Introduction
Total knee arthroplasty (TKA) is considered to be the most effective approach to treat patients with symptomatic knee osteoarthritis (OA) who failed conservative treatment.1 Improved function , pain relief and cost effectiveness are all attributed to choosing TKA as the mainstay management of end stage OA.2 Total knee arthroplasty can be done either manually or robotically , which has become more popular nowadays.
For many years, conventional TKA has been the technique of choice when managing OA due to proven effectiveness and replicability.3,4 However, many patients have complained of dissatisfaction with their outcomes which can be related to factors such as implant placement and soft tissue balance.5,6 Moreover , patients with more complex conditions may not have as much precise component alignment when undergoing conventional TKA.7
A potential solution for alignment precision and improved soft tissue balance is using robotic knee arthroplasty technology.8 In the late 1980 robotic surgeries were introduced to orthopedics , with ROBODOC ( integrated surgical systems , Davis, CA ) being one of the systems used in hip arthroplasty initially and then integrated in over 15000 robotic TKA’s worldwide.9–11 When preparing for a Robotic-assisted TKA, some softwares needs a three-dimensional 3D implant templating and a Computed tomography CT of the intended limb preoperatively . This has resulted in reducing both surgical time and costs as well as accurately predicting the size of implant leading to satisfactory outcomes.12 In one study, it was found that lower incidence of revision surgeries, manipulation under anesthesia, and opiates consumption were associated with undergoing Robotic-assisted TKA’s in contrast to the conventional TKA’s.13 However, in another study, they had some concerns about how robotic-assisted TKA’s can not assure improved accuracy or reduced rate of postoperative complications.14–17 Thus , more research is needed to clarify this conflict.
As both convential TKA (CTKA) and robotic-assisted TKA (RTKA) have been proven to be effective in managing end-stage OA, short- and long-term outcomes may vary depending on multiple factors. In this study we aim to compare the outcomes of both CTKA and RTKA performed in a special population as bilateral staged TKA by a single surgeon.
Materials and Methods
The study was conducted at a tertiary center, performed by a single senior arthroplasty surgeon. All patients who underwent bilateral staged TKA were included in the study, RTKA and CTKA were performed in the same patient.
In this study, mechanical alignment was achieved using both the measured resection and gap balancing surgical techniques, utilizing the medial parapatellar approach. All patients received spinal anesthesia, pre-operative antibiotics as part of preoperative preparations. Tranexamic acid was administered based on the weight, and intra-articular local anesthesia was given during the surgery. Finally, post-operative adductor canal block and three doses of antibiotics postoperatively. Regarding the types of implants used, Journey II system was used with CORI robotic system and Triathlon system used with MAKO robotic system.
The study design was a retrospective cohort study, and the sample size consisted of all patients (n=19) who underwent bilateral staged TKA in which one of them is utilizing RTKA and the other one is conventional TKA. by a single surgeon from January 2022 until May 2024 at a single tertiary center. A non-probability consecutive sampling technique was used, including all patients who met the inclusion criteria.
Data were collected using a data collection sheet after identifying patients who fit the research criteria. Patients’ information were collected from the electronic health records of the orthopedic surgery department. The data were first entered into an Excel sheet (Microsoft, Redmond, WA, USA) and then analyzed using the Statistical Package for Social Sciences version 29.0 (IBM-SPSS; Armonk, NY, USA).
After data was entered on the excel sheet, data management and analysis was carried out using the Statistical Software for Social Sciences (SPSS) version 29. A comprehensive statistical analysis was conducted on the dataset, encompassing both descriptive and inferential methodologies. A descriptive analysis is conducted to summarize the demographic characteristics of the patients, which include age, gender, and other features. Moreover, the Chi-Square Test and Fisher’s Exact Test is used to the association between categorical variables. Subsequently, the Independent Sample T test is used to find the difference between continuous variables. All statistical analyses are executed using IBM’s SPSS Software, version 29.0.0.
Patients’ consents were not required due to the retrospective nature of this cohort study. All data were kept confidential, and patients’ privacy were assured. No identifiers were collected, and all copies were kept in a secure place within the center’s premises. Data access was restricted to the study group members.
Results
Our study included 19 patients with 38 knees with predominantly female cohort, with 16 female patients (84.2%) and 3 male patients (15.8%) (Table 1). The average age of the patients was 64.6 years (SD = 7.1), with a range of 49 to 75 years. The average body mass index (BMI) of the group was 33.7 kg/m^2 (SD = 3.9), ranging from 24.8 to 40.3 kg/m2.
