Introduction
Globally, falls have a prevalence of 26.5% and are a leading cause of injury related disability and death in the elderly.1,2 With increasing age, patients typically accumulate a greater number of risk factors predisposing them to fragility fractures that are associated with significant morbidity and mortality with proximal femur fractures being among the most common.3 One subset, neck of femur fracture (NFF), is often seen in the elderly suffering from osteoporosis following falls or low-impact trauma. The garden classification is used to further distinguish between non-displaced (types I and II) and displaced (types III and IV) and can also help guide surgical approach.4 There are several surgical options for the management of displaced NFF, namely, open reduction and internal fixation (ORIF) or arthroplasty, which can be further divided into hemiarthroplasty (HA) and total hip arthroplasty (THA).5 For patients younger than 60 years, ORIF is typically utilized whereas patients 80 and over more often undergo arthroplasty.6,7 For patients between 60 and 80, however, internal fixation or arthroplasty may be used.8 The choice of intervention is often based on several factors including the baseline functional status, level of pre-injury activity, bone quality, associated comorbidities and patient/surgeon preferences.9,10 In patients with lower activity levels and significant disease comorbidity, arthroplasty may be preferred due to fewer long-term complications. Such examples include nonunion and avascular necrosis of the femoral head, which can carry a significant risk of increased mortality.5 Conversely, ORIF has distinct advantages, such as shorter operation time, lower blood loss, less extensive soft tissue damage, and lower rates of aseptic loosening.5,11
Another potential advantage ORIF may have over other surgical methods is a lower rate of postoperative DVT. This association could be explained in the context of the shorter operation time, where operation time has been inversely correlated with the risk of postoperative DVT.12 However, there is mixed evidence regarding this outcome, with Fu et al, and Dou et al, finding significantly lower rates of postop DVT in the ORIF group vs the arthroplasty group.13,14 These studies regularly screened patients using Doppler ultrasound at set time intervals postoperatively regardless of symptoms of DVT as well as when there is clinical suspicion and were able to capture asymptomatic DVT. Conversely, a 2020 meta-analysis by Cui et al, found no statistically significant difference between the two surgical interventions and rate of postoperative DVT.15 The studies included within Cui et al, however, examined rates of symptomatic DVT with a total of 8 patients developing DVT across a pooled population size of 875 from 4 studies.
Within the arthroplasty group there may also be an increased risk associated with THA compared to HA. THA carries on average longer operation time and has also been associated with a greater duration of hospitalization and greater blood loss.16 All of which are risk factors for the development of DVT.17,18 Despite this, previous research has not found any significant difference in the rates of postoperative DVT between these two interventions for the treatment of NFF.19
The rate of postoperative DVT across all interventions differs significantly between the existing literature notably, Fu et al, 56%, Dou et al, 8% and Cui et al, 0.91%.13–15 Part of this variation can be explained by the differing methods used to capture DVT and the differing outcomes of symptomatic DVT and asymptomatic DVT. However, there is still significant variation even when comparing literature with similar methodology and outcomes.13,14
One limitation of the existing literature is limited follow up after surgery. Previous research has established that the rate of postoperative DVT, although often presents within the first few weeks postoperatively, risk remains elevated for up to 3 months after surgery.20–22 Capturing DVT after discharge can be difficult due to various factors including limited follow up and typically a lack of an integrated EMR system across multiple facilities. In the state of Qatar, patients above the age of 60 with NFF are cared for by an ortho-geriatric co-care team at Hamad General Hospital. Patients are typically admitted under the orthopedic team but are concurrently followed by geriatrics, whose roles include medical stabilization, optimization for surgery, prevent complications, geriatric syndromes management, medication review, anticoagulation… To our knowledge, this is the first study exploring this outcome within an Ortho-geriatric co-care program globally.
