstrated the incidence of collar-calcar gaps as 18.7%,8 35%,11 36.1%,10 and 53.9%.9
Two studies analyzed the incidence over time. Hawkins et al. reported complete osseointegration of 66.7% of the initial 18.7% of patients with gaps at 1-year follow-up, with only 6.3% of patients still having no or partial filling.8 Ohashi et al. reported a gap disappearance rate of 76.4% within 36 months, with only 8% of patients having a gap at a 3-year follow-up.11 Notably, Ohashi et al. determined that lateral gap distance at baselines was a significant predictor of gap disappearance whereby receiver operating characteristic (ROC) curve analysis demonstrated a 5.5 mm maximal cutoff for lateral gaps likely to close via osseointegration.11 Han et al. and Soballe et al. reported incidence of CCG at final follow as 53% and 34%, respectively.12,13 Notably, Hawkins et al.8 and Ohashi et al.11 were the only two studies that evaluated gap closure in the context osteointegration, explicitly accounting for stem-subsidence to differentiate between gap filling and migration. Hawkin’s et al.8 demonstrated <1% of stems at 1-year showed subsidence meaning closure could be attributed to integration, while Ohashi et al.11 excluded patients with >2mm of subsidence and used logistic regression to demonstrate subsidence did not predict closure.
Collar–Calcar Biomechanical Testing (in vitro)
A total of five studies investigated the biomechanical implications of CCG through in vitro testing, utilizing composite femurs, cadaveric specimens, or finite element analysis (Table 3). Lamb et al. conducted a composite femur in vitro study utilizing 3 groups of 6 composite fevers at increasing calcar-collar separation (0, 3, and 6 mm). Each specimen underwent a standardized torsional loading protocol measuring fracture torque, rotational displacement at fracture, torsional stiffness, and rotational work to failure. They found that without CCG, fracture torque was higher (47.33 vs 38.26 Nm, p = 0.05), rotational displacement was lower (16.6° vs 21.2°, p = 0.07), and torsional stiffness was significantly greater (151.38 vs 96.86 rad·Nm⁻¹, p < 0.01), while rotational work did not differ (p = 0.60).14 Harrington et al. utilized 8 cadaver femurs in an in vitro cadaveric stair-climbing model, where cemented femoral stems loaded under physiologic joint reaction forces. They found that when CCG was created by removing a 0.5-mm slice of bone beneath the collar, peak principal tensile strains in the proximal cement mantle increased by 1.5-2× compared with conditions without CCG.15 Markolf et al. found that the removal of calcar support increased collar displacement by 8-28% for standard collars (p <0.005). Additionally, the presence of CCG increased stem subsidence by 45-91%.16
Collar-Calcar Biomechanical Testing (FEA)
Two studies utilized finite element analysis to evaluate stress distribution and micromotion at the bone-implant interface. Watanabe et al. utilized 3 FEA models of collar (C), non-contact collar (NC) and collarless (CL) to asses micromotion under flat walking and stair climbing conditions. The contact model (C) demonstrated the lowest stem-bone micromotion under both loading conditions, with median values of 56 µm during flat walking compared with 67 µm and 66 µm for the non-contact (NC) and collarless (CL) models, respectively, and 79 µm during stair climbing compared with 99 µm and 98 µm for NC and CL. Reductions in micromotion with no CCG were most pronounced in the proximal region of the stem.17 Jeon et al. performed a three-dimensional element hip model that compared a collared stem with perfect calcar contact, a collared stem with imperfect contact, and a collarless stem under a simulated walking load. They found that collared stems demonstrated lower lateral stem tilting (~541 µm), whereas imperfect contact produced the greatest tilting (~567 µm), acting as a pivot under load.18
Stem Subsidence
Four studies investigated the relationship between CCG and stem subsidence (Table 4). Weiner et al. found that patients were much more likely to have subsidence when a CCG was present (19.0% vs 1.3%; p < 0.001) as well a greater magnitude of subsidence (mean 0.35 ± 0.74 mm vs mean 0.02 ± 0.24 mm; p < 0.001).10 Dammerer et al. also found greater subsidence when a gap was present in collared stems however this finding did not reach statistical significance (2.0mm vs 1.3mm; p > 0.05).9 Ohashi et al. commented that subsidence did not influence gap disappearance (0.54 OR; CI: 0.14-2.13; p = 0.375), while Hawkins et al. mentioned that out of 592 collared stems they analyzed only 0.8% of the stems demonstrated subsidence.8,11
Stress shielding and Remodeling
Two studies evaluated the effect of stress shielding and remodeling (Table 5). Han et al. demonstrated no significant relationship between calcar-collar contact and stress shielding, defined as proximal femoral bone resorption from altered load transmission, radiographically characterized by calcar rounding and/or cortical bone loss in the femur. They found that calcar resorption occurred in 91% of stems at minimum 10-year follow-up, however did not find a statistically significant association between CCG and stress shielding (p >0.05).12 While Soballe et al. mentioned that at 5-year follow-up, calcar resorption occurred in 16% of hips with no CCG at the time of implantation compared with 30% of hips with an initial CCG, suggesting that a CCG rather than the presence of a collar may lead to subsequent radiographic changes consistent with stress shielding .13
Discussion
The aim of this scoping review was to synthesize information available on CCG with femoral stem placement in THA. Our review found that CCGs are a common radiographic finding postoperatively with biomechanical and FEA implications demonstrating inferior rotational stability, greater periprosthetic femoral fracture risk, and micromotion. Of note, however, when radiographic assessment is performed over time, a substantial proportion of these collar gaps demonstrate osseointegration and gap closure over time.