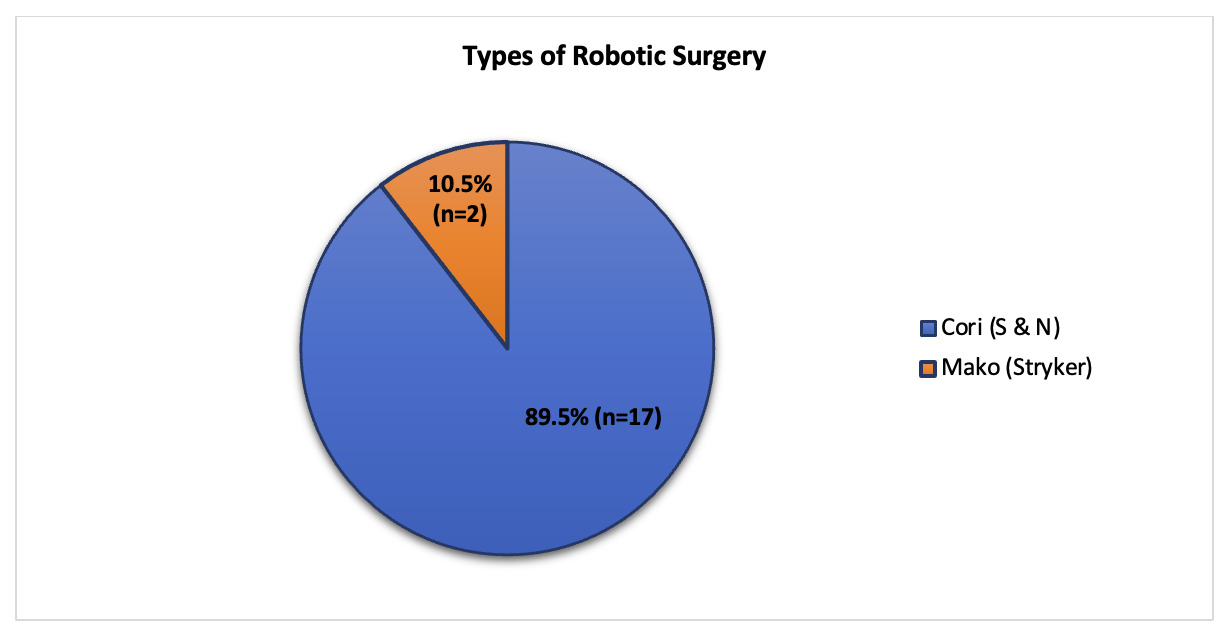
Table 2 shows descriptive statistics for various features, management, and outcomes for 38 knee surgeries, equally divided between robotic (50.0%, n=19) and conventional methods (50.0%, n=19). Among the robotic surgeries, the Cori system by Smith & Nephew was used in the majority of cases (89.5%, n=17), while the Mako system by Stryker was used in a minority (10.5%, n=2) (Figure 1). All surgeries utilized a medial parapatellar approach and spinal anesthesia (100%, n=38). and no surgical drains were used (100%, n=38). Blood loss was predominantly 100 ml (89.5%, n=34), with lesser occurrences of 150 ml and 200 ml losses (5.3% each, n=2 for both). The estimated operative time averaged 93.3 minutes (SD=16.9), ranging from 70 to 130 minutes. No pre-operative or intra-operative blood transfusions were reported (100%, n=38), except for one case that required a post-operative blood transfusion (2.6%, n=1). Tranexamic acid was used intraarticularly in all surgeries (100%, n=38), and most patients did not require narcotics after three weeks (89.5%, n=34).
.png)
Table 3 shows post-operative complications and outcomes for 38 knee surgeries. Only one instance of surgical site infection, urinary tract infection, and acute kidney injury (AKI) were reported, each occurring in 2.6% (n=1) of cases. No Pin site pain was reported. There were no instances of periprosthetic fracture, prosthetic joint infection, or venous thromboembolism. Additionally, there were no readmissions within one month or mortality reported.
Table 4 provides a comparison of different features between robotic and conventional types of Total Knee Arthroplasty (TKA) for 38 knees. Both types show uniformity in several aspects such as the utilization of unilateral knee procedures, anesthesia type (all spinal), approach (all medial parapatellar), and absence of drains, with each having equal distribution (50% each, n=19). The mean operative time was significantly longer for RTKA (105.3 minutes, SD=12.9) than CTKA (81.4 minutes, SD=10.8, p<0.001). Range of Motion (ROM) at discharge showed no significant difference between RTKA (99.2°) and CTKA (98.4°) surgeries, with a p-value of 0.797. Length of hospital stay was also shorter for RTKA (4.2 days, SD=0.7) compared to CTKA (5.6 days, SD=1.9), p=0.006. No significant differences were observed in blood loss, post-operative complications, or narcotic use after three weeks. Both approaches demonstrated comparable outcomes regarding range of motion at discharge and rates of post-operative complications.
Table 5 shows significant postoperative functional improvement in both conventional and robotic total knee arthroplasty (TKA). For the left knee, conventional TKA showed a marked rise in KOOS from 14.18 (3.13) to 85.64 (4.20) (p < 0.001), while WOMAC scores improved from 85.27 (5.53) to 18.91 (3.33) (p < 0.001). Robotic TKA yielded comparable gains, with KOOS increasing from 15.20 (2.25) to 87.00 (2.71) (p < 0.001) and WOMAC decreasing from 84.40 (3.66) to 19.00 (3.97) (p < 0.001). For the right knee, conventional TKA improved KOOS from 16.80 (2.70) to 86.50 (3.60) (p < 0.001) and WOMAC from 84.80 (5.03) to 26.20 (20.55) (p < 0.001). Robotic TKA showed parallel results, with KOOS rising from 16.36 (3.59) to 84.36 (5.18) and WOMAC dropping from 83.91 (5.22) to 18.55 (2.84) (p < 0.001).