Upon admission, the admitting physician completes an VTE risk assessment workflow which is then entered into the patient chart. Patients receive VTE prophylaxis in the form of a pneumatic compression device as-well as pharmacologic anticoagulation, either a direct oral anticoagulant (DOAC), typically a factor Xa inhibitor such as Rivaroxaban, 10mg, once daily, low molecular weight heparin (LMWH) either Enoxaparin, 40 mg or Dalteparin, 5000 IU, Unfractionated Heparin (UFH), 5000 IU, twice daily or Warfarin, target INR 2.0-3.0.23 Pharmacologic anticoagulation is typically started 12 hours after anesthesia and continued for 28-30 days. Upon discharge, patients taking UFH are switched to LMWH or DOAC.
Once cleared by the ortho-geriatric team, patients are typically discharged home or to the Qatar rehabilitation institute, in either case they continue to have regular outpatient follow up with the orthogeriatric care team and are examined for signs of DVT at each visit. Patients who present with symptoms of DVT, namely, development of pain, warmth and swelling in one or more extremities undergo deep venous Doppler ultrasound for the presence of an intraluminal filling defect.24 Additionally, patients who present with findings concerning for pulmonary embolism are also evaluated, with pulmonary angiography and if positive, doppler ultrasound for concurrent DVT. If evidence of a DVT/PE is found, patients are subsequently started on therapeutic doses of anticoagulation, for a duration of 3 months. Our patient population has experienced acute trauma, is undergoing orthopedic surgery and therefore DVT in this cohort can be classified as transient provoked DVT for which 3 months of anticoagulation is indicated.25
These services are part of the wider Hamad Medical Corporation (HMC), the largest healthcare provider in Qatar. HMC facilities include multiple hospitals and a large number of primary care centers providing approximately 90% of all acute services in the country and serves a large ethnically diverse urban/suburban population.26 All patient interactions are entered into a combined cross-facility EMR, allowing researchers to track patient visits for adverse outcomes following discharge across an number of facilities.