Many of the studies in our review analyzed the incidence of CCGs through radiographic assessment, ranging from ~20-50% indicating that a substantial proportion, and in some series more than half, of patients exhibit CCG immediately following implantation.8,9 This variability is likely attributable to differences in surgical technique, implant design, and patient-specific anatomy. Importantly, among studies with longitudinal radiographic follow-up, rates of osseous integration were high, suggesting that bone remodeling frequently facilitates gap closure. However, no studies definitively established a threshold gap distance predictive of osseointegration. One investigation identified 5.5 mm as a potential cutoff, while another reported a 3.8-fold increased risk of persistent gap for every 1 mm increase in separation.11,14 Further studies are needed to better define clinically meaningful thresholds that may guide surgical decision-making
Biomechanical testing and FEA consistently demonstrated that direct collar–calcar contact provides superior rotational stability, increased resistance to periprosthetic fracture, and reduced micromotion compared with collared stems exhibiting a gap. Furthermore, Watanabe et al. specifically demonstrated that when CCG is present, the implant functions similar to a collarless stem.17 Together, our analysis of the studies demonstrated that the biomechanical advantages conferred by the collar are contingent upon direct engagement with the femoral calcar, as the presence of CCG negates the intended load transfer mechanism. Furthermore, subsidence was found to be significantly greater in the presence of a CCG, further underscoring the critical role of preventing CCG in early implant stability
Discussion surrounding stress shielding and bone remodeling was limited to only two investigations with very limited analyses. Soballe et al. reported reduced calcar resorption in hips with time-zero contact, while Han et al. found no significant association between collar contact and stress shielding–related outcomes.12,13 The limited evidence requires further analyses to better understand the long-term biological consequences of CCG on bone remodeling patterns and stress shielding.
Notably, this review did not identify studies directly evaluating the risks associated with aggressive broaching or reaming techniques aimed at preventing CCG. While achieving direct contact may enhance rotational stability and reduce subsidence through optimized load transfer, overly aggressive preparation (i.e. over broaching) may compromise proximal femoral bone stock and increase the risk of intraoperative fracture. Furthermore, excessive bone removal may predispose patients to long-term complications such as aseptic loosening. These findings underscore the importance of balancing immediate mechanical stability with preservation of host bone integrity. Future studies should specifically investigate the impact of reaming strategies on proximal femoral bone stock, fracture risk, and long-term implant survival to guide surgical technique optimization.
This review is not without limitations. The included studies consisted primarily of retrospective clinical analyses, biomechanical experiments, and finite element modeling, which are inherently limited by small sample sizes, short-term follow-up, and heterogeneity in implant designs and surgical techniques. Additionally, variability in radiographic measurement techniques and definitions of osseointegration introduces further inconsistency in reported outcomes. The absence of standardized protocols for assessing CCGs limits cross-study comparability and highlights the need for uniform measurement methodologies.
Our analysis revealed that CCGs are a prevalent postoperative occurrence that often resolve through bone remodeling. However biomechanical studies have demonstrated that the presence of a gap compromises rotational stability, increases susceptibility to periprosthetic fracture, and leads to greater subsidence compared to stems with direct calcar contact.
Conclusion
CCGs are common following total hip arthroplasty. Although many of these gaps close over time through osseous remodeling, biomechanical evidence indicates that the benefits of collared femoral stems depend heavily on immediate direct contact with the calcar. When contact is achieved, rotational stability improves, and both subsidence and fracture risk decrease. In contrast, when a gap persists, collared stems exhibit biomechanical behavior similar to collarless designs. Accordingly, preventing CCGs appears important for maximizing early implant stability, while careful surgical technique is required to balance this goal against the risk of compromising proximal femoral bone stock.
Author Contributions
Sandeep Yanamala: Data curation, formal analysis, investigation, visualization, writing original draft, writing- review and editing. Rakan Alshaibi: Data curation, formal analysis, investigation, visualization, writing original draft, writing- review and editing. John Kelly: John Kelly: Validation, investigation, writing- review and editing. Christopher Nagelli: Validation, investigation, writing- review and editing. Michael Taunton: Validation, investigation, writing- review and editing. Mario Hevesi: Conceptualization, resources, data curation, formal analysis, supervision, validation, investigation, visualization, methodology, project administration, writing original draft, writing- review and editing.
Potential COI
SY, RA, JK, and CN have no disclosures
MH: DJO, LLC: Type: Other Professional Activities, Moximed: Type: Other Professional Activities
Type: IP Royalties, Stryker: Type: Other Professional Activities, Journal of Cartilage and Joint Preservation: Type: Editorial or governing board Self
MT: DJO, LLC: Type: Other Professional Activities, Type: Other Intellectual Property, AAOS: Type: Board of Directors or committee member Self, Journal of Arthroplasty: Type:, Editorial or governing board Self
Acknowledgement
We would like to thank the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32 AR56950)