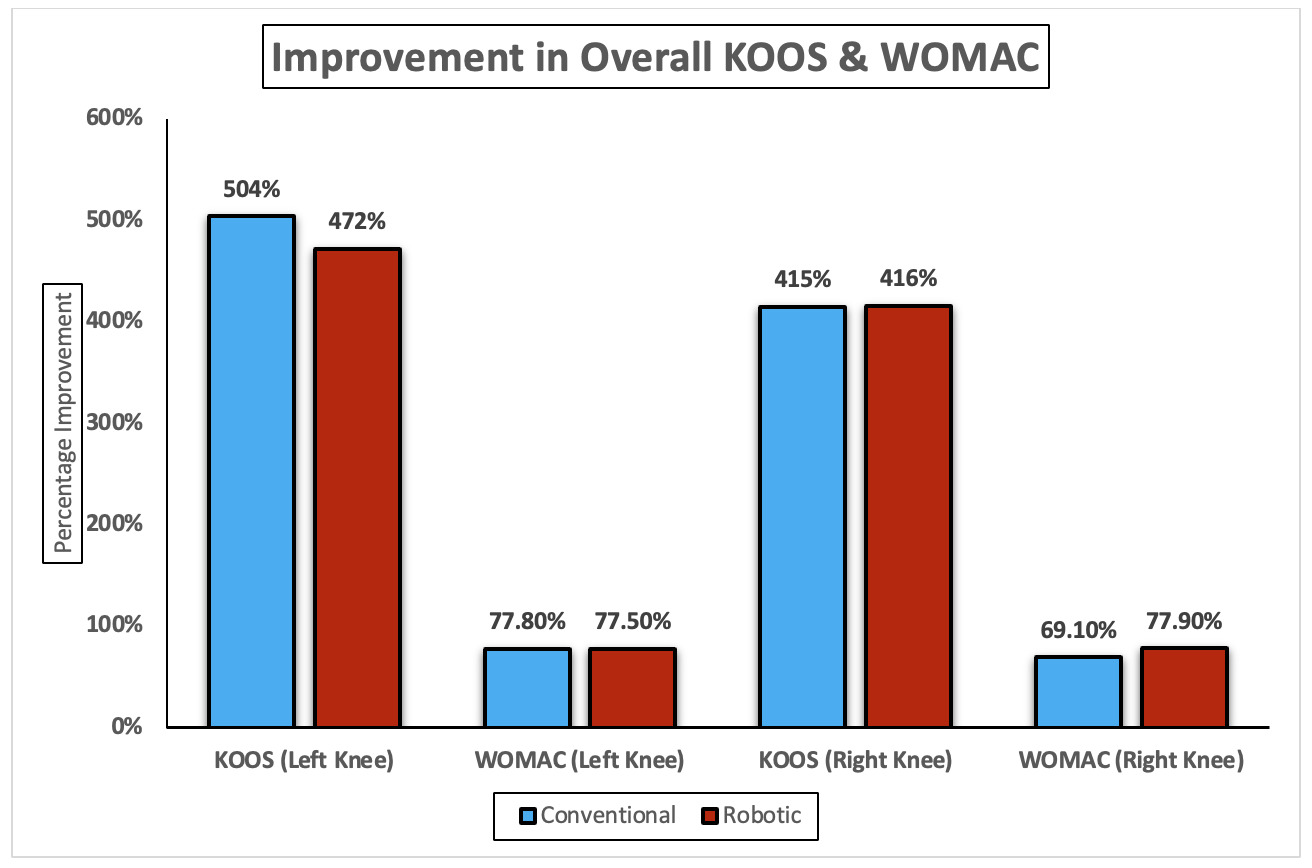
Overall, the improvements revealed that for the left knee, conventional TKA demonstrated a slightly greater gain in KOOS (504%) than robotic TKA (472%), while both achieved nearly identical reductions in WOMAC scores (77.8% vs 77.5%, respectively). For the right knee, both techniques showed comparable KOOS improvement (416% vs 415%). However, in WOMAC reduction, robotic TKA again outperformed conventional (77.9% vs 69.1%) (Figure 2).