Given the relative paucity of studies on this topic, limited follow up time and wide variation in rate of postoperative DVT, further research is required to establish the differing rates of postoperative DVT among the various surgical interventions. We hoped to explore this association further with the added advantage of being able to assess the development of postoperative DVT for an extended period after discharge. We hope that this may be used to guide the choice of surgical intervention with patients who have a greater risk of DVT for elderly patients undergoing NFF.
Materials and Methods
Ethical Considerations
The following study was reviewed by the Weill Cornell Medicine–Qatar institutional review board and granted exempt status. The present study was also reviewed by the Medical Research Centre at Hamad Medical Corporation and additionally granted exempt status. Data was collected from patient records, all identifiable data removed and stored on a password protected excel sheet located and stored on Hamad Medical Corporation premises. At the end of the data collection period the anonymized data was then shared in a limited capacity with statisticians at Weill Cornell Medicine–Qatar for assistance with data analysis.
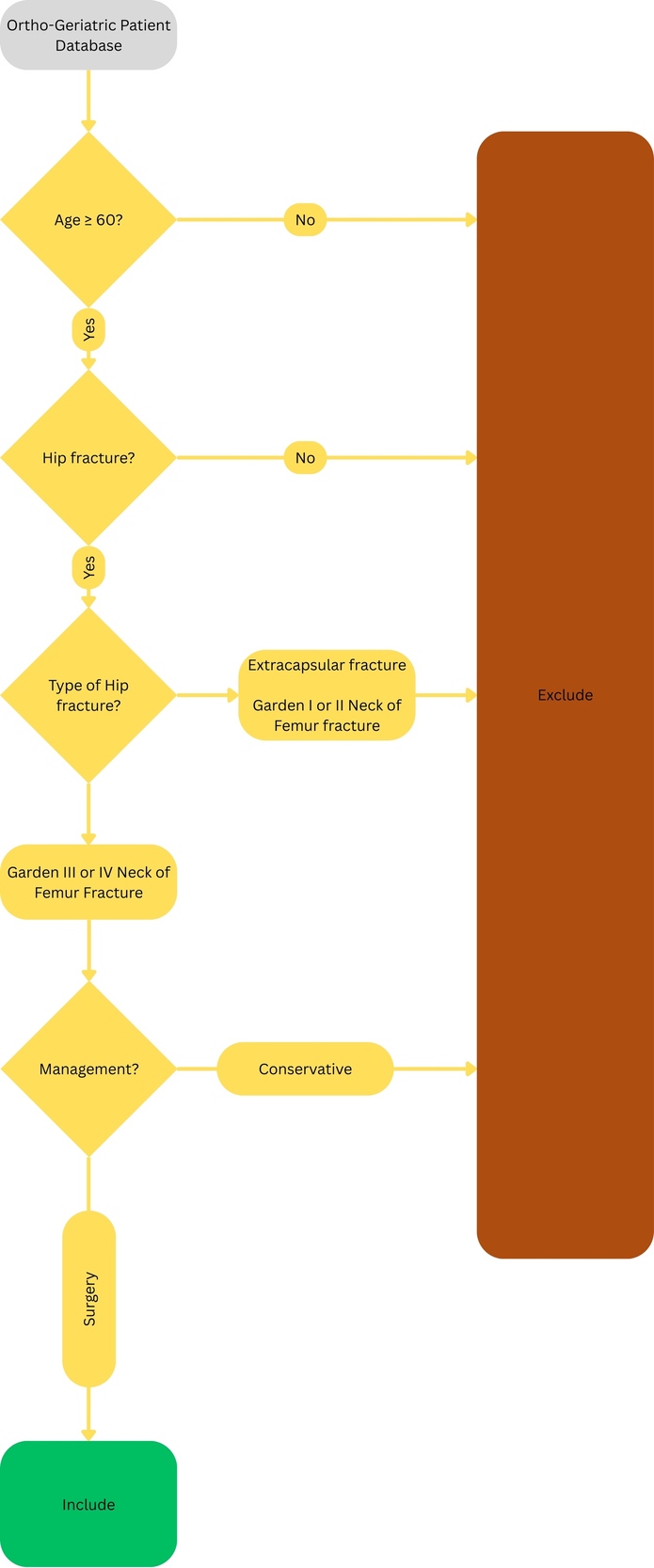
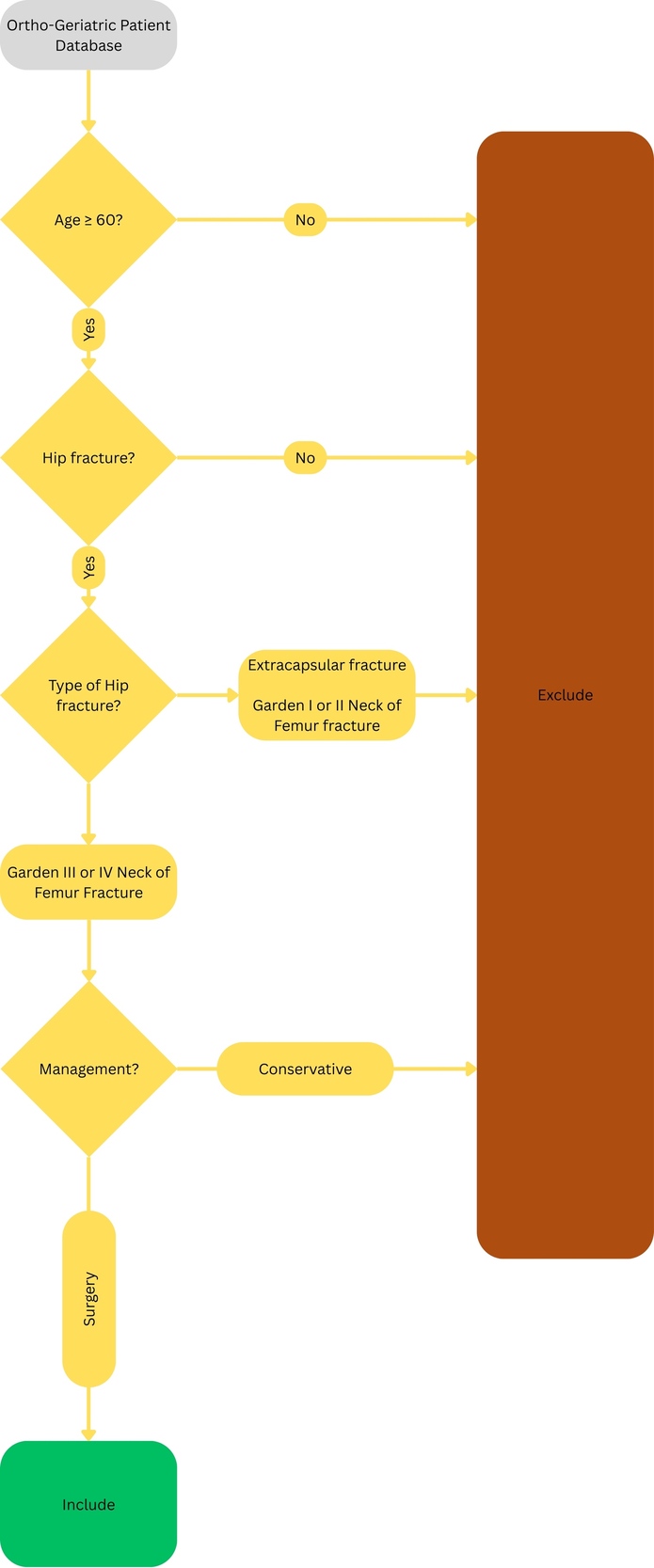
This study is a retrospective cohort analysis of patients who underwent surgical management of NFF within the orthogeriatric co-care program of Hamad General Hospital. Patient records stored on the electronic medical database of the orthogeriatric co-care program were searched between 1/2020-5/2023 for patients who met the criteria for inclusion in the study. Patients were included if they were: a) 60 years or older, b) X-ray confirmation of displaced (Garden III or IV) neck of femur fracture and c) underwent surgical intervention for neck of femur fracture. Patients were excluded if they were: a) 59 or younger, b) X-ray evidence of extracapsular or femoral head fracture or nondisplaced (Garden I or II) neck of femur fracture, c) were managed conservatively without surgical intervention (Figure 1).