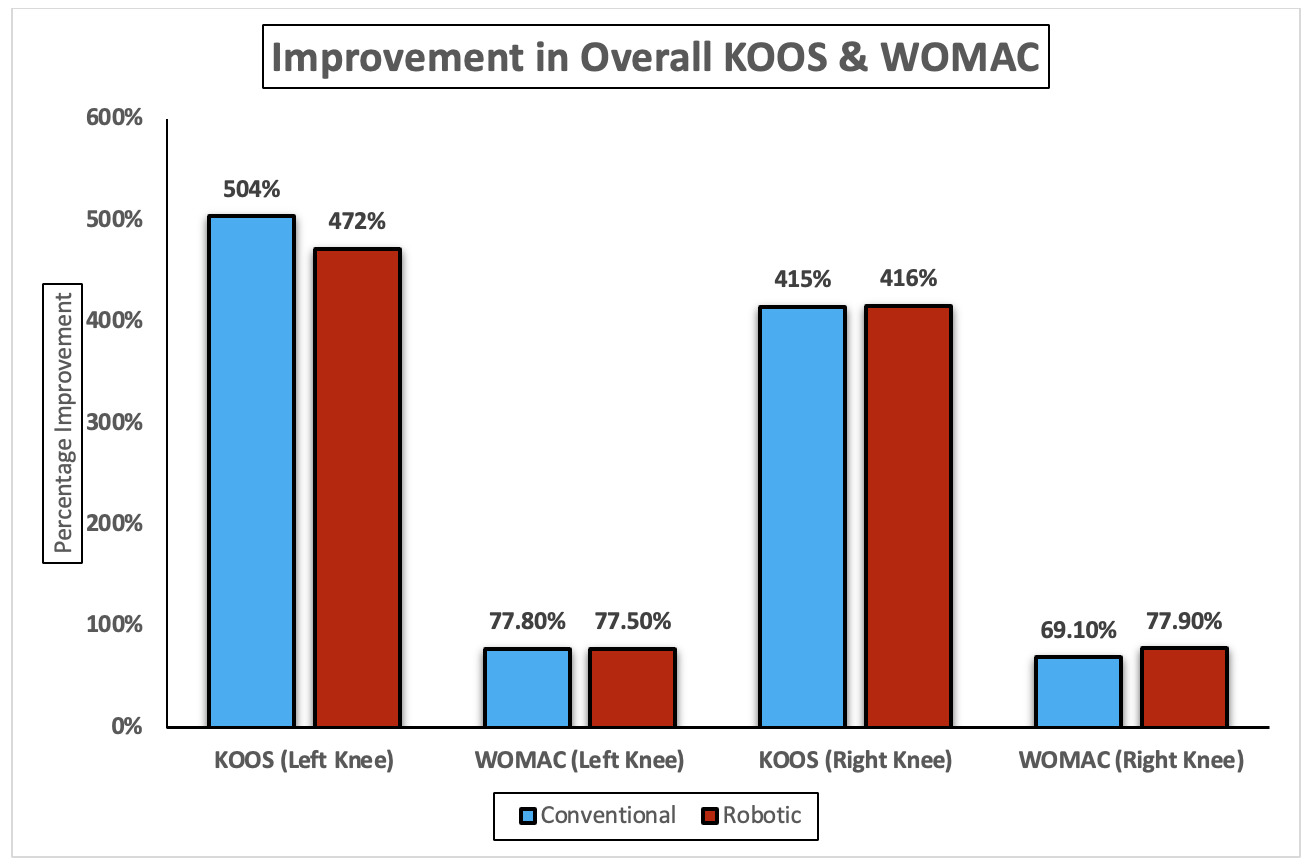
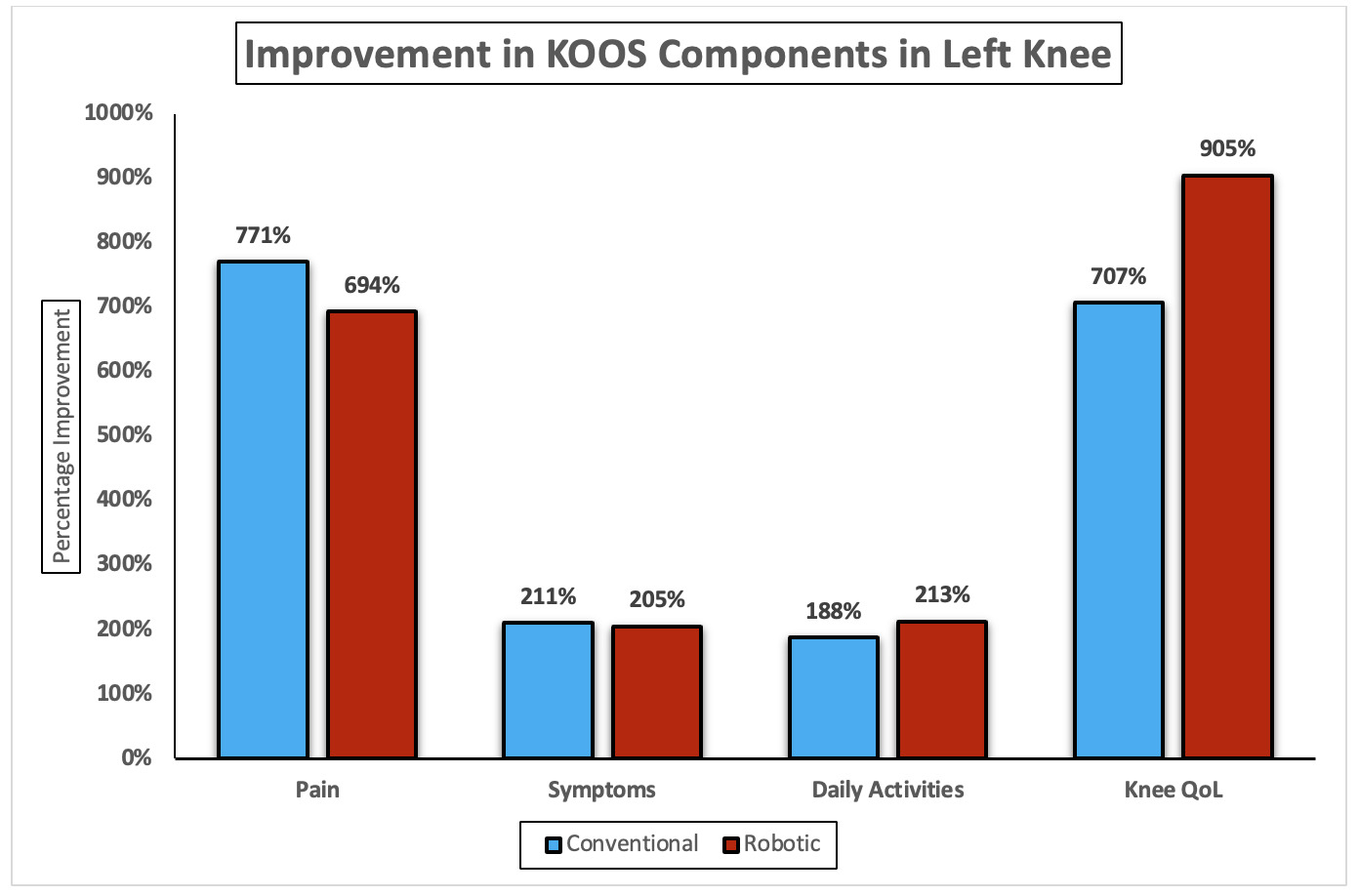
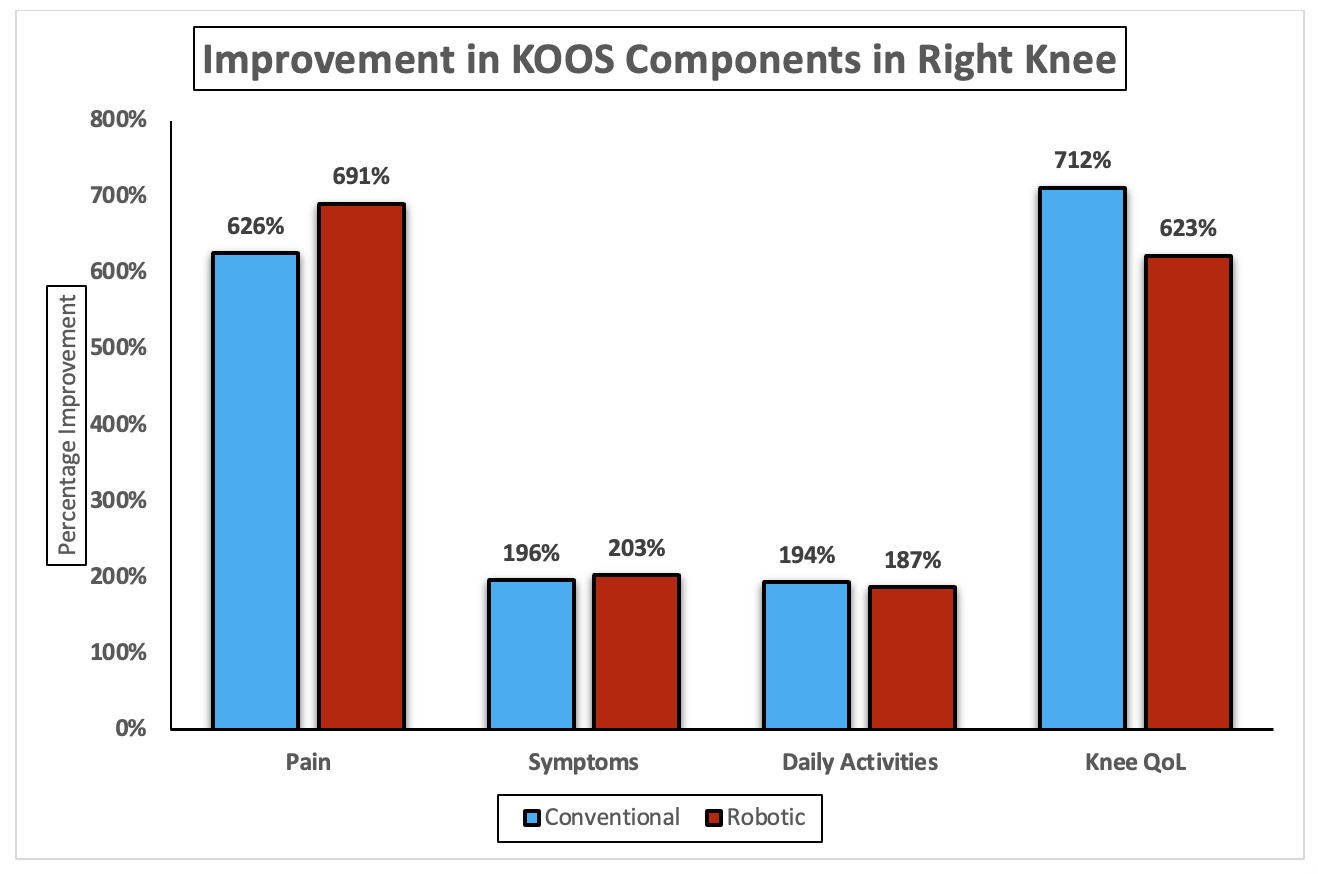
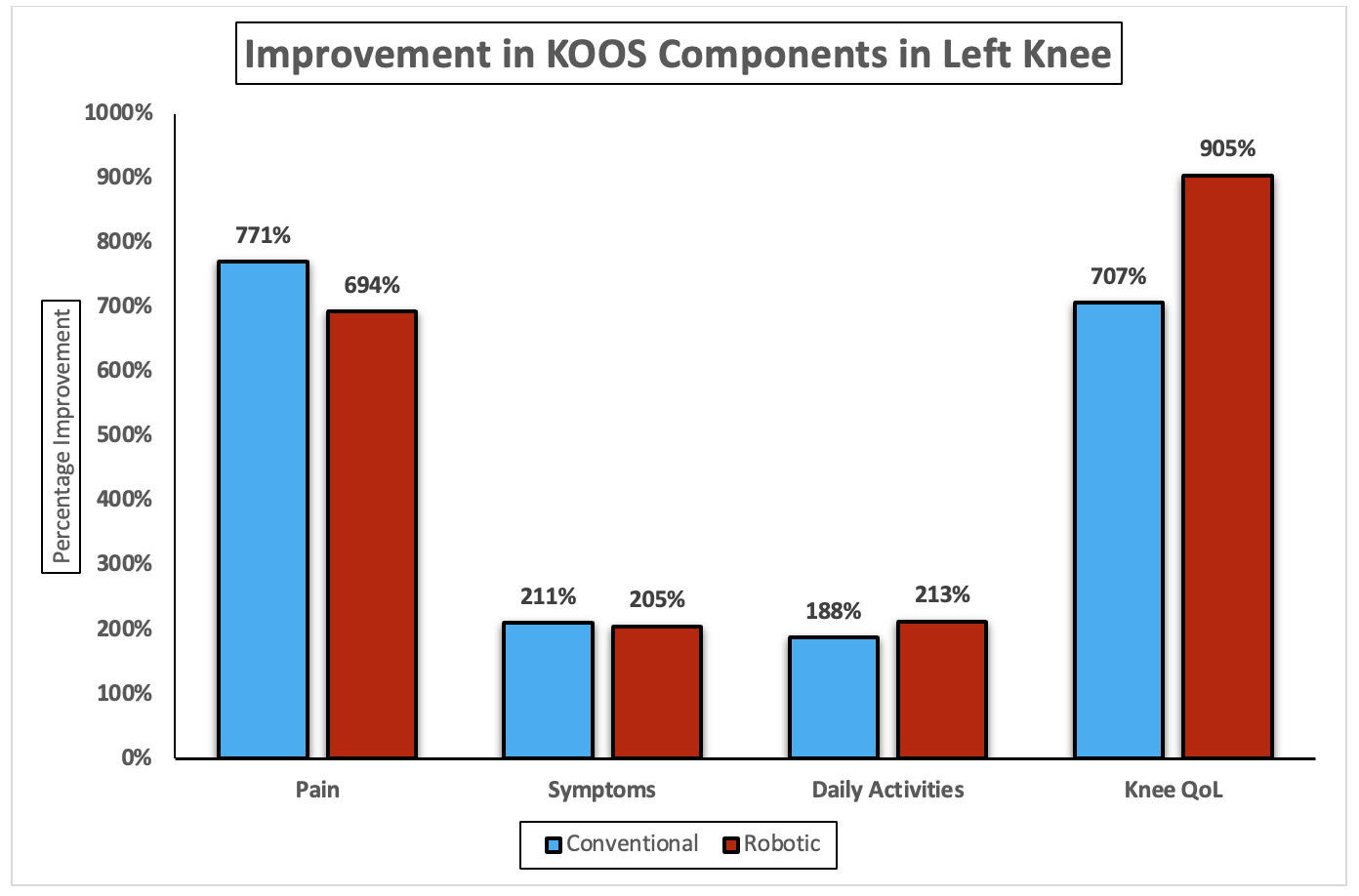
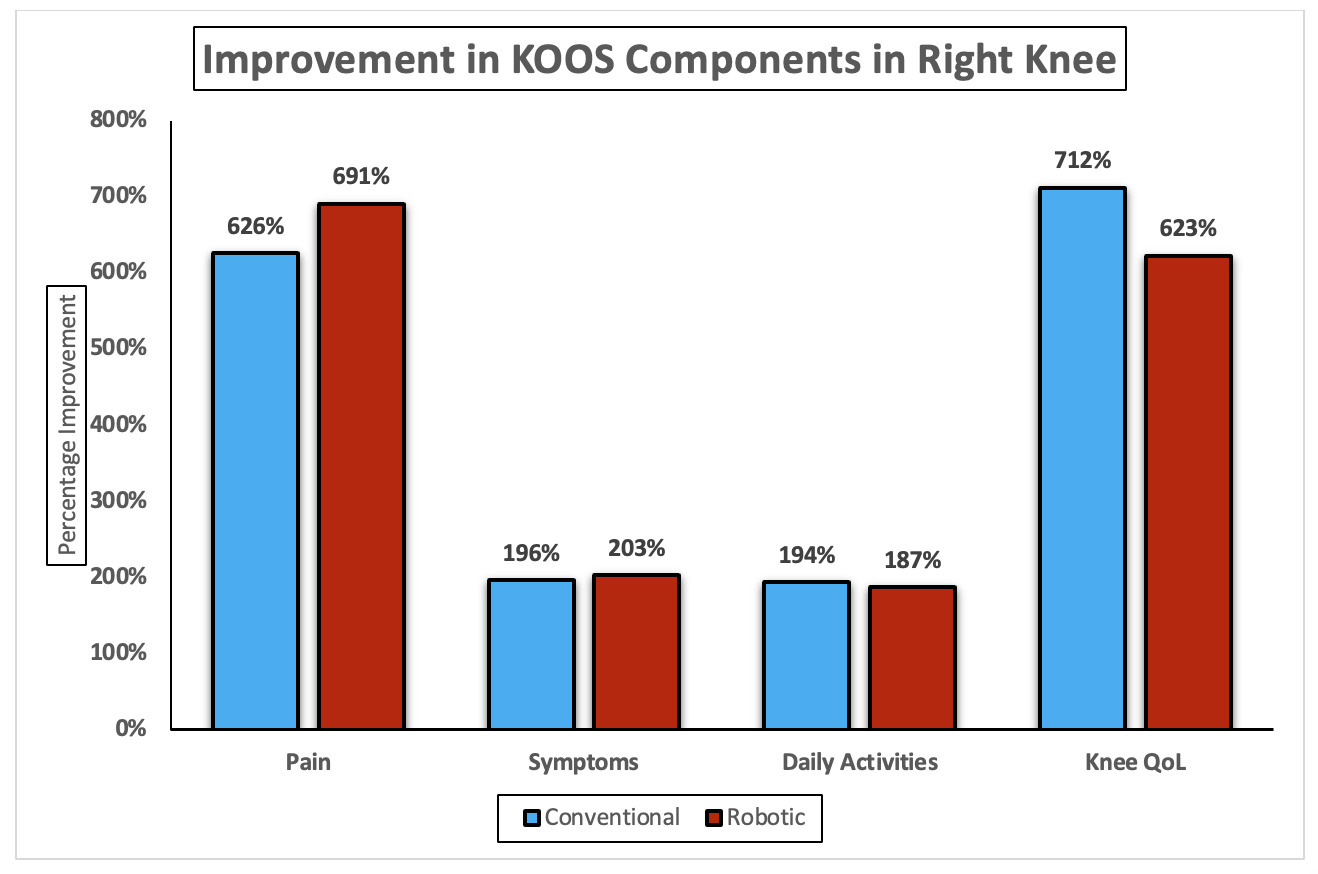
Table 6 shows significant postoperative improvement across all KOOS subdomains in both conventional and robotic total knee arthroplasty (TKA). For the left knee, conventional TKA demonstrated significant improvements in pain, symptoms, daily activities, and knee QoL, all with p < 