Included patients had the following demographic and clinical characteristics recorded: type of surgical intervention, gender, age, nationality, body mass index, smoking status, diabetes mellitus, hypertension, history of clotting disorder, history of VTE, osteoporosis, immobility, whether they take medications like antihypertensives, antidiabetics, bisphosphonates, proton pump inhibitors, anticoagulants, antiplatelets and other medications*.* Patient nationality was categorized into Qataris and non-Qataris. The clinical characteristics recorded were selected based on established association with DVT and factors that may have influenced the choice of surgery. Patient medical records were searched for up to 3 months postoperatively for the development of DVT at subsequent outpatient follow-up visits or emergency department visits.
Following the collection of the above, patients were grouped by surgical intervention (ORIF vs arthroplasty) and demographic and clinical characteristics were compared between the two interventions using Pearson Chi square or Fishers exact test for categorical variables and T-test or Mann Whitney U-test for numeric variables. Postoperative DVT rates were compared between ORIF and arthroplasty. The analysis described was then repeated comparing ORIF, HA, and THA
Results
Overall, 161 patients underwent surgical treatment for femoral neck fracture, with 27 patients undergoing open reduction and internal fixation while 134 patients underwent arthroplasty. Non-Qataris made up the largest ethnic demographic, 61% (n=98), while 39% (n=63), were Qatari (Table 1). Qataris were significantly more likely to undergo arthroplasty, 94%, compared to 77% of non-Qataris who had a much higher rate of ORIF, 24% vs 6% in Qataris. Patients on average were overweight with a mean BMI of 27 ± 5.3 (Table 1). The gender distribution was evenly split between females (n=81) and males (n=80), while the mean age of the cohort was 74 ± 8.3 (Table 1). A majority of patients in the population had diabetes (63.4%), and/or hypertension (81.4%).
Comparing ORIF vs arthroplasty, patients differed in age, nationality and number of antihypertensives (Table 1). All other variables were found to not differ significantly between the two interventions. Across all interventions, 3 patients developed deep venous thrombosis, with 2 among arthroplasty patients (1.4%) and 1 among ORIF patients (3.7%). This difference was not found to be statistically significant (p>0.05).
Among patients undergoing arthroplasty, 129 (96.3%) underwent hemiarthroplasty while 5 (3.7%) underwent total hip arthroplasty (Table 2). All cases of postoperative DVT were among the hemiarthroplasty group. The analysis was repeated to compare the three surgical interventions, ORIF vs HA vs THA. Nationality differed significantly between the three interventions, and none of the other variables were found to be significant. There was no statistically significant difference in rates of postoperative DVT among the three surgical interventions (Table 2).
Discussion
Across all interventions, 3 patients undergoing surgery for neck of femur fracture developed postoperative DVT, 1.6% of the population. All three patients within our study developed DVT within 1 week of surgery and while hospitalized. A total of 31 patients presented with symptoms concerning DVT and underwent doppler ultrasound with negative findings. Sorting by surgical intervention, 134 patients underwent arthroplasty with 2 developing DVT, a rate of 1.5% while 27 underwent ORIF, and 1 developed DVT, a rate of 3.7%. This difference was not statistically significant (p>0.05). Based on a power value of 80%, a minimum of 821 patients within each study arm would be required to detect a statistically significance difference, as a result we can infer that our study was significantly underpowered.
The rate of postoperative DVT within our study lies squarely within the 0%-3.4% reported in the literature for postoperative DVT after orthopedic surgery.27 In addition, our findings are also comparable to Cui et al, who found a postoperative DVT rate of 0.91% across all interventions and no statistically significant difference in the rate of postop DVT between ORIF and HA patients.15 The studies included within Cui et al’s analysis did not detail how DVT was diagnosed.28–31 However, given the lack of a protocol to detect asymptomatic DVT, it is likely that Cui et al’s result is reflective of a pooled rate of asymptomatic DVT, which may explain the concordance with our results.
In contrast, both Fu et al and Duo et al, incorporated a predefined protocol to detect asymptomatic DVT.13,14 In both studies, all patients were screened for DVT using Doppler ultrasound approximately 3-5 days post-surgery as well as when clinical suspicion for DVT arose. As a result, these studies were able to capture asymptomatic DVT in addition to symptomatic DVT, with most cases being diagnosed after pre-scheduled ultrasound and not as a result of patient symptomatology, likely explaining the higher rates of DVT reported by Fu et al, 56% and Duo et al, 8%. Furthermore, among the 3 patients within our study who developed DVT, 2 also developed pulmonary embolism (PE) and were brought to clinical attention as a result of PE symptoms. The rate of DVT reported within our study, therefore, represent symptomatic DVT with the rate of asymptomatic DVT within our population likely being significantly higher.
Fu et al additionally found that 37.5% of ORIF patients developed DVT compared to 58.6% of HA and 75% of THA patients.13 The authors attributed this variation in results to several factors including age, where ORIF patients had a mean age of 55, compared to 68 and 77 for THA and HA groups, respectively. Age also differed significantly between the ORIF and arthroplasty groups within our study, 71 ± 7.7 vs 75 ± 8.3 (p<0.05), however, our cohort was older as we excluded all patients under 60 years of age. Duo et al found that the rate of DVT was 3.4% among ORIF patients compared to 17.4% of Arthroplasty patients and this difference was statistically significant.14 Further analysis of the factors which may have contributed to this difference was not carried out however the authors asserted that the increased rate of DVT in arthroplasty was likely due to the longer operation time relative to ORIF.
In addition, the prevalence of DVT reported within our study may have been impacted by the ortho-geriatric co care model. In this model the geriatrics team performs several measures in order to mitigate the development of DVT, such as; daily rounds reviewing and adjusting anticoagulation, early mobilization, adequate hydration and regular outpatient follow up with anticoagulation review. It is difficult to determine, however, whether this model had any preventative effect within our study as the rate of DVT we observed is similar to previous literature that did not include an orthogeriatric co care team.