0.001. Robotic TKA showed comparable postoperative gains across the same KOOS subdomains, also achieving p < 0.001 in all measures. For the right knee, both conventional and robotic TKA resulted in marked improvement in pain, symptoms, daily activities, and knee QoL, each reaching statistical significance (p < 0.001) across all domains. Overall, for the left knee, conventional TKA achieved greater gains in pain (771%) and symptoms (211%), while robotic TKA excelled in daily activities (213%) and knee QoL (905% vs. 707%). For the right knee, robotic TKA showed higher improvement in pain (691%) and symptoms (203%), whereas conventional TKA led in daily activities (194%) and QoL (712% vs. 623%) (Figure 3a & b).
Discussion
Total knee arthroplasty (TKA) is the primary treatment for severe osteoarthritis, offering pain relief and improved function, either through conventional or robotic methods.18 While conventional TKA has been favored historically for its effectiveness, robotic-assisted TKA offers precise alignment and potentially better soft tissue balance.19 Despite its increasing popularity and technological advantages, debates continue regarding its superiority over conventional methods in reducing complications and revision surgeries, necessitating further research to explore these aspects in managing end-stage osteoarthritis. Our study compares outcomes and complications between robotic (RTKA) and conventional (CTKA) Total Knee Arthroplasty approaches.
Notably, our study shows that predominance of females (84.2%), with an average age of 64.6 years, aligning with the global demographic trend where TKA is more frequently performed in older women due to higher rates of osteoarthritis. Similarly, Patel et al. (2020) show that TKA is more prevalent in females (59.1%) than males (40.9%) who underwent TKA.20 The body mass index (BMI) average was 33.7 kg/m^2, indicating a majority of our patient were classified obese, which is consistent with the literature that links higher BMI with increased risk of knee osteoarthritis and subsequent need for TKA.21
Moreover, both surgical approaches were utilized equally in our cohort, with each method applied to 19 knees. This balanced distribution allows a robust comparison of the two techniques. We found no significant difference in several procedural aspects such as anesthesia type and surgical approach, which were consistent across both groups. However, significant differences were noted in the duration of surgery. RTKA procedures had a longer average operative time (105.3 minutes) compared to CTKA (81.4 minutes), a finding that could be attributed to the additional time required for robotic arm setup and calibration. Similarly, Süzer et al. (2023) shows that mean total surgery time was significantly higher in group RTKA than in group CTKA (151.25 ± 24.51 (120-240) minutes vs. 116.72 ± 4.99 (105-125) minutes, P < .001).22 Moreover, robotic assistance improves precision and alignment in surgeries but comes with high costs and requires broader validation, as noted by Sankar et al. (2025).23 Tourniquet use is often debated in TKA due to concerns about pain and vascular complications; however, it remains commonly used in conventional surgeries to reduce intraoperative bleeding and improve visibility.24
The absence of periprosthetic fractures and venous thromboembolism in our study is particularly notable, suggesting effective perioperative management strategies, consistent with findings from other studies that advocate for aggressive mobilization and anticoagulation protocols.25
Notably, the length of hospital stay was significantly shorter for RTKA compared to CTKA, which may indicate faster recovery times associated with robotic-assisted procedures. Kayani et al. (2018) shows that robotic-arm assisted TKA was associated with decreased pain, improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based TKA.26 This could be due to more precise implant placement and potentially less soft tissue damage during surgery. However, our data did not show a significant difference in the range of motion at discharge, suggesting that immediate functional recovery may be similar between the two techniques. Archunan et al. (2021) shows that after conventional TKA mean flexion improved from 55.7 to 93.8 degrees, and mean fixed flexion deformity decreased from 9.5 to 4.1 degrees.27
Our results indicate that pin site pain was exclusive to RTKA, possibly due to the additional fixation points required for robotic arms. Despite this, the overall requirement for narcotics post-operation was not significantly different between groups, aligning with studies suggesting that post-operative pain management should be tailored individually rather than based on the surgical approach alone.28
Furthermore, in term of the functional improvement, our study showed findings which are consistent with the previous literature. Similarly, there is a study by Stoltz et al. (2014) reported that there is a similar significant gains in KOOS and WOMAC scores postoperatively for both TKA approaches.29 Notably, the conventional TKA demonstrated higher improvements in pain and symptoms, while robotic TKA provided slightly better enhancement in daily activities and knee quality of life. There is a study by Mostafa et al. (2025) which showed that RA-TKA offers improved mechanical alignment accuracy compared to C-TKA but does not demonstrate superior short to medium-term functional outcomes.30 However, Kim et al. (2020) shows that at a minimum follow-up of 10 years, there is no differences between robotic-assisted TKA and conventional TKA in terms of functional outcome scores, aseptic loosening, overall survivorship, and complications.31 Overall, the present results align with global evidence that both methods significantly enhance postoperative function, with robotic TKA offering modest but not universal advantages in specific domains.
Limitations
Our study has several limitations including a small, homogeneous sample limiting generalizability, and a focus on short-term outcomes without long-term follow-up. Conducted in a single center without randomization, the findings may not be widely applicable and could be influenced by selection bias. No cost-effectiveness analysis was included, and potential confounders were not fully controlled. Additionally, reporting bias due to funding sources and the novelty of robotic systems necessitates cautious interpretation of the results. Future research should address these gaps to better evaluate TKA methods.
Implications and Future Directions
Our study highlights the precision of robotic-assisted methods, advocating for their adoption and necessitating surgeon training. Future research should focus on long-term outcomes, employ multicenter trials for broader validation, and include economic analyses to evaluate cost-effectiveness. Advancements in technology should aim to reduce costs and enhance usability, driven by clinical feedback. This comprehensive approach will help optimize surgical outcomes and improve patient care in knee arthroplasty.
Conclusion
Our study supports the efficacy and safety of both robotic and conventional knee arthroplasty, with each showing distinct advantages. The choice of technique should consider patient-specific anatomical and clinical conditions, with RTKA offering precision and potentially shorter recovery, albeit with longer operative times and associated costs. Both methods showed the substantial gains in KOOS and WOMAC scores. The robotic TKA slightly outperformed in the WOMAC reduction and specific KOOS subdomains like daily activities and quality of life, whereas the conventional TKA showed marginally greater improvement in pain. Overall, both approaches had provided excellent and clinically meaningful outcomes.
Abbreviations
CTKA – Conventional Total knee arthroplasty.
RTKA – Robotic-assisted Total knee arthroplasty.
KAMC – King Abdulaziz Medical City.
KAIMRC – King Abdullah International Medical Research Center.
BMI – Body Mass index.
TXA – Tranexamic acid.
ROM – Range of motion.
Declarations
This study was approved by King Abdullah International Medical Research Center (KAIMRC) with the following protocol number: NRR24/064/10. The requirement for informed consent was waived due to the retrospective nature of this study.
Consent for publication
Not applicable
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Competing interests
The authors declare that they have no competing interests.
Funding
No funding was obtained for this research.
Authors’ contributions
AT, TM, AAH and ZJ developed the idea and designed the methods. ZJ, KH, AS, AH and GM collected the data. ZJ, KH, and GM analyzed, interpreted, and presented the results. All authors wrote the manuscript. AT, TM, AAH and ZJ critically revised the manuscript for content and finalization. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Acknowledgements
Not Applicable.