No difference in rates of postoperative DVT were found when comparing THA vs HA and ORIF. Due to the extremely small number of patients that underwent THA within our patient population, it is difficult to draw any meaningful conclusions about differences in rates of postoperative DVT between HA and THA. However, previous literature on this topic has similarly failed to find any significant differences between these two interventions and postoperative DVT.
Nationality was found to differ significantly between the surgical interventions, with over 90% of Qatari patients undergoing arthroplasty while Non-Qataris were significantly more likely to undergo ORIF. One possible explanation for this finding may be that Non-Qatari patients likely accounted for a larger proportion of non-residents particularly during the 2022 Qatar World Cup and hence may have opted for greater preservation of the hip joint while abroad. The high rate of arthroplasty among Qataris likely contributed to the disproportionate number of patients undergoing arthroplasty vs ORIF.13,19
Limitations
Our study has a number of limitations. Firstly, the population size for our study was significantly lower than anticipated, 161 compared to the approximately 300 patients we anticipated would meet inclusion for our study. This was largely a result of patients with intertrochanteric fracture being included in the same database as those with NFF resulting in an original overestimation of eligible patients.
In addition, there was a major skew within our study of patients undergoing HA, 80%, compared to 17% undergoing ORIF and only 3% of patients underwent THA. The lopsided distribution may have resulted in our study being underpowered and may have affected the results observed. This may be due to the relatively older age of our cohort and exclusion of patients younger than 60 leading to surgeons and patients preferring arthroplasty over ORIF consistent with guidelines for older patients.9 In addition, Qatari patients were far more likely to undergo arthroplasty potentially as a result of permanent residency status.
Furthermore, although patients were followed up after discharge and access to all subsequent emergency visits was available to investigators, we could not account for patients who sought care at private hospitals or received medical treatment outside the country.
Lastly, our study recorded rates of symptomatic DVT, whereas previous literature which had found differences in the rate of DVT between ORIF and Arthroplasty, measured asymptomatic DVT. This discrepancy makes it difficult to directly compare the results of our study and that of the literature.
In this cohort of elderly patients with displaced femoral neck fractures managed within an ortho-geriatric co-care program, the overall incidence of postoperative DVT was low across all surgical interventions. While numerically higher rates were observed among patients treated with ORIF compared to arthroplasty, this difference was not statistically significant. These findings suggest that both approaches can be performed safely within the context of standardized perioperative thromboprophylaxis. Nonetheless, given the small number of observed events, further multicenter studies with larger patient populations are warranted to more definitively assess potential differences in thrombotic risk between surgical techniques.
Conclusion
In summation, the present study found no statistically significant difference in the rates of postoperative DVT among patients undergoing ORIF, HA, and THA. Our study was likely limited by the small population size and the relatively low percentage of patients undergoing ORIF or THA. Although studies exploring asymptomatic DVT have established ORIF as a protective factor in NFF patients, this association has not been observed in symptomatic DVT. The rates of postoperative DVT observed in our study were consistent with prior studies into this topic. Additionally, the rates observed may have been impacted by the utilization of the orthogeriatric co-care model. Ultimately, however, larger, multicenter studies exploring the development of symptomatic DVT are required. Given the low incidence of symptomatic DVT following NFF surgery, future studies should employ a large sample size of approximately 870 patients within each study group in order to reasonably detect a 5% absolute difference in surgical method. In addition, there should be an adequate number of patients receiving each type of surgery, so study results are not skewed toward 1 intervention. Finally, future projects should also have the ability to reasonably capture subsequent development of DVT for a period of 3 months after discharge.
Author Contributions
MM, JP and MJ conceived of the project. JP, MJ and AM developed the methodology utilized within the present study. MJ performed data collection, BS, JP and AM oversaw the data collection process. MJ and BS performed data analysis. MJ and MM performed data interpretation. MJ, MM, JP, HA and NM wrote and prepared the manuscript. All authors reviewed the results and approved of the final version of the manuscript.
Disclosures
The authors declare they have no conflicts of interest pertaining to the